In the United States, roughly 20% to 25% of the general adult population is afflicted by some form of chronic allergic respiratory disease, making allergy one of the most commonly diagnosed disorders. Among children, allergic disease is more common, with some sources estimating that it affects up to 40% of children. The focus of this article involves making the diagnosis of the most familiar and best understood of the hypersensitivity reactions, type 1 hypersensitivity, also termed immediate hypersensitivity. Although type 1 hypersensitivity can be caused by ingestion of food antigens or pharmaceuticals, this article focuses on IgE-mediated allergic disease caused primarily by inhalant allergens.
- •
Allergic disease affects multiple systems through one common immunologic mechanism of IgE-mediated response, and its symptoms can range from annoying to life threatening.
- •
A thorough exploration of symptoms, including timing, patient location when symptomatic, and duration/onset of symptoms, will help the physician determine if allergic disease is present and which possible antigens are potentially responsible.
- •
Testing for the presence of IgE-mediated disease is performed by either skin testing or in vitro testing.
- •
Both types of testing methods are valid and the choice of testing methods is influenced by a number of different factors.
- •
Patient history should guide the selection of antigens for testing and support clinical decision making.
In the United States, roughly 20% to 25% of the general adult population is afflicted by some form of chronic allergic respiratory disease, making allergy one of the most commonly diagnosed disorders. Among children, allergic disease is more common, with some sources estimating that it affects up to 40% of children. The social and economic burden of allergic disease is substantial, with allergic rhinitis alone responsible for 3.5 million missed days of work and more than $6 billion spent on prescription medications alone for its treatment in 2000. This does not take into account loss of productivity, physician office visits, over-the-counter medications, or other costs associated with additional manifestations of allergic disease.
Allergic disease affects all ages, ethnicities, and socioeconomic classes, and occurs throughout the United States, accounting for a large number of physician visits annually. Basically, allergy is the undesirable clinical manifestation of an exaggerated immunologic response to an otherwise harmless antigen. These responses also are known as hypersensitivity reactions and are classified further into several different types, depending on the immunologic mechanism of the reaction. The focus of this article involves making the diagnosis of the most familiar and best understood of the hypersensitivity reactions, type 1 hypersensitivity, also termed immediate hypersensitivity. This diagnosis is made through a combination of eliciting symptoms from the patient’s history, noting physical examination findings, and testing for evidence of immunoglobulin E (IgE)-mediated disease by either some form of skin testing or in vitro testing.
Type 1 hypersensitivity reactions are IgE mediated, and the process of IgE production in response to exposure to an allergen is termed atopy. Although type 1 hypersensitivity can be caused by ingestion of food antigens or pharmaceuticals, this article focuses on IgE-mediated allergic disease caused primarily by inhalant allergens. In addition to allergic disease and allergic rhinitis, there are other types of rhinitis and disorders that may be similar or confused with true allergic disease, and should be included in the physician’s differential diagnosis. These are discussed in other articles within this publication.
Inhalant allergic diseases can manifest in a variety of organ symptoms, but, generally, complaints are focused on the head and neck and upper airways. All types of allergic complaints tend to be grouped together under the term “allergic rhinitis,” as the myriad of symptoms all result from a single common pathogenesis. Much of the allergy literature centers around the diagnosis and management of allergic rhinitis, although the disease manifestations typically are not isolated or restricted to the nose.
At the beginning of taking a patient’s allergy history, the patient may state on questioning that he or she ‘‘has allergies.’’ This self-diagnosis may or may not be accurate and a patient’s self-diagnosis should not be passively accepted without further query to establish the likelihood of allergic disease. Nonallergic triggers may cause symptoms that are identical to allergic disease; however, it is just as common for patients to be completely unaware that the main cause of their complaints is allergy. A good example is the patient with frequent sinus complaints who often feels ill from repeated infections. Many times, the cause is an underlying allergic pathology, not sinusitis. History taking and testing for evidence of IgE-mediated disease are important steps in determining whether or not the diagnosis of allergic disease is appropriate for each patient.
