9
Tinnitus Activities Treatment
Activities treatment is an extension of our earlier work on information counseling, providing information to the patient about tinnitus and associated problems, considering the patient’s overall well-being, and suggesting appropriate coping strategies (Tyler and Babin, 1986; Tyler and Baker, 1983). In most situations we combine activities treatment with partial masking sound therapy (e.g., Stouffer and Tyler, 1990; Tyler et al, 1989). We strongly believe it is important to consider “all the patient’s difficulties, not only an isolated problem” (Tyler and Babin, 1986, p. 3215). For example, we and others have realized the importance of reassuring patients that tinnitus was not an indication of a life-threatening disease, and educating them about the high prevalence of tinnitus in the general population (Stouffer et al, 1991). We recommend the use of a tinnitus problems questionnaire (Tyler and Baker, 1983) as part of a counseling program to determine the issues that are especially important to the patient (see also Chapter 1 in this book). This “represents an excellent opportunity for the patient to consider the problems that he or she attributes to tinnitus” (Tyler and Baker, 1983, p. 153).
Early work that has influenced our counseling includes landmark studies by Richard Hallam and colleagues (e.g., Hallam, 1989; Hallam et al, 1984; Hallam et al, 1988). Other important and influential work is that of Sweetow (1984), Coles (1987), and Coles and Hallam (1987). The significant contributions of Peter Wilson and colleagues (Henry and Wilson, 2001, 2002; Wilson et al, 1998) have been immensely helpful in organizing our overall plan and providing excellent examples of treatment goals and patient interactions. The summary of clinical techniques recommended for audiologists by Flasher and Fogle (2004) also has been helpful.
Tinnitus Partial Masking Therapy
Although not a focus of this chapter, we often include sound therapy, particularly tinnitus partial masking therapy, with this counseling package. Since the early 1980s, we have been using noise to partly mask tinnitus so that both the tinnitus and the noise are heard (see Bentler and Tyler, 1987; Tyler and Babin, 1986, Tyler and Bentler, 1987). Our general sound therapy strategy remains the same, in that we “urge the patient to use the lowest level masker that provides adequate relief” (Tyler and Babin, 1986, p. 3213). Sound therapy is not used with all patients, and when it is used, we do not insist that the noise be present all the time. Hearing-impaired people often experience difficulty hearing in noise (e.g., Tyler et al, 1983), and there may be some situations where they prefer hearing better over the partial relief of tinnitus provided by noise. We also caution that frequent changing of the noise levels may call attention to the tinnitus. Selecting a single, low-level noise is preferable. Recently, we have been using soft background music in place of background noise with some patients (see also Chapter 11).
Patient Expectation Nurturing
We have discussed in some detail the importance of providing a positive outlook for the patient (Tyler et al, 2001). The areas that are relevant to tinnitus treatment in nurturing patient expectations include:
• Being perceived as a knowledgeable professional
• Being sympathetic
• Demonstrating an understanding of the problem
• Having a clear therapy plan
• Sincerely caring about the patient
• Providing feelings of mastery
• Providing hope for the patient
Picture-Based Counseling
In 2001, Tyler and Bergan introduced the concept of picture-based counseling for tinnitus patients. For each counseling session and topic, we produced a series of illustrations that we show to the patient. We believe this approach is helpful because
• The session proceeds in an orderly fashion.
• The clinician does not overlook important concepts.
• It is easier for the patient to understand concepts.
• The treatment can be easily used by other clinicians.
• In studies comparing tinnitus treatments, it is easier to control counseling across conditions and therapists.
Discussions can be adapted to the needs and sophistication of each patient.
Activities Treatment
Our experience in treating tinnitus patients and our discussions with other experts led us to group the problems faced by tinnitus patients into four broad categories:
• Emotional well-being
• Sleep
• Concentration
Impairments in these areas can lead to additional social and work problems. We believe that a complete treatment plan should address all of these categories. Any area not of concern for the patient can be omitted from counseling. The counseling provided in each of these areas is described in more detail later in this chapter.
Components of Tinnitus Activities Treatment
There are three main components of tinnitus activities treatment, which are integrated with each other. These components are informational counseling, activities engagement, and sound therapy (when needed).
