In their discussion of the treatment of allergic rhinitis, the authors present key features of the disease and its management, allergen responses, the role of the inferior turbinate, and reviews of outcomes with submucosal resection, total inferior turbinectomy, cryosurgery, laser cautery, radical turbinectomy, submucous turbinectomy, submucous electrocautery, and microdebriber turbinoplasty. The authors discuss radiofrequency ablation and coblation outcomes and complications, along with the role of endoscopic sinus surgery in allergic rhinitis and emphasize the need for Otolaryngologists to be facile with a variety of procedures for best outcomes.
- •
Allergic rhinitis is a widespread condition, and nasal obstruction is a defining and bothersome symptom.
- •
Allergic rhinitis that is refractory to medical therapy may necessitate surgical intervention.
- •
Reduction of the inferior turbinate is the primary means of augmenting the nasal airway in allergic rhinitis patients.
- •
A variety of procedures exist for the surgical reduction of inferior turbinate tissue, including outfracture, submucous resection, laser vaporization, radiofrequency ablation, and coblation.
- •
Septoplasty alone has little role in the treatment of nasal obstruction for allergic rhinitis.
- •
Endoscopic sinus surgery is an important treatment method for allergic rhinitis when it contributes to chronic sinusitis, nasal polyposis, or allergic fungal disease.
- •
No single operation has evolved as the gold standard for treatment of nasal obstruction in allergic rhinitis; instead the surgeon should be familiar and facile with several approaches.
Allergic rhinitis (AR) is a widespread condition that affects millions of patients yearly, and the hallmark complaint of nasal obstruction accounts for one of the most common reasons for outpatient otolaryngologic visits. Comorbid conditions often seen with AR include asthma, otitis media, atopic disease, and various forms of rhinosinusitis. The differentiation between rhinosinusitis and AR is often based on clinical history, associated perennial symptoms, nasal cytology, and response to different medical or surgical therapies. Many interventions exist for the treatment of AR, but the most common surgical interventions are aimed at reducing nasal obstruction to better augment the nasal airway.
Background
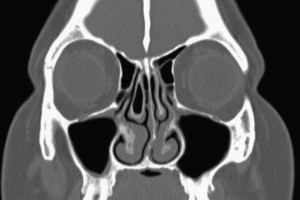
Allergic rhinitis has been described as the “total rhinologic disease,” and requires comprehensive otolaryngologic care. Treatment of patients with AR can be challenging, and has the goal of reducing perennial symptoms while improving quality of life. The disease process can contribute to chronic rhinosinusitis, nasal polyposis, and chronic rhinitis, and therefore AR may be difficult to differentiate from these associated conditions. Patients with chronic AR may also present with fungal disease of the paranasal sinuses or persistent acute sinus exacerbations, often caused by secondary ostial obstruction from edematous sinonasal mucosa ( Fig. 1 ). These coexisting conditions may further complicate patient care.
The incidence of AR is steadily increasing, with up to 24% of the general population having this condition, including approximately 30% of the adult population and 40% of children. More than 600 million patients worldwide are afflicted, making AR the most prevalent atopic disorder. The total direct and indirect cost associated with AR treatment exceeds $5 billion annually. The hallmark symptoms include nasal obstruction, sneezing, seromucosal rhinorrhea, and nasal pruritus. Symptoms may show seasonal or perennial variations, and medical therapy is generally implemented early in the disease process. Systemic symptoms or conditions may also be present with AR, including asthma, bronchitis, pneumonia, and atopic dermatitis. Clinical history is of central diagnostic value, and helps to delineate etiologic factors. Additional allergen testing or serum diagnostics are often used in the workup of patients and to confirm and help direct therapy.
The origin of AR has many contributing factors. The mucosa of the nose and paranasal sinuses is continuous with the lower airway, with only microscopic changes on different levels. Based on this membrane continuum, the association among asthma, certain pulmonary conditions, and AR can be understood. Seasonal variations are often attributed to external factors, such as trees, grass, weeds, and molds. Skin prick, nasal allergen provocation or challenge, intradermal, or in vitro serum–specific testing can delineate allergens and narrow therapeutic regimens. Occupational exposures often contribute to episodic AR, and common triggers include wood dust, latex, spores, or certain chemical irritants. Perennial disease is often caused by indoor allergens, but certain outdoor allergens that are present year-round can also be contributing factors. House dust mites, specifically Dermatophagoides farinae and Dermatophagoides pteronyssinus , pets, and cockroaches are common culprits of perennial AR.