History: inhalant allergies
For any patient with chronic or recurrent upper respiratory complaints, the diagnosis of allergic disease should be considered. Food allergy or hypersensitivity has some crossover manifestations similar to inhalant allergic disease but this article focuses on inhalant allergic disease. For all types of allergy, though, the patient’s history is the single most important source of information in making the diagnosis of atopy. Additionally, there are various inflammatory conditions of the head and neck for which allergy may be a contributing factor to the underlying disease process. For some patients with head and neck symptoms, complete improvement may not occur unless the associated allergic issues also are addressed.
For the allergic history, the history of present illness can be broken down into 3 essential components: symptoms (ie, what they are), timing (ie, onset, duration, seasonality), and location/environment (ie, types of exposures, geography). In reality, a discussion of the patient’s symptoms will not occur in isolation; that is to say, the patient will not generally relate a history of itchy eyes (ie, symptom) without mentioning when this occurs (ie, timing) or where (ie, location). If the patient does not, the physician will promptly question the patient at that point about timing and location for that particular symptom, rather than elicit all possible symptoms before moving on to discover the timing and location of each. Although the performance of the patient interview will be more fluid in actuality than what is described here, the mechanics of the patient history have been isolated into the essential components as an aid in understanding. Family history and past medical history are also very important to elicit but come later in the patient interview.
Common and Important Aspects of History for Inhalant Allergies
The potential number and kinds of questions that could be asked of the patient during the allergy history are almost infinite. The purpose of this portion is not to present an exhaustive list of all questions that should be considered. Rather, for practicality’s sake, the most common and important aspects of the history are covered. However, the reader should keep in mind that an allergic history is like a detective story or a murder mystery. Not all the facts or clues are presented in the initial setting, but are discovered over a period of time and not all are relevant or completely accurate. Information vital to identifying the culprit allergen may be missing and the physician will need to further investigate areas outside what is most commonly encountered. The history of the allergic patient is an ongoing process, not just an occurrence at the initial visit, and continues over the course of the physician-patient relationship. This becomes very important if the patient develops recurrence of allergic symptoms or onset of new allergic symptoms. The detective must remember his magnifying glass and begin to search for more clues.
Patient Symptoms in Allergy
The first type of “clue” to consider is the patient’s specific symptoms. Sneezing; itchy, red, or watery eyes; and clear rhinorrhea are common, well-known allergic symptoms. Wheezing, particularly expiratory wheezing, coughing, urticaria, complaints of increased mucus, and shortness of breath are more potential allergic symptoms. However, other less specific symptoms may indicate allergy, such as complaints of nasal congestion; frequent sinus infections; change in hearing, ear pressure, or pain; the feeling of ears being stopped up; itchy throat; hoarseness; heartburn; and gastrointestinal upset. In addition, other disease processes, such as obstructive sleep apnea, eustachian tube dysfunction, asthma, and chronic rhinosinusitis can be exacerbated by inhalant allergies, so it is critical that the practitioner investigate the presence of allergic symptoms.
Timing of Symptoms in Allergy
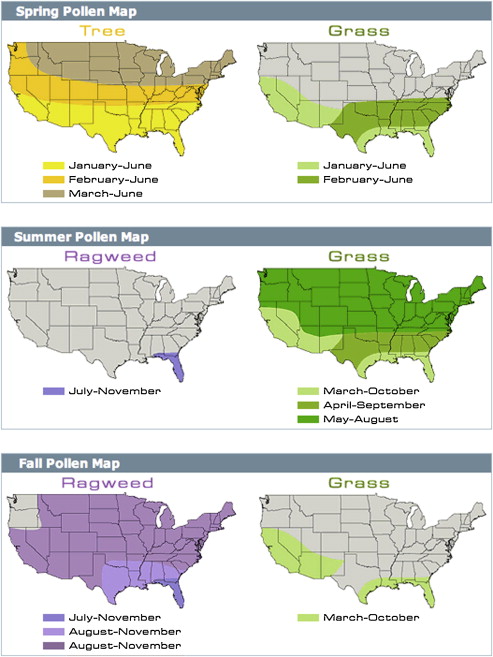
The timing of symptoms is helpful to establish in diagnosing allergy. Timing includes onset of symptoms (ie, both age at onset and duration of symptoms), fluctuation or seasonality (ie, only in the spring vs year round), and symptom pattern. The age of onset is important because onset of true inhalant allergies is rare in the infant and geriatric populations, but more common in the teen and young adult ages, peaking at around age 30. Duration of symptoms includes not only the time frame of onset (ie, How many years have you had this complaint?) but also time course of symptoms (ie, I only sneeze for a week or my eyes itch most of the year). Questions about the time course of symptoms overlap somewhat with questions about fluctuation or seasonality, but the key thing to identify is if the symptom occurs periodically, associated with a season or location, or perennially. Whether the symptoms are present year-round or only during certain seasons is very helpful in diagnosing perennial versus seasonal allergic disease. Fig. 1 demonstrates examples of the seasonal pattern and distribution by geographic location of a few common inhalant allergens. This type of information can be very helpful in the investigation of allergic symptoms. Establishing any symptom patterns is crucial as well. If multiple symptoms are elicited, do they all occur together or only certain ones? This helps the physician track down potential suspect allergens and aids in identification of which allergen is causing which symptom or symptom pattern.