Determining Which of the Four Activities to Treat
Because not all patients will require treatment in all four activities categories, we initially determine which areas require treatment. To assist in this, we administer the Tinnitus Activities Questionnaire (Fig. 9–1). This questionnaire produces a score in each of the four areas (emotional well-being, hearing, sleep, and concentration) and, in conjunction with input from the patient, an overall treatment plan can be devised.
When designing questionnaires, we prefer a scale from 0 to 100. This provides better resolution than scales with only 7 or 10 points. In the latter case, patients often do not use values close to the end points, so the 7-point scale often becomes a 5- or 3-point scale, and the 10-point scale becomes an 8- or 6-point scale. With 100-point scales, patients typically use either 10- or 5-point intervals. When the questionnaire is administered several times, standard deviations can be obtained for each question, and statistically significant changes for each individual question can be studied. The use of the 100-point scale has been criticized because it may be unwieldy or too esoteric for some patients (Newman and Sandridge, 2004). In our experience this is not the case. With a 100-point scale, we suggest that the patient consider the scale like a dollar bill, and to consider their responses like pennies or nickels or dimes. We have administered this and similar 100-point questionnaires to thousands of patients and have never seen one who found it too unwieldy or esoteric.
Activities Treatment Protocol
Emotional Well-Being
Tinnitus patients, like most people, often are experiencing problems in many aspects of their lives. Therefore, we begin our counseling by learning from the patients what general concerns are important for them. Occasionally, it becomes evident that the problems are beyond our expertise, and appropriate referrals to a clinical psychologist or psychiatrist are made.
We approach this by:
• Listening to the patient
• Providing information about hearing, hearing loss, tinnitus, and attention
• Discussing ways to make tinnitus less important
• Changing lifestyle to manage better
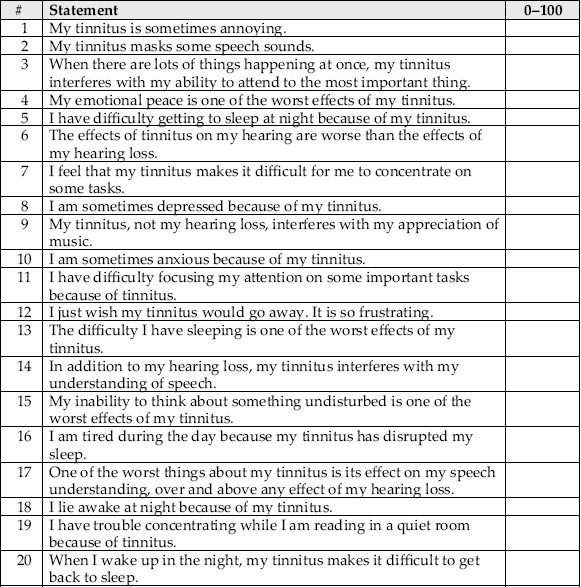
Figure 9–1 Iowa Tinnitus Activities Questionnaire.
LISTENING TO THE PATIENT
It is critical to determine what is important for the individual patient. Why is the patient here? What does he or she expect? Is the patient alone, or does he or she have support? Are other important things going on in the patient’s life in addition to tinnitus? Probing questions can help obtain such information. The answers to these questions can influence the direction of counseling. Having the patient describe how tinnitus has affected his or her life can be a useful way to begin. This facilitates a basic understanding of the whole patient and assists the clinician in determining when referrals to other professionals (i.e., psychologists, physicians) may be warranted. Fig. 9–2 is one of the illustrations we use to encourage patients to tell us about their specific problems. We say, “Please make a list of the difficulties that you think have been caused by your tinnitus. List them in order of importance.”
Figure 9–2 One of the initial illustrations used to ask patients about the role of tinnitus in their life.
PROVIDING INFORMATION ABOUT HEARING, HEARING LOSS, TINNITUS, AND ATTENTION
Providing basic information on tinnitus and related issues
• Helps patients realize they are not alone
• Removes some of the fear of the unknown
• Assists them in developing realistic expectations
In general, providing knowledge about hearing loss and tinnitus removes many unknowns, misconceptions, and fears. Fig. 9–3 conveys the concept of the coding of information in the nerves and in the brain. This neural activity is used to code the presence of acoustic sound. However, even without sound, there is random spontaneous activity in the nerves and in the brain. Later in the therapy session we discuss how tinnitus is likely coded in spontaneous activity (see Fig. 9–4).
A few common issues are addressed directly, including those posed by the following questions:
• Am I going to become deaf?