Allergen responses in the nasal mucosa are mediated by a variety of complex interactions among inflammatory markers. IgE is the main mediator of the allergen-allergic response and the resulting sequelae. Mast cells are present in ample quantities in the nasal mucosa, and IgE-mediated binding of allergens initiates a cascade of inflammatory mediator release, both immediate and delayed. Histamine, tryptase, kinins, leukotrienes, and prostaglandins are included in the array of mediators and lead to rhinorrhea. The effects include mucous gland stimulation and increased vascular permeability, resulting in increased secretions, edema, and exudate. Vasodilation leads to engorgement of nasal mucosa and structures, especially the inferior turbinates, thereby causing nasal obstruction, congestion, and discomfort. Inflammation of neuroepithelium and sensory nerve endings cause nasal pruritus and bothersome sneezing. The effects continue in a delayed fashion, causing recruitment and migration of inflammatory cells, including macrophages, neutrophils, and eosinophils. This late phase may persist for hours or days.
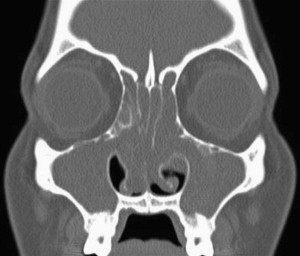
The sequence of events initiated by the allergen also causes secondary sinus ostia closure, which results in negative pressure within the sinus cavities and sets the stage for bacterial invasion. Further reduction in ciliary function leads to accumulation of secretions, bacterial stasis, or biofilm formation. A cycle of sinusitis may ensue and quality of life can be significantly impaired ( Fig. 2 ). First-line treatment includes aggressive nasal hygiene, parenteral therapy, and topical nasal corticosteroids. More complex or persistent disease may benefit from immunotherapeutic desensitization or surgical intervention. Additionally, certain patients are refractory to even long-term medical management, and repeated physician visits for immunotherapy may not be feasible.
The literature agrees that nasal obstruction is the symptom in AR that is most refractory to medical management. It is also perhaps the most important symptom in improving quality of life for these patients. Surgical intervention may be necessary to address this issue, and also to reduce fixed obstruction and aid in dynamic compliance of the nasal airway. Although surgery will not eliminate the inflammation central to AR, additional patency of the nasal fossa reduces the effects of edematous mucosa and may alleviate symptoms. Before the era of endoscopic sinus techniques, septoplasty and inferior turbinate reduction were the classic surgical interventions for the treatment of AR. Neurectomy and selective nasal tissue reduction have been used, though limited data is available to support their routine use. Endoscopic sinus surgery has gained increasing popularity in the past decade and has proven useful, especially when AR contributes to chronic sinusitis, fungal disease, or polyposis. Still, inferior turbinate reduction is perhaps the most common and widely used procedure for treating nasal obstruction in AR that is refractory to medical therapy.
The Role of the Inferior Turbinate in AR
Hypertrophy of the inferior turbinates has long been established as the central cause of symptomatic nasal obstruction in AR. Allergic inflammation causes vasoreactive engorgement of turbinate tissue and associated inflammation of the mucosal lining. The mucosal epithelium of the inferior turbinates has been regarded as the central site for IgE-mediated reactions and nasal eosinophilia. Topical intranasal corticosteroid therapy targets the inferior turbinate epithelium to help attenuate the allergic inflammatory response. In certain refractory cases or in chronic rhinosinusitis, surgical reduction/removal of turbinate tissue may help alleviate symptoms.
The effect of reducing allergic symptoms using surgical reduction of turbinate tissue can best be understood through histologic and anatomic considerations of the inferior turbinate. The lower turbinates have a very important role in nasal physiology and airway compliance. They are bony structures lined with mucosa consisting of ciliated pseudostratified columnar epithelium. The submucosal lamina propria supports this superficial epithelial layer and contains key histologic elements, including parasympathetic nerve fibers, mucous glands, Goblet cells, and abundant vasculature. Hyperplasia of glandular elements within the submucosal layer of the turbinate may worsen nasal obstruction and rhinorrhea in AR. The inferior turbinates modulate inhaled air temperature and nasal resistance, while sharing important mucociliary functions with surrounding nasal tissue. The first points of contact for allergens are the lower turbinates, and deposition in these areas results in localized inflammation stemming from submucosal structures. The goal of surgery of the inferior turbinate is to minimize allergen effects through reducing bulky inflammatory tissue or inducing scar formation, while enhancing patency of the nasal fossa.
