12
Hearing Aids and Tinnitus
Hearing aids have long been considered useful tools in tinnitus management (Saltzman and Ersner, 1947). They have been used for total and partial masking therapies (Coles, 1985; Hazell et al, 1985; Vernon and Meikle, 2000; Von Wedel et al, 1998; see also Chapters 1 and 13 in this book), including tinnitus retraining (Jastreboff and Hazell, 1993; Jastreboff and Jastreboff, 2000; see also Chapter 10), and as adjuncts to the psychological management of tinnitus (Hallam et al, 1984). In a survey of tinnitus patients over one third of respondents reported that the primary benefit of attending a specialized tinnitus clinic was the fitting of hearing aids (Sanchez and Stephens, 2000). This chapter will briefly consider the existing literature on the use of hearing aids for tinnitus management before focusing on the practical aspects of fitting these instruments for treating tinnitus.
How Hearing Aids Help Reduce Tinnitus
There are at least five ways the fitting of hearing aids can benefit tinnitus sufferers (Coles, 1985):
1. Assisted hearing has psychological benefits.
2. Less attention is paid to hearing, and consequently tinnitus.
3. Patient comes to understanding that hearing loss is the main cause of communication problems, not tinnitus.
4. Ambient noise and internal circuit noise can make the tinnitus less audible.
5. The counseling accompanying hearing aid fitting can provide an under standing of tinnitus.
In addition, the sounds amplified by hearing aids produce neural activity throughout the auditory system, which interfere or compete with the central auditory representation of tinnitus (whatever form it may take; see Chapter 1), and divert attention to complex sounds of greater importance or interest, such as speech and music (Andersson, 2002).
Few studies have been published on the success rate of hearing aid fitting in managing tinnitus. Surr et al (1985) reported that ∼50% of hearing aid patients achieved some relief from tinnitus, and Surr et al (1999) found an average 10 % improvement in tinnitus handicap 6 weeks following the fitting of hearing aids. In contrast, Melin et al (1987) concluded that hearing aids alone were not effective devices for reducing tinnitus. The, at best, modest success of hearing aids in those studies must be placed in context; predominantly linear hearing aids were fitted in a conventional manner solely to improve hearing. Through careful selection of hearing aid characteristics and by fitting the hearing aids with the intention of reducing tinnitus audibility, the likelihood of a reduction in tinnitus may be increased.
Protocol for Using Hearing Aids to Help Reduce Tinnitus
The tinnitus management protocol suggested here places an emphasis on the comfortable amplification of speech to divert attention paid to tinnitus, as well as amplification of ambient sound to reduce tinnitus audibility. The initial goal is partial masking using amplified ambient sound and speech. The long-term goals are to reduce the amount of attention paid to tinnitus and to consequently reduce tinnitus awareness.
The protocol involves five or six 1-hour appointments. An additional appointment at 6 months assesses progress and addresses patient concerns. The protocol comprises the following elements:
1. Diagnostic audiology and tinnitus evaluation
2. Counseling
3. Instrument selection for sound therapy
4. Instrument fitting
5. Follow-up
Some elements within the protocol, such as the assessment of tinnitus and counseling, will be discussed only briefly here because they have been covered in detail elsewhere in this book, are common to most tinnitus therapies, and are not the focus of this chapter.
Diagnostic Audiology and Tinnitus Evaluation
The first step in the evaluation of tinnitus and then its management is a comprehensive case history, including questions of onset, description, location, possible cause (noise, medications, stress), and severity. If the tinnitus is objective, pulsatile, unilateral, or associated with a temporomandibular joint complaint, referral to an otolaryngologist is made. If the patient is experiencing anxiety or depression, referral to a psychologist is organized.
The assessments of hearing and tinnitus undertaken are consistent with standard audiological practice and are similar to those used at other tinnitus clinics (Jastreboff and Jastreboff, 2000; Sandlin and Olsson, 1999). In addition, self-report questionnaires—for example, Tinnitus Severity Index (Meikle et al, 1995) and the Tinnitus Handicap Questionnaire (Kuk et al, 1990)—assist in identifying the most bothersome aspects of the individual’s tinnitus that need to be addressed by counseling and possibly sound therapy. These results are used to identify specific areas of tinnitus impact to be discussed at counseling sessions.