• Do I have a tumor?
• Will my tinnitus get worse?
We also follow the work of Hallam (1989), who emphasized the importance of hearing and attention. For example, he noted that we normally attend to only one thing at a time (see Fig. 9–5). Our attention can be diverted by things that are unusual or surprising. Hallam gave the example of a refrigerator hum being repetitive and meaningless so that our brain automatically tunes it out. Another example provided by Hallam is that we cannot decide not to pay attention to items—we subconsciously monitor the sensory environment for significant events (see Fig. 9–6). This is normal. If we decide tinnitus is important to monitor, then we will not be able to habituate to tinnitus. Hallam suggested that most people can learn to ignore tinnitus in ∼18 months.
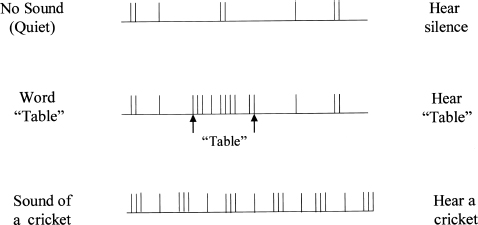
Figure 9–3 Diagram showing how neural impulses convey information to the brain. In the absence of any acoustic sound, there is random spontaneous activity on nerve fibers. When a word is spoken, such as table, a particular pattern of impulses is conveyed. Other sounds, such as the sound of a cricket, create a unique pattern of activity.
DISCUSSING WAYS TO MAKE TINNITUS LESS IMPORTANT
Our tinnitus treatment is designed to help patients change how they think about and react to their tinnitus. Providing information can help patients realize that their tinnitus need not be threatening. We have patients consider how they view their tinnitus. We also encourage patients to refocus their attention on other activities, such as joining new clubs and learning new tasks. It is important for patients to know that many people have tinnitus and are able to lead happy and productive lives. Group counseling (see Chapter 14) can be very effective with tinnitus patients.
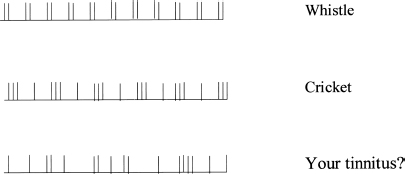
Figure 9–4 Examples of neural presentations of tinnitus that are perceived as the sounds of a whistle and a cricket. Patients are asked to describe what their tinnitus sounds like.
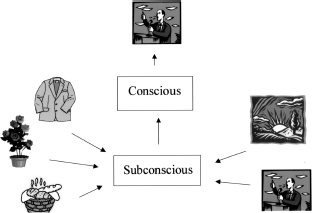
Figure 9–5 Diagram representing how many sensory stimuli are received subconsciously, yet we can usually attend to only one thing consciously.
EFFECTIVE LIFESTYLE CHANGES FOR BETTER TINNITUS MANAGEMENT
Addressing the many ways tinnitus can affect a patient (including sleep, hearing, and concentration) can lead to improvement in these areas and also help with the individual’s general emotional well-being. Part of this arises from the way the patient thinks about these issues. Cognitive therapy separates the tinnitus from the patient’s reaction to it (see Fig. 9–7).
Patients often benefit from being given a specific assignment to work on to assist them in changing how they cope with their tinnitus. We sometimes use a “tinnitus diary” for the first few weeks of treatment. Patients are asked to list situations where their tinnitus is worse and situations where their tinnitus is better (Stouffer and Tyler, 1990). It is then possible to discuss these situations and determine if the patient’s environment can be modified to increase the good situations and decrease the bad ones. We recommend that such a diary be used for only a few weeks because we want the patient to move away from thinking about tinnitus.
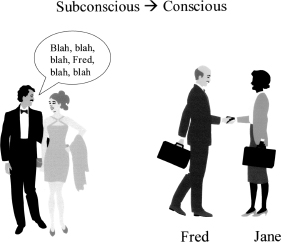
Figure 9–6 Illustration depicting how an important subconscious stimulus can grab our attention. Although Fred and Jane are talking between themselves, Fred’s conscious attention is interrupted when his name is mentioned in a background conversation.