Inferior Turbinate Reduction in AR
Over the years, total turbinectomy has become significantly less common and essentially obsolete, partly because of fear of complications such as atrophic rhinitis or empty nose syndrome (ENS). Radical turbinectomy also compromises ciliary function and reduces nasal resistance and humidification. Additionally, technological advances have led to the development of a broader and less-traumatic armamentarium of surgical techniques for turbinoplasty.
Mechanisms accounting for symptomatic improvement in patients with AR after turbinate surgery are likely a combination of various factors. The net mucosal surface may be slightly decreased after volume reduction of the turbinates, thereby reducing available contact points for allergens. Scar tissue develops within the submucosal layer after surgical manipulation, thereby destroying vasculature and glandular structures while impeding regrowth through fibrosis. The reduced volume of the inferior turbinate results in increased nasal patency, allowing the nasal fossa to accommodate swelling of the turbinate from AR. The net effect is improved quality of life through decreased nasal obstruction.
Many techniques are available for turbinate reduction, including classic lateral outfracture techniques, submucosal resection, radiofrequency ablation, coblation, and laser reduction.
Lateralization Outfracture of the Inferior Turbinate
Lateral outfracture of the inferior turbinates has a longstanding history in the otolaryngologic treatment of nasal obstruction. The anterior and inferior portions of the lower turbinate are the main determinants of nasal resistance, and hence are the target of outfracture. Poiseuille’s law states that the laminar flow rate of air along a pipe is proportional to the fourth power of the pipe’s radius. Therefore, small changes in the inferior turbinate will dramatically affect nasal airflow, which is the physiologic basis on which reduction of lower turbinate tissue rests.
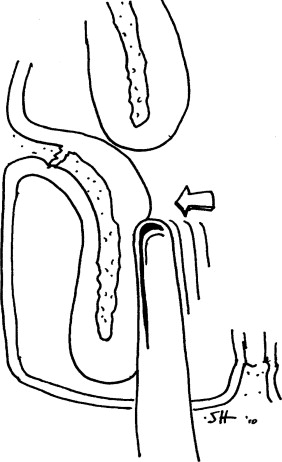
Of all the turbinate reduction techniques, outfracture lateralization is the most surgically conservative and considered the least traumatic to mucosa and surrounding nasal structures. The outfracture procedure was first described by Killian in 1904 as an alternative and replacement to the more historic radical turbinectomy. The risk of nasal adhesions is negligible and there is a minimal chance of developing atrophic rhinitis. Historically, outfracture techniques were thought to produce only short-lasting benefits with a modest increase in nasal patency that is not predictable, especially because the turbinate may medialize over time and symptoms may recur. The classic method is displacement of the inferior turbinate in a lateral, then superior, and then inferior fashion until a crunching sound is heard ( Fig. 3 ). Minor variations exist; some authors prefer to first displace the turbinate in an inferomedial direction, whereas others will add chiseling to the lateral wall attachment to facilitate anterior lateralization.
Aksoy and colleagues evaluated the effectiveness of bilateral turbinate outfracture in 40 patients as a function of the angles and distances between the inferior turbinate and lateral nasal sidewall on paranasal coronal CT scans. They found statistically significant reductions in the angle and distance between the inferior turbinate bone and lateral nasal wall and the area lateral to the inferior turbinate. This reduction was sustained at 6 months postoperatively, leading the authors to conclude that medialization does not occur in at least the first 6 months after outfracture. In general, lateralization outfracture of the inferior turbinate is a safe and simple method of enhancing nasal patency and can be accomplished with routine instrumentation. Additionally, there is virtually no disruption of mucosa and sensory afferents or risk of damage to surrounding structures, including the nasolacrimal system. Further studies with large patient populations are needed to evaluate the long-term efficacy of lateralization outfracture.
Laser Vaporization of the Inferior Turbinate
Six basic laser systems are available for the treatment of hypertrophic inferior turbinates: carbon dioxide (CO 2 ), diode, neodymium-yttrium aluminum garnet (Nd:YAG), potassium-titanyl phosphate (KTP), argonion, and holmium-yttrium aluminum garnet (Ho:YAG) lasers. Each laser differs slightly in depth of penetration and the optimum chromophore. Cited benefits of laser therapy include enhanced hemostasis, reduced postoperative pain, and improved healing.