Counseling
Counseling should be considered a tinnitus management strategy in its own right as well as an adjunct to other management strategies, including hearing aid fitting. To be successful in counseling the tinnitus sufferer, the clinician should have extensive knowledge of the physiology of the hearing system, tinnitus mechanisms, and management. First and foremost the counseling should provide reassurance and correction of false beliefs (e.g., Hazell, 1999). The counseling session typically involves family members or friends, as well as the patient, and comprises the elements recommended by Wilson et al (1998) and others (see Chapter 1). A client-centered approach is used with greater discussion of those areas important to the tinnitus sufferer (see Chapter 15). The clinician must assess the level of understanding of the patient and adjust the counseling appropriately. A counseling session is wasted if the patient does not understand the information provided. The session is facilitated by a slide show presentation of
• Cochlear anatomy and pathology
• Hearing loss
• Auditory pathways and central auditory processing of sound
• Tinnitus mechanisms
• Conditioned responses
• Tinnitus management options
• Stress and anxiety
• Attention distraction strategies
Written information is given to the patient detailing key points and referral sources for stress management. Pen-and-paper exercises explaining tinnitus and its management are completed by the patient and his or her audiologist. The mechanism of tinnitus generation, which is explained to the patient, is related back to the individual’s audiological and tinnitus evaluation. Typically, patients are told that
• Most tinnitus appears to be the consequence of the auditory system’s interpretation of altered activity from the inner ear.
• Unevenness in the spontaneous (background) output of the cochlea may be exaggerated by central auditory processing, which can eventually lead to a change in the functional organization of the auditory cortex.
• Tinnitus severity is not fully explained by the degree of ear damage because there is poor correlation between hearing threshold and tinnitus distress.
• It is thought that much of the severity of tinnitus relates to enhancement by central auditory processing and the individual’s reaction to the abnormal perception.
Patients are counseled as to the various tinnitus therapies available at the clinic and other clinics. The premise of using hearing aids, sound generators (maskers), and combination devices for reducing tinnitus audibility are discussed. Patients are told that
• Hearing aids should improve communication and divert attention from the tinnitus.
• Hearing aids also amplify background sound, which should decrease the prominence of the tinnitus.
• Patients should enrich their listening environment with music or other sounds to divert attention away from the tinnitus and to partially mask it. A selection of sounds (white, pink, and brown noise and nature sounds) is available on a digital music playback system from the clinic for this purpose.
• Sound therapy using hearing aids and an enriched listening environment may interfere with the central processing of the tinnitus, leading to reduced awareness of the tinnitus.
To focus counseling and determine goals and realistic expectations for management, a version of the Client Orientated Scale of Improvement (COSI; Dillion et al, 1999) is used. The original COSI assesses patients’ communication needs and outcomes achieved following the fitting of hearing aids. Using the Client Orientated Scale of Improvement in Tinnitus (COSIT), the clinician and patient identify specific situations in which tinnitus is bothersome (e.g., “Tinnitus affects my ability to concentrate at work”) and means of reducing tinnitus in these situations (e.g., amplify sound to reduce tinnitus audibility). At stages throughout the tinnitus rehabilitation process the problems identified using the COSIT are reexa-mined, and improvement in tinnitus in each situation is determined. If improvement is not shown, appropriate steps are undertaken to address the problem until realistic goals are achieved.
Instrument Selection for Sound Therapy
Our approach for determining hearing aid candidacy is similar to that of Vernon and Meikle (2000, p. 328): “If the patient has hearing impairment, always try hearing aids first regardless of the nature and extent of the hearing loss.”
Unless the patient has normal pure-tone audiometry or hearing loss confined to greater than 6 kHz, hearing aids are the instruments initially trialed. Hearing aids are not fitted to those individuals with hearing loss confined to above 6 kHz due to the limited high-frequency amplification provided by most hearing aids. When the individual has normal hearing (5% of patients at our clinic), ear-level sound generators are provided and fitted in a manner similar to that recommended by some of the partial masking therapies (see, e.g., Chapters 1, 10, and 13), or are considered for the acoustic desensitization protocol discussed in Chapter 11.
When selecting hearing aids, the aim is to find devices that will achieve the dual, but potentially antagonistic, goals of improving the audibility of speech and amplifying ambient sound to interfere with tinnitus. To meet both goals, we often use multiple program hearing aids, with one program dedicated to tinnitus management. This tinnitus program incorporates features desirable for tinnitus management; namely, those that enhance perception of quiet environment sounds without sacrificing listening comfort.
DESIRABLE HEARING AID FEATURES FOR TINNITUS MANAGEMENT
The pros and cons of different hearing aid features are discussed following here, with a view to assist in the selection of hearing aids for managing tinnitus. Not all features of modern aids are beneficial in tinnitus management.
Open Fitting Open fittings reduce occlusion and increase user comfort, which is important if the patient is to become accustomed to the aids. Reduction in environmental sound, from blocking the ear canal, can result in increased tinnitus awareness (Sheldrake et al, 1996). Although behind-the-ear aids and open ear molds are often recommended, the fitting of in-the-canal and completely-in-the canal hearing aids is often successful when open venting is used. Although large vents in in-the-ear aids can increase the risk of acoustic feedback, the feedback management algorithms available in many of today’s aids enable greater venting than was previously possible. With some aids, however, the feedback management occurs at the expense of a reduction in gain, possibly increasing the audibility of the tinnitus. There are also occasions in which less venting is appropriate, such as low-frequency hearing losses (Tyler and Bentler, 1987). The conflicting merits of open fittings and desired amplification levels need to be considered with every fitting. Measurement of the real-ear occluded response (Hawkins and Mueller, 1992) allows a means of checking if attenuation of external sounds is too great. If ambient sound is at all attenuated, attempts should be made to increase venting or adjust aid settings to provide extra amplification of soft sounds.