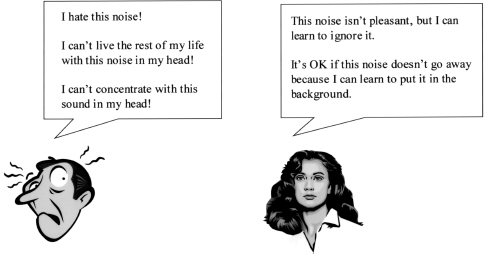
Figure 9–7 Illustration showing different ways of thinking about the same tinnitus. One person “hates” the tinnitus. The other person doesn’t like it, but is prepared to learn different ways of reacting to it.
The use of background sound and partial masking is helpful to many patients. Even if we do not recommend a wearable device for partial or total masking, providing a rationale for and activities related to background sound is usually helpful. Fig. 9–8 shows how partial masking can reduce the neural prominence of the tinnitus. Fig. 9–9 shows how we draw analogies between the visual and auditory domain; partial masking can be effective in either. Fig. 9–10 is one of several examples of activities the patient can use to decrease the prominence of the tinnitus. Having this knowledge and skill is helpful for all four areas: emotional well-being, sleep, hearing, and concentration.
Sleep
Sleep disturbances are very common in tinnitus patients (e.g., McKenna, 2000; Tyler and Baker, 1983; see also Chapter 7). Some patients report difficulty falling asleep, waking during the night, early awakening, or being tired during the day. Being under emotional stress and having difficulty concentrating and hearing can also contribute to fatigue. Our therapy regarding sleep includes:
• Understanding normal sleep patterns
• Exploring factors that can affect sleep (stress, environmental noise, room temperature)
• Arranging the bedroom to promote sleep (i.e., comfortable bedding, removing non-sleep-related items from the bedroom)
• Avoiding drinking alcohol, smoking, and eating before bedtime
• Using background sound to reduce the prominence of tinnitus (i.e., quiet music, nature sounds)
• Learning relaxation exercises (i.e., progressive muscle relaxation and visual imagery)
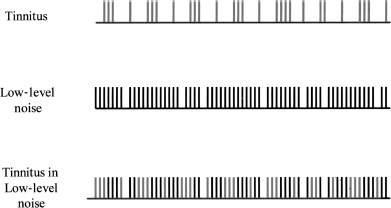
Figure 9–8 Diagram representing how the neural activity of the tinnitus can be partially masked by presenting low-level background sound.
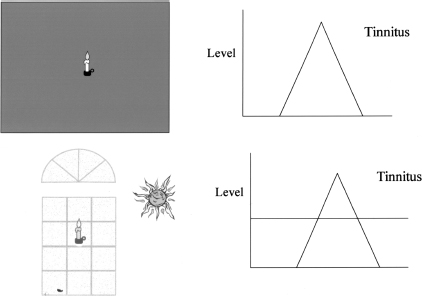
Figure 9–9 Illustration depicting the analogy between partial masking of light and sound. On the left, a candle in a dark room is partially masked by the bright sunlight through a window. On the right, the tinnitus is partially masked by a background noise.
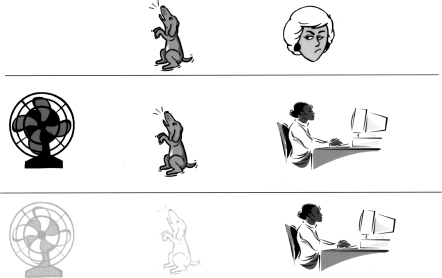
Figure 9–10 An example of how background noise can partially mask an annoying barking dog while someone is trying to concentrate on work.
Fig. 9–11 lists steps to be taken to arrange a bedroom and encourage good sleep patterns.
Hearing
The goal of this therapy is to help patients understand how tinnitus can affect hearing and provide some approaches for patients to use to improve their hearing. Improving hearing should
• Alleviate some of the communication difficulties associated with hearing loss
• Improve communication difficulties associated with tinnitus
• Reduce stress
Fig. 9–12 introduces some of the general areas to be covered regarding hearing. Many of these areas can actually be demonstrated, not simply discussed.
HEARING AND HEARING LOSS
One way to reduce difficulties associated with hearing loss is to help the patient better understand hearing and hearing loss. First, we briefly explain to our patients how the auditory system works by reviewing some basic anatomy and physiology. Second, we talk to them about how the auditory system is affected when we acquire a hearing loss. Finally, we discuss with our patients various difficulties that they may experience as a result of their hearing impairment. Particularly, we help them understand the perceptual consequences of hearing loss and that some sounds that they once heard may be difficult to distinguish or may no longer be audible to them at all. For example, if they have a high-frequency hearing loss, we would explain to them why they perceive people talking to them as “mumbling” or why sounds with mostly high-frequency energy, like/s/, will often no longer be heard. We also explain to them how noise can affect their hearing and the importance of the signal-to-noise ratio.