The concept of laser therapy is to prevent excessive mucosal damage or bony exposure while inducing fibrosis and reducing turbinate bulk and surface area. Vaporization of the entire turbinate has been reported but is not widespread. The laser may be applied in a linear fashion, anterior-to-posterior stripes, cross-hatching across the entire mucosal surface, or along only the anterior or inferior aspect of the turbinate. Spot treatment based on obvious areas of edema or inflammation or any combination of these techniques may also be used for increased efficacy.
The effect of laser therapy on allergen-mediated responses of the inferior turbinates has been studied in histochemical models. Elwany and Abel Salaam reported on 15 patients undergoing CO 2 laser ablation turbinoplasty. Biopsy specimens taken 1 month after laser treatment showed many disorganized seromucinous acini in a background of dense fibrous stoma. Electron microscopy showed an overall reduction in the number of active nasal glands, likely accounting for the postoperative reduction in nasal rhinorrhea. Although this study included specimens only up to 1 month postoperatively, other authors have verified the long-term histologic changes induced by the laser.
Caffier and colleagues recently reported on the effects of diode laser turbinoplasty on 40 subjects, both seasonal and perennial sufferers. Some patients had concomitant septal or middle turbinate pathology that was also addressed, but overall, 95% of patients had diode laser inferior turbinoplasty. The investigators noted statistically significant improvements in both objective rhinomanometry and subjective scores for nasal obstruction, rhinorrhea, sneezing, and nasal pruritus. The improvement was greatest in symptomatic nasal obstruction and was initially higher in perennial patients, but was more sustained in the seasonal rhinitis population. No significant group differences were seen in symptoms of rhinorrhea, sneezing, or itching. Overall, 80% and 65% of patients experienced a stable, nonmedicated course at 1 and 2 years, respectively. In some cases, bony exposure of septal crests or spurs occurred, but no significant long- or short-term adverse outcomes were seen.
Takeno and colleagues prospectively compared CO 2 laser partial turbinectomy in perennial and seasonal patients, and noted initially less-pronounced improvement in sneezing and rhinorrhea in the seasonal group and greater cross-sectional enlargement of nasal cavity volume in the perennial group. These findings led the authors to conclude that laser therapy may be beneficial for acute seasonal exacerbations, but the effects may not be maximally therapeutic until later in the allergy season. Supiyaphun and colleagues found no statistically significant differences in total airway resistance assessed by rhinomanometry after KTP turbinoplasty, although improvements in total inspired nasal airflow were noted.
Overall, symptomatic improvement from laser turbinoplasty and turbinectomy is varied in the literature, from 50% to 100% effectiveness. Proponents advocate less postoperative pain, better hemostasis, and more precise delivery of focused energy to achieve results. Additionally, the use of in-office lasers obviates the need for general anesthesia. Although lasers have a very low side-effect profile, the equipment can be expensive, bulky, and unavailable in many medical centers. Complications include crusting, synechiae formation, and bony exposure of nasal structures.
The Role of Submucosal Resection
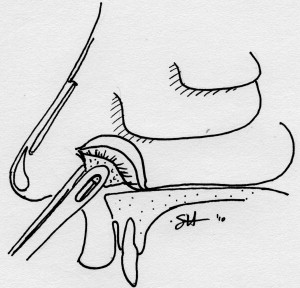
The classic procedure of submucous resection involved an incision and the raising of a mucosal flap on the medial/septal side of the lower turbinate, followed by resection of bone with forceps ( Fig. 4 ). The mucosa overlying the inferior meatus on the lateral aspect of the inferior turbinate was often also removed, and the medially conserved mucosa was then redraped over the resection site. Over time, the term submucous resection has become somewhat unclear and is now used throughout the literature in reference to a variety of techniques, including thermal ablation of cavernous submucosal tissue, laser reduction, and powered instrumentation. Navigating the literature, one will find that submucous resection is used loosely and the specific technique may not be elucidated. The authors advise the judicious use of the term submucous resection and instead recommend naming and clearly describing the specific technique used. When referencing submucous resection of the inferior turbinate, this term should be reserved for the classic open technique.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