Compression and Expansion Low-compression kneepoints enable the amplification of low-intensity environmental sounds to audible levels without causing discomfort to louder sounds. Understanding the degree to which a particular hearing aid, or aid setting, results in the amplification of low-intensity sounds is fundamental to knowing how to adjust hearing aids to reduce tinnitus audibility. Fig. 12–1 illustrates a loudness growth function for a normal-hearing person and a hearing-impaired person, superimposed with an ambient noise level of 30 dB SPL (Fig. 12–1A) and input/output curves for a hearing aid with similar compression characteristics, except varying kneepoint from 30 (Fig. 12–1B) to 50 dB SPL (Fig. 12–1C). If the amount of gain to moderate inputs is maintained and the kneepoint is lowered, the level of ambient noise perceived should increase. Wide dynamic range compression with low-compression kneepoints (20–45 dB SPL) is recommended. Circuit noise, long thought of as an ally in tinnitus management (Tyler and Bentler, 1987), is often inaudible in digital hearing aids due to expansion or “soft squelch.” Expansion results in a more rapid reduction in gain below the kneepoint than in conventional compression (Fig. 12–1D). The goal of expansion is exactly the opposite of what is desirable for reducing tinnitus audibility in quiet: the reduction of ambient sound and circuit noise. The effect of reducing the compression kneepoint on the amplification of ambient room noise is shown in Fig. 12–2.
Multiple Microphones and Noise Reduction Algorithms Switchable microphones (directional/omnidirectional modes) enable optimization of options for a patient wishing to hear speech in background noise (May, 1998; Ricketts and Mueller, 1999) and allow change to omnidirectional hearing to take maximum advantage of diffuse ambient noise for tinnitus management. Noise reduction digital signal–processing algorithms monitor temporal and spectral characteristics of sound and attempt to reduce amplification in channels in which speechlike stimuli are not present (Schweitzer, 1997). Digital noise reduction in hearing aids has yet to be proven effective in improving speech recognition in noise, but it may improve listening comfort through reduced amplification in noise (Bray and Nilsson, 2002; Trine and Van Tasell, 2002). However, these algorithms also effectively reduce the ambient sounds used to partially mask tinnitus (Fig. 12–3). Our preference is for hearing aids in which noise reduction features can be turned off and omnidirectional characteristics selected when in quiet environments.
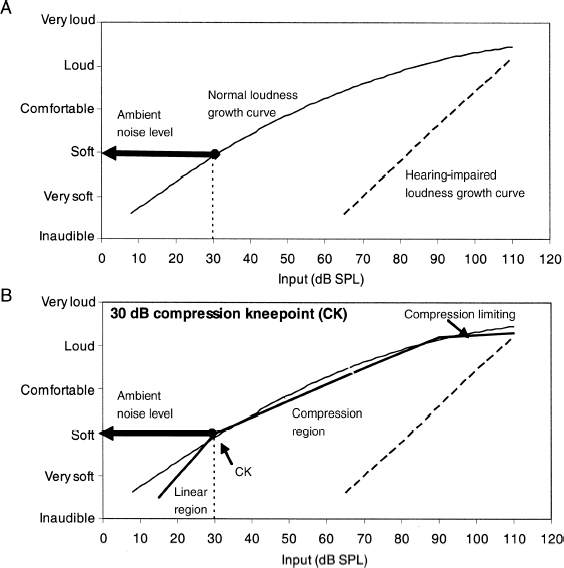
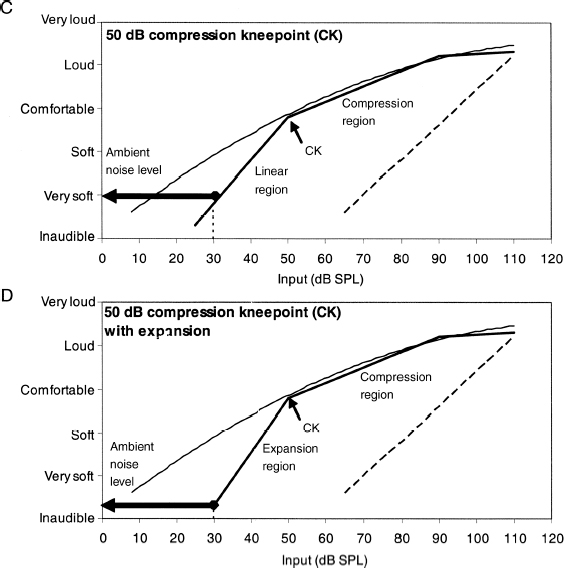
Figure 12–1 The rationale behind choosing a low-compression kneepoint for amplification of ambient sound. Input/output curves for different hearing aid compression kneepoints are shown compared to a loudness growth function for a normal-hearing listener (solid line) and a hearing-impaired listener (dashed line) (loudness growth curves modified from Pluvinage, 1994). An ambient noise level of 30 dB SPL is shown (vertical dotted line). (A) For the normal-hearing listener, the ambient sound is soft (arrow), whereas for the impaired listener, the sound is inaudible. (B) Input/output curve from a hearing aid with a compression kneepoint of 30 dB SPL. The hearing aid has been fitted to return the impaired listener’s perception of moderately intense sounds to normal levels; ambient sounds are heard as soft (arrow). (C) With the compression kneepoint set at 50 dB SPL, the ambient sound of 30 dB SPL is very soft. (D) The same as C but with expansion below the compression kneepoint. Expansion below the kneepoint means background sounds are barely audible. By having a low-compression kneepoint, without expansion, greater amplification is provided to low-intensity sounds, making them audible to the hearing-impaired listener. This allows low-intensity environmental sounds to interfere with the detection of tinnitus, without overamplifying louder sounds. CK, compression kneepoint.