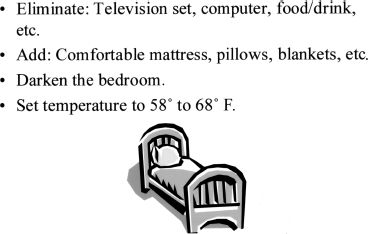
Figure 9–11 Activities for arranging the bedroom to facilitate sleep.
HEARING DIFFICULTIES DUE TO HEARING LOSS AND TINNITUS
It is important to help patients understand and distinguish difficulties they may be experiencing due to their hearing loss versus those they may be experiencing as a result of their tinnitus. We explain to patients that hearing loss will make some sounds they hear seem distorted and other sounds almost completely inaudible. We also explain that tinnitus does not cause a hearing loss, but it can produce hearing difficulty by distracting one from listening. The ringing, buzzing, or roaring sound of the tinnitus can also produce a masking of some sounds (Surr et al, 1985). In addition, we explain that tinnitus can cause difficulties in distinguishing one sound from another because the tinnitus sound can be confused with other sounds that have the same pitch. For example, sometimes people with tinnitus may hear a sound, like a whistle, then discover that it was actually their tinnitus.
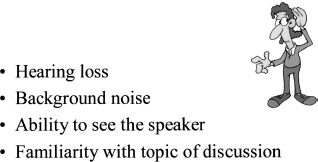
Figure 9–12 Different factors that can affect communication.
STRATEGIES TO IMPROVE HEARING AND REDUCE STRESS
There are three main areas that we discuss in detail to help patients better manage their hearing loss. These consist of the following.
Amplification The first step in managing a hearing loss is to make sure that patients are fit with an appropriate hearing device (see Chapters 12 and 13). This may consist of fitting the patient with a hearing aid or an assistive listening device. First, we explain to the patient how a hearing aid and an assistive listening device function. Next, we discuss the importance of using a device that is appropriate for the patient’s hearing loss and personal life. We also discuss the advantages of binaural hearing aids (Balfour and Hawkins, 1992). Finally, if the patient is already wearing a hearing device, we check the appropriateness of the fit and briefly answer any questions that the patient may have about the current device.
Environment Patients are often unaware of how the environment influences their hearing performance. We teach patients that environments with the following characteristics are more suitable for facilitating a conversation (Dillon, 2001):
• Good lighting
◯ Making sure that there is adequate light to illuminate the communication partner’s face without shadowing it
◯ Moving away from light that is shining directly in the listener’s eyes and making it difficult to see the communication partner’s face
• Positioning
◯ Being close to the communication partner, thereby creating a better signal-to-noise ratio
◯ Making sure that the face of the communication partner is visible and not in profile
• Minimizing visual distractions
◯ Closing a door to eliminate movement from another room
◯ Closing a window to eliminate blowing curtains or other distractions
◯ Turning off a television
• Minimizing noise
◯ Turning off extraneous sources of noise (TV, radio, kitchen appliances, etc.)
◯ Closing doors and windows to minimize background noise
Communication One of the most important things we do with our patients is to empower them to take charge of their hearing loss by using an effective communication style. First, we define assertive communication and compare that with passive and aggressive styles (Tye-Murray, 1998). We then teach them, regardless of their personality type, how to become an assertive rather than a passive or aggressive communicator. Finally, we demonstrate appropriate assertive communication while teaching the following:
• Use of repair strategies to repair communication breakdowns (i.e., asking individuals to slow down, use clear speech, repeat, rephrase, reduce, or elaborate sentences).
• Use of anticipatory strategies prior to communication interactions (i.e., knowing the topic and/or key vocabulary words, using relaxation tech niques, and/or practicing dialogue)
• How to disclose hearing loss to potential conversation partners, when appropriate
• Speech-reading strategies (i.e., watching facial expressions and body movements)
Concentration
We address three areas to improve concentration: providing information, decreasing the prominence of the tinnitus, and increasing attention to the task at hand.