Automatic Volume Controls Automatic volume controls are advantageous for tinnitus management. When appropriately set, automatic volume adjustment may result in less attention being paid to the aids, ears, and, consequently, tinnitus. Constant volume control manipulation may focus attention to the ears, which will hamper attempts to ignore tinnitus. Volume controls can be useful to increase amplification in quiet environments, but they are unnecessary if the hearing aid user is able to select different amplification settings for normal and quiet environments through use of a program selector switch or remote control.
Multiple Programs: The “Tinnitus Program” Several hearing aid manufacturers promote the use of hearing aids with user-selectable listening programs designed for different listening situations (e.g., background noise or music). These programs attempt to optimize combinations of gain, compression, frequency response, and digital signal processing to suit the listener’s environment. To interfere with tinnitus perception without sacrificing communication, it is often prudent to choose a hearing aid with at least two listening programs. One program can be optimized for communication, and one can be optimized to amplify background sounds. The “tinnitus program” is intended for quiet environments where conventionally amplified ambient sounds would be inaudible or too faint to interfere with the tinnitus. The tinnitus program should have many of the features already described as being beneficial for tinnitus management, such as
• A low-compression kneepoint (at or below 40 dB SPL)
• Soft squelch or expansion turned off
• An omnidirectional microphone setting
• Noise reduction algorithms switched off
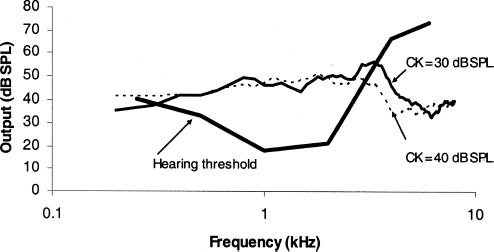
Figure 12–2 Probe microphone measurements illustrating the effect of a change in compression kneepoint on aided ambient sound levels (compression kneepoint 30 dB SPL: solid line, compression kneepoint 40 dB SPL: dashed line). The ambient sound being amplified was on average 30 dB SPL. The lower compression kneepoint resulted in greater amplification of background sound in the region of the hearing loss. CK, compression kneepoint.
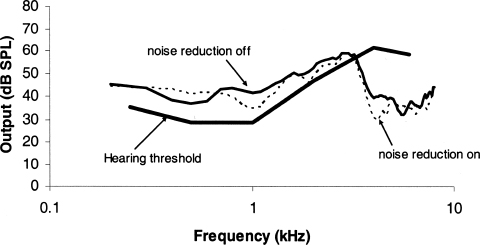
Figure 12–3 Probe microphone measurements illustrating the effect of switching off noise reduction digital signal processing on the amplification of ambient sound (noise reduction off: solid line, noise reduction on: dashed line). Ambient background sounds were more audible with the noise reduction feature disabled.
The principle is to provide as much gain of low-intensity ambient sound as possible without louder sounds causing discomfort. Our rule of thumb in choosing settings for the tinnitus program is to turn off or minimize settings that are promoted as noise reduction features.
Monaural versus Binaural Binaural fittings are advocated in the presence of a hearing loss in both ears. This is done to achieve fairly symmetrical stimulation of the auditory system, to divert attention away from potentially unilateral tinnitus, and to achieve the documented benefits for speech recognition (Ross, 1980). For a unilateral hearing loss, consideration could be given to binaural stimulation with a noise generator for the normal-hearing ear (e.g., hearing aid for right ear, sound generator for left ear). In practice the necessity for such an approach is rare. However, if the hearing aid alone does not interfere with tinnitus detection, a noise generator for the normal-hearing ear can be trialed. Evidence for the long-term merit of binaural versus monaural sound therapy in unilateral tinnitus has yet to be established.
Summary: Hearing Aid Features for Tinnitus Management The hearing aids chosen for tinnitus management should meet the communication needs of the individual. Because of the complex interaction between sound and tinnitus (Feldmann, 1971; Hallam et al, 1984), as well as the loudness sensitivity that often accompanies tinnitus, hearing aids that allow the clinician to alter compression characteristics (compression kneepoint, ratio, maximum power output) and noise reduction features (expansion, noise reduction algorithms, microphone settings) and provide very different settings depending on the listening environment (multiple programs) are recommended.
Instrument Fitting
PHYSICAL COMFORT
The physical comfort of the device is evaluated by placing the aid switched off in the ear. Any physical discomfort due to the aid will heighten the patient’s awareness of the ear, focusing attention on the tinnitus. Alterations to the hearing aid shell or mold to ensure that the aid is comfortable, if not a change in style (e.g., completely-in-the-canal to behind-the-ear), are recommended.
OCCLUSION MEASURES
The extent to which the chosen hearing aid prevents transmission of sound by occluding the ear canal is determined using real-ear measurements (Hawkins and Mueller, 1992). A comparison between the real-ear unaided and occluded (aid in but switched off) responses indicates the extent to which the device attenuates sound. If the hearing aid significantly blocks quiet sounds, steps can be taken to overcome this by increasing the vent size or changing the ear mold style. Some occlusion of the ear with the aid switched off is acceptable only if the aid switched on can amplify sounds to overcome any insertion loss of ambient sound.
PRESCRIPTION OF HEARING AID AMPLIFICATION
Prescriptive procedures for hearing aid amplification, such as NAL-NL1 (Dillion, 1999) and DSL[i/o] (Cornelisse et al, 1995), have been developed to determine the most appropriate amount of amplification for an individual based on his or her hearing loss. The amount of amplification that best assists hearing speech and that which is optimized to reduce tinnitus audibility in quiet environments is different (Wise, 2003). Also, the amount of amplification normally prescribed by these formulas for high-intensity sounds may exceed the usually low loudness tolerance of tinnitus sufferers.
Hearing Program The hearing aid is adjusted to match real-ear insertion response targets at multiple test levels according to the NAL-NL1 prescriptive procedure. Real-ear probe microphone measurements are undertaken on all aids to verify a good match to prescribed gain. When patients have a history of sound intolerance, it is recommended that uncomfortable loudness levels be measured (Hawkins et al, 1992) rather than being predicted from the audiogram. The hearing aid’s output to high-intensity sound is measured (80–90 dB SPL, swept tones) using the probe microphone system, and the maximum output of the aid is altered where necessary to be below uncomfortable loudness levels.
Tinnitus Program In a second program the aid settings are optimized to amplify ambient sound to partially mask tinnitus. The DSL[i/o] prescriptive target is used as a starting point for the tinnitus program because preliminary evidence indicates that tinnitus is less audible with hearing aids set to this prescription than NAL-NL1 (Wise, 2003). The most likely reason for reduced tinnitus audibility using the DSL[i/o] prescription is that it prescribes greater low-intensity, low-frequency amplification than NAL-NL1 (Dillon, 2001), and most noise is concentrated in the low frequencies (Moreland, 1988).
When undertaking the real-ear measures, the response to a moderate-intensity (65 dB SPL) stimulus (swept tone or composite noise) is matched to the DSL[i/o] aided target, then a quiet background sound (of ∼30 dB SPL) is amplified to meet or exceed auditory threshold across as wide a frequency range as possible (Fig. 12–4). The level of sound used is lower than that produced by real-ear measurement equipment; this requires the real-ear equipment signal to be switched off and replaced by a signal external to the equipment. The ambient sound within the clinic room or just audible sound from a hearing aid manufacturers’ environmental sound compact disc can be used as the stimulus to be measured. The amount of amplification finally chosen is usually that which results in the tinnitus being less easily detected without discomfort to the listener. For some patients total masking can be achieved with little amplification of sound. If the degree of ambient sound amplification is unpleasant for the patient, the amount of gain is reduced. Just as with the hearing program, output to high-intensity sound is measured and adjusted so as to be lower than measured uncomfortable listening levels.