PROVIDE INFORMATION ABOUT CONCENTRATION DIFFICULTIES
Everyone can be distracted by visual and auditory stimuli. Fig. 9–13 reviews factors that contribute to our ability to concentrate and sets the stage for related activities. Distracting stimuli can be
• Annoying
• Fearful
• Competing with the desired target
• Loud
• Unpredictable
• Uncontrollable
Figure 9–13 Things that can affect concentration, including factors in (A) the environment and (B) your physical and emotional state.
We begin by discussing differences in concentration skills. Some people cannot read in a noisy coffee shop, whereas others can do so easily. Yet people can learn to focus their attention. An example of this is that some individuals with chronic pain can successfully train themselves to focus their attention away from their discomfort and onto other activities.
Not everyone is distracted by his or her tinnitus. We discuss reasons for these individual differences. We also ask patients if there are situations where they are not distracted by their tinnitus. We try to figure out what it is about these situations, and whether or not their characteristics can be transposed to other situations.
We discuss the fears patients may have about tinnitus and, with appropriate information, help them to realize that they do not need to be so threatened by the disorder.
DECREASING THE INTRUSIVENESS OF THE DISTRACTION
Various kinds of sound therapy can decrease the prominence of tinnitus and reduce its distracting nature. We often recommend partial masking, with either wearable or nonwearable devices, and have recently used background music in a more systematic fashion (see Figs. 9–9 and 9–10).
We compare the intrusiveness of intense visual stimuli in a dark room to the intrusiveness of tinnitus in a quiet room. Adding more background light can be helpful in the first situation, in the same way that adding low levels of background sound can be helpful in dealing with the tinnitus. The effects of light and real (non-tinnitus) sounds can be demonstrated in activities during the counseling session. For example, many patients prefer the masking sound of water when they are required to listen to an intense whistle.
FOCUSING ATTENTION ON THE TASK
Henry and Wilson (2001, p. 79) describe an “attention diversion” approach to help tinnitus patients. Patients practice refocusing their attention from one stimulus to another (Fig. 9–14). In this therapy, we have found that it can be easier to begin with physical sensations, such as clothing on the skin. Practice can then be done with being aware of external sounds and, later, directing attention to and from tinnitus. Patients are taught that there are some aspects of their attention they can control, and that they can divert attention away from their tinnitus and onto other tasks.
Another strategy is for patients to modify how they approach tasks in which they are having difficulty concentrating (Fig. 9–15). For example, a complex task requiring focused and prolonged concentration can be reduced to smaller tasks requiring less intense concentration, or tasks that require intense concentration can be done for shorter periods of time. Reading is one task that can easily be segmented into shorter intervals.
Developing self-confidence can help a patient concentrate. Learning a new task can increase motivation. Patients can be encouraged to learn a new game or try a new computer program, for example. When patients are able to experience success with their concentration abilities, they may feel greater control over their concentration skills and be more confident when undertaking future tasks.
Figure 9–14 Illustration introducing attention control exercises.
Duration of Therapy Sessions
For many patients, it may be that a 5- to 15-minute counseling session that provides a brief overview of the general principles outlined in this chapter will be sufficient (see Preece et al, 2003; Tyler and Erlandsson, 2000). During the initial consultation with a patient we determine if a more thorough counseling session is warranted.
Our complete counseling package is usually provided over the course of several sessions. We have found that presenting the material in this manner gives patients the opportunity to practice the strategies covered in each session for a period of time before returning to discuss their experiences with the clinician. Presenting the material over several sessions also allows for repetition of key concepts and makes it easier to avoid overloading patients with too much information in any one session. Most patients can complete the counseling in three or four sessions, typically lasting 1 hour each and separated by 1 or 2 weeks.
Figure 9–15 Examples of how people stay focused when their concentration is challenged.
Conclusion
This chapter outlines our general approach to tinnitus activities therapy and partial masking therapy. The activities therapy covers emotional-well being, hearing, sleep, and concentration. The treatment has evolved from our informational counseling approach of the 1980s and has greatly benefited from the work of Hallam (1989) and Henry and Wilson (2001). We are now testing the treatment in controlled studies to determine its effectiveness.
Acknowledgments
We wish to acknowledge grant support provided by the American Tinnitus Association and the National Institutes of Health (NIH Grant 5R01DC005972–02). Richard Tyler is an Obermann Scholar at the Obermann Center for Advanced Studies at the University of Iowa. In addition to those mentioned in the article, Anne-Mette Mohr, Cynthia Bergan, and Diana Kain made valuable contributions to the development of our ideas.