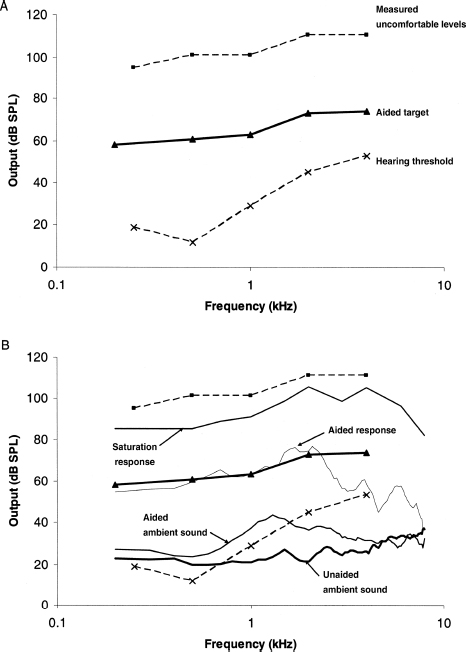
Figure 12–4 Prescription of amplification for tinnitus. (A) DSL[i/o] real-ear aided target (solid line) for an adult with a mild high-frequency sensorineural hearing loss (dB SPL, lower dashed line) and measured uncomfortable loudness levels (dB SPL, upper dashed line). (B) Hearing aid fitted to prescription with the intention of reducing tinnitus audibility. The hearing aid was first adjusted so that output to a moderate intensity stimulus (in this instance, 65 dB SPL composite noise) matched the DSL[i/o] aided target. Ambient sound was amplified to exceed hearing threshold across as wide a frequency range as the hearing aid allowed. Finally, the response to a high-level sound (90 dB SPL swept tone) was measured to ensure that in amplifying soft sounds to audible levels, loud sounds did not exceed measured tolerance levels. The method described is viewed as an easily implemented means to estimate appropriate amplification levels for tinnitus management. The final setting for hearing aid trial would be modified further based on listener preference.
Follow-Up
At each appointment the premise for the fitting of hearing aids is reiterated, and experiences with the hearing aids are discussed. Fine-tuning of the aids is tailored to ensure that they meet the particular patient’s communication needs assisted by the individual’s subjective report in a diary of listening experiences. Once the communication goals have been achieved, the emphasis of tuning changes to reduction of tinnitus audibility. Any adverse response to the hearing aids needs to be addressed so as not to heighten tinnitus focus. Patients are initially encouraged to wear their aids as often as possible, with the intention that they will wear them most of the day once the fitting process has been completed. Depending on their lifestyle, patients may predominantly use the hearing or tinnitus program. Importantly, patients are counseled that both settings are designed to assist in tinnitus reduction. They are instructed to use the hearing program in situations in which communication is likely, and the tinnitus program when in quiet environments. Sources of ambient sound to be amplified are discussed. When in quiet environments patients are encouraged to listen to music, in particular music that evokes positive emotions for the individual. Music that diverts attention and is vigorous is recommended for short-term relief from the tinnitus at its worst, whereas slower pieces of music that enable a progression to a relaxed state may be more helpful in the longer term (Hann, 2003). On occasion a separate hearing aid program may be necessary to enable comfortable amplification of music (Chasin, 2004).
What Should Be Done If Hearing Aids Alone Do not Help the Tinnitus?
Although most patients report immediate benefit in reducing tinnitus annoyance when wearing hearing aids, some do not. Rarely, patients may report an increase in tinnitus, whereas other patients report no change. Possible reasons for such results are discussed here.
Decreased Sound Tolerance
Intolerance to sounds can accompany tinnitus and can create a potential barrier for management using hearing aids. When patients complain that hearing aids exacerbate their tinnitus, it is often found that the maximum output of the hearing aids had been set above the particular patient’s loudness tolerance levels. To accommodate reduced loudness tolerance, extra caution must be applied in selecting appropriate hearing aid settings. In such cases optimal amplification of speech sounds may have to be sacrificed and preference instead given to comfort and amplification of soft sounds. Wide dynamic range compression amplification with low-compression kneepoints (below 40 dB SPL) and high-compression ratios (1:2 or greater) and low maximum output levels (<100 dB SPL) are chosen. If necessary, gain is reduced across inputs and is gradually increased as sound tolerance permits. As long as the sound intolerance is not severe, management of the tinnitus can occur concurrently. When a patient cannot tolerate any amplification, combination instruments are used. In these cases low-level broadband sound is used initially, as in tinnitus retraining therapy (Jastreboff and Jastreboff, 2000), but the noise is progressively withdrawn and replaced by amplified sounds when change in tolerance levels allow.
Combination Instruments
If patients have moderate to severe hearing loss, combination hearing aids and noise generators (tinnitus instruments) may be more suitable than hearing aids alone. For these hearing losses, the large amount of gain required to make quiet sounds sufficiently loud to partially mask tinnitus may not be possible, or may result in acoustic feedback. In these cases masking noise replaces ambient sound as the best means to reduce tinnitus audibility in quiet. For severe to profound hearing losses, sound therapy of any kind becomes increasingly difficult because amplification of quiet ambient sound to audible levels is unlikely to be achieved, and therapeutic noise may be of insufficient intensity to be heard. Alternatively, the noise level may exceed safety recommendations for intensity and duration of exposure (McFadden, 1982). Some of these patients may be candidates for cochlear implants and receive some tinnitus relief from electrical stimulation (McKerrow et al, 1991; Staller, 1998; Tyler, 1995).
Assistive Listening Devices and Tinnitus
Another relevant consideration is whether or not a patient has a hearing loss. In very quiet environments there may be insufficient background sound to reduce tinnitus audibility. Assistive listening devices such as FM radio aids and infrared and loop systems are employed to enhance the signal-to-noise ratio and/or to amplify sound to connected individuals, sparing others in the room who are not connected. These devices also can be used with tinnitus sufferers to transmit background noise or music directly to the user’s receiving device. This strategy can be very important for those patients who spend most of their day in quiet environments.
Many patients listen to music or background sounds at night when attempting to sleep (see Chapter 9). Music players or bedside maskers are often used, but this sometimes annoys a bed partner. This is helped by pillow speakers, but another option is assistive listening devices (whether or not a hearing loss is present). Some patients have told us they use their hearing aids and assistive devices to achieve a reduction in tinnitus audibility when lying in bed. In this situation they turn off the aid’s microphone to eliminate the feedback that would normally occur when an aided ear is placed on a pillow.
The Future of Research
There has been a relative paucity of research into the use of recent and emerging hearing aid technologies in tinnitus management. The flexibility of current hearing aid technologies may lead to the development of fitting approaches specifically intended for the reduction of tinnitus. Future tinnitus research involving hearing aids needs to be more explicit as to the nature of the devices used and how they were fitted.
Conclusion
• Hearing aids are useful in managing tinnitus when combined with counseling.
• Amplification of speech serves to divert attention away from tinnitus.
• Amplification of ambient noise serves to partially mask tinnitus.
• The most effective hearing aid settings for communication are not necessarily the best for reducing tinnitus audibility.
• It is suggested that multiple program hearing aids are fitted with settings optimized for communication and another optimized for amplification of quiet background sounds.
• Fitting the hearing aids using the DSL[i/o] fitting formula is suggested as a starting point for prescribing appropriate amounts of amplification for the partial masking program.
References
Andersson G. A cognitive-affective theory for tinnitus: experiments and theoretical implications. In: Patuzzi R, ed. Proceedings of the Seventh International Tinnitus Seminar. Perth: University of Western Australia; 2002:197–200
Bray V, Nilsson M. What digital hearing aids can do: another perspective. Hearing J 2002;55(4):60–64
Chasin M. Hear the music … or not? Hearing J 2004;57(7):10–17
Coles RRA. Tinnitus and its management. In: Kerr AG, ed. Scott-Brown’s Otolaryngology. London: Butterworths; 1985:368–414
Cornelisse L, Seewald R, Jamieson D. The input/output formula: a theoretical approach to the fitting of personal amplification devices. J Acoust Soc Am 1995;97(3):1854–1864
Dillion H. NAL-NL1: A new procedure for fitting non-linear hearing aids. Hear J 1999;52(4):10–16
Dillion H. Hearing Aids. Turramurra, Australia: Boomerang Press; 2001
Dillion HG, Birtles G, Lovegrove R. Measuring the outcomes of a national rehabilitation programe: normative data for the Client Orientated Scale of Improvement (COSI) and the Hearing Aid Users Questionnaire (HAUQ). J Am Acad Audiol 1999;10(2):67–79
Feldmann H. Homolateral and contralateral masking of tinnitus by noise-bands and by pure tones. Audiology 1971;10(3):138–144
Hallam RS, Rachman S, Hinchcliffe R. Psychological aspects of tinnitus. In: Rachman S, ed. Contributions to Medical Psychology. Oxford: Pergamon; 1984:31–53
Hann D. The elements of music which aid in the management of tinnitus [master’ thesis]. Auckland: The University of Auckland; 2003
Hawkins DB, Ball TL, Beasley HE, Cooper WA. Comparison of SSPL90 selection procedures. J Am Acad Audiol 1992;3(1):46–50
Hawkins DB, Mueller HG. Test protocols for probe-microphone measurements. In: Mueller HG, Hawkins DB, Northern JL, eds. Probe Microphone Measurements. San Diego: Singular; 1992:259–268