References
Balfour P, Hawkins D. A comparison of sound quality judgments for monaural and binaural hearing aid processed stimuli. Ear Hear 1992;13(5):331–339
Bentler RA, Tyler RS. Tinnitus management. ASHA 1987(May):27–32
Coles RRA. Tinnitus and its management. In: Stephens SDG, Kerr AG, eds. Scott-Brown’s Otolaryngology. Guildford, UK: Butterworth; 1987;(2):368–414
Coles RRA, Hallam RS. Tinnitus and its management. Br Med Bull 1987;43:983–998
Dillon H. Hearing Aids. Turramurra, Australia: Boomerang Press; 2001
Flasher LV, Fogle T. Counseling Skills for Speech-Language Pathologists and Audiologists. Clifton Park, NY: Thomson Delmar Learning; 2004
Hallam RS. Tinnitus: Living with the Ringing in Your Ears. New York: HarperCollins; 1989
Hallam R, Rachman S, Hinchcliffe R. Psychological aspects of tinnitus. In: Rachman S, ed. Contributions to Medical Psychology. Vol 3. Oxford: Pergamon Press; 1984:31–53
Henry JL, Wilson PH. The Psychological Management of Chronic Tinnitus: A Cognitive-Behavioral Approach. Boston: Allyn & Bacon; 2001
Henry JL, Wilson PH. Tinnitus: A Self-Management Guide for the Ringing in Your Ears. Boston: Allyn & Bacon; 2002
McKenna L. Tinnitus and insomnia. In: Tyler RS, ed. Tinnitus Handbook. San Diego: Singular; 2000:59–84
Newman CW, Sandridge SA. Tinnitus questionnaires. In: Snow JB, ed. Tinnitus: Theory and Management. Hamilton, Ontario, Canada: BC Decker; 2004:237–254
Preece JP, Tyler RS, Noble W. The management of tinnitus. Geriatrics Aging 2003;6(6):22–28
Stouffer JL, Tyler RS. Characterization of tinnitus by tinnitus patients. J Speech Hear Disord 1990;55:439–453
Stouffer JL, Tyler RS, Kileny P, Dalzell L. Tinnitus as a function of duration and etiology: counseling implications. Am J Otol 1991;12(3):188–194
Surr R, Montgomery A, Mueller H. Effect of amplification on tinnitus among new hearing aid users. Ear Hear 1985;6(2):71–75
Sweetow RW. Cognitive-behavioral modification in tinnitus management. Hearing Instruments 1984;35:14–52
Tye-Murray N. Foundations of Aural Rehabilitation: Children, Adults, and Their Family Members. San Diego: Singular; 1998
Tyler RS, Babin RW. Tinnitus. In: Cummings CW, Fredrickson J-M, Harker L, Krause CJ, Schuller DE, eds. Otolaryngology–Head and Neck Surgery. St. Louis: Mosby; 1986:3201–3217
Tyler RS, Baker LJ. Difficulties experienced by tinnitus sufferers. J Speech Hear Disord 1983;48:150–154
Tyler RS, Baker LJ, Armstrong-Bednall G. Difficulties experienced by hearing-aid candidates and hearing-aid users. Br J Audiol 1983;17:191–201
Tyler RS, Bentler RA. Tinnitus maskers and hearing aids for tinnitus. Semin Hear 1987;8(1):49–61
Tyler RS, Bergan C. Tinnitus retraining therapy: a modified approach. Hearing J 2001;54(11):36–42
Tyler RS, Erlandsson S. Management of the tinnitus patient. In: Luxon LM, Furman JM, Martini A, Stephens D, eds. Textbook of Audiological Medicine. Oxford: Isis Publications; 2000:571–578
Tyler RS, Haskell G, Preece J, Bergan C. Nurturing patient expectations to enhance the treatment of tinnitus. Semin Hear 2001;22:15–21
Tyler RS, Stouffer JL, Schum R. Audiological rehabilitation of the tinnitus client. J Acad Rehab Audiol 1989;22:30–42
Wilson PH, Henry JL, Andersson G, Hallam RS, Lindberg P. A critical analysis of directive counseling as a component of tinnitus retraining therapy. Br J Audiol 1998;32:273–286
< div class='tao-gold-member'>