Hazell J. The TRT method in practice. In: Hazell J, ed. Proceedings of the Sixth International Tinnitus Seminar. London: Tinnitus and Hyperacusis Centre; 1999:92–98
Hazell JWP, Woods SM, Cooper HR, et al. A clinical study of tinnitus maskers. Br J Audiol 1985;19:65–146
Jastreboff PJ. Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neurosci Res 1990;8:221–254
Jastreboff PJ. Optimal sound use in TRT: theory and practice. In: Hazell J, ed. Proceedings of the Sixth International Tinnitus Seminar. London: Tinnitus and Hyperacusis Centre; 1999:491–494
Jastreboff PJ, Hazell JWP. A neurophysiological approach to tinnitus management. Br J Audiol 1993;27:7–17
Jastreboff PJ, Jastreboff JMM. Tinnitus retraining therapy (TRT) as a method for treatment of tinnitus and hyperacusis patients. J Am Acad Audiol 2000;11:162–177
Kuk FK, Tyler RS, Russell D, Jordan H. The psychometric properties of a tinnitus handicap questionnaire. Ear Hear 1990;11(6):434–445
May A. Multi-microphone instruments, DSP and hearing-in-noise. Hearing Review 1998;5(7):42–45
McFadden D. Tinnitus: Facts, Theories and Treatments. Washington, DC: National Academy Press; 1982
McKerrow WS, Schreiner CE, Snyder RL, Merzenich MM, Toner JG. Tinnitus suppression by cochlear implants. Ann Otol Rhinol Laryngol 1991;100(7):552–558
Meikle, MA, Griest SE, Stewart BJ, Press LS. Measuring the negative impact of tinnitus: a brief severity index [abstract]. Association for Research in Otolaryngology 1995;18:167
Melin L, Scott B, Lindberg P, Lyttkens L. Hearing aids and tinnitus: an experimental group study. Br J Audiol1987;21(2):91–97
Moreland JB. Ambient noise measurements in open-plan offices. J Acoust Soc Am 1988;83(4):1683–1685
Pluvinage V. Rationale and development of the ReSound system. In: Sandlin RE, ed. Understanding Digitally Programmable Hearing Aids. Needham Heights, MA: Allyn & Bacon; 1994:15–39
Ricketts T, Mueller HG. Making sense of directional microphone hearing aids. Am J Audiol 1999;8(2):117–127
Ross M. Binaural versus monaural hearing aid amplification for hearing impaired individuals. In: Libby ER, ed. Binaural Hearing and Amplification. Chicago: Zenetron; 1980:1–21
Saltzman M, Ersner M. A hearing aid for the relief of tinnitus aurium. Laryngoscope 1947;57:358–366
Sanchez L, Stephens D. Survey of the perceived benefits and shortcomings of a specialist tinnitus clinic. Audiology 2000;39(6):333–339
Sandlin RE, Olsson R. Evaluation and selection of maskers and other devices used in the treatment of tinnitus and hyperacusis. Trends in Amplification 1999;4(1):6–26
Schweitzer C. Development of digital hearing aids. Trends in Amplification 1997;2(2):41–77
Sheldrake JB, Coles RRA, Foster JR. Noise generators (“maskers”) for tinnitus. In: Reich GE, Vernon JA, eds. Proceedings of the Fifth International Tinnitus Seminar. Portland, OR: American Tinnitus Association; 1996:351,352
Staller SJ. Suppression of tinnitus with electrical stimulation. In: Vernon J, ed. Tinnitus: Treatment and Relief. Boston: Allyn & Bacon; 1998:77–90
Surr RK, Kolb JA, Cord MT, Garrus NP. Tinnitus Handicap Inventory (THI) as a hearing aid outcome measure. J Am Acad Audiol 1999;10(9):489–495
Surr RK, Montgomery AA, Mueller HG. Effect of amplification on tinnitus among new hearing aid users. Ear Hear 1985;6(2):71–75
Trine TD, Van Tasell D. Digital hearing aid design: fact vs. fantasy. Hearing J 2002;55(2):36–42
Tyler R. Tinnitus in the profoundly hearing-impaired and the effects of cochlear implants. Ann Otol Rhinol Laryngol Suppl 1995;165:25–30
Tyler RS, Bentler RA. Tinnitus maskers and hearing aids for tinnitus. Semin Hear 1987;8(1): 49–62
Vernon JA, Meikle MB. Tinnitus masking. In: Tyler R, ed. Tinnitus Handbook. San Diego: Singular; 2000:313–355
Von Wedel H, Von Wedel U, Walger M. Tinnitus masking with tinnitus-maskers and hearing aids: a longitudinal study of efficacy from 1987 to 1993. In: Vernon JA, ed. Tinnitus Treatment and Relief. Needham Heights, MA: Allyn & Bacon; 1998:187–192
Wilson PH, Henry JL, Andersson G, Hallam RS, Lindberg P. A critical analysis of directive counseling as a component of tinnitus retraining therapy. Br J Audiol 1998;32(5):273–286
Wise K. Amplification of sound for tinnitus management: a comparison of DSL[i/o] and NAL-NL1 prescriptive procedures and the influence of compression threshold on tinnitus audibility [master’s thesis]. Auckland: The University of Auckland; 2003
< div class='tao-gold-member'>