Location and Environment in Allergies
Location and environment complete the critical elements of information to obtain in the history of present illness. The current geographic location helps establish what potential aeroallergens the patient is exposed to, but previous locations where the patient has lived are also important. A significant change in environment, such as a cross-country move, with exposure to new allergens, can be factor in the development of allergies in the adult population, so it is important to elicit this history when seeing a new patient with allergic-type symptoms. Questions of timing overlap with location and environment as the patient’s fluctuations in symptoms may not necessarily be seasonal but related to local exposures at work or home. The list of environmental exposures can be exhaustive when considering home, outdoor, and occupational environments, but key things to inquire about are the presence of pets (indoor or outdoor) or livestock, tobacco use, hobbies, stuffed animals, carpeting or draperies in the domicile, type of heating or air conditioning, indications of mold or humidity, and nearby landscaping. Certainly it is impossible during one session to investigate all possible exposures, but if the allergic patient is not improving with appropriate treatment, it can be highly beneficial to review additional environmental exposures.
Past Medical History and Family History in Allergies
Additional components of the allergic history are past medical history and family history. Past medical history should include a review of any previous treatments or testing, surgeries, particularly past sinus surgery, and medications. Previous treatment includes not only treatment the patient may have received from a physician, such as previous skin or in vitro testing or immunotherapy, but also self-administered medications, such as over-the-counter antihistamines and cold preparations. The effectiveness of any previous treatment should be documented. A thorough review of medications is important, as certain medications, like tricyclic antidepressants and antihistamines, can effect skin reactivity or increase the risk of certain testing and treatment options, such as beta-blockers or angiotensin-converting enzyme (ACE) inhibitors. Family history is also key historical information. Allergic disease is hereditary, and other family members usually will be affected by the same or similar complaints as the patient.
Diagnostic testing
Not all patients with allergic rhinitis or atopic disease require confirmatory diagnostic testing. The patient’s history and physical examination are sufficient to make the diagnosis of allergic disease in most cases. If appropriate medical therapy is instituted and it controls the patient’s symptoms, then no further workup or testing is needed. However, if medical therapy fails or incompletely resolves the patient’s symptoms, the patient wishes to implement environmental control measures and wants guidance on what to avoid, or wishes to receive allergy immunotherapy, then proceeding with diagnostic testing is appropriate. It is important to note that although diagnostic testing does not necessarily mean that the patient must proceed with immunotherapy, immunotherapy cannot commence without the evidence of IgE-mediated disease that diagnostic testing provides. A patient who undergoes diagnostic allergy testing with negative results is not a candidate for immunotherapy.
Diagnostic allergy testing for inhalant allergens includes selecting a type of in vivo testing (ie, skin testing) or in vitro testing. The decision as to which testing method the physician chooses to use can be a complex one and is influenced by a number of factors. Some of these factors are discussed in the following paragraphs with each different type of testing method and are also discussed toward the end of the article. The following described testing methods are all considered acceptable standard medical practice and the author does not espouse one technique over the other.
Skin Testing in Allergies
Skin testing generally involves prick testing, intradermal testing, or a combination of the two testing methods, such as modified quantitative testing (MQT). For all types of skin testing, appropriate types of positive histamine controls and negative controls must be placed at the start of testing to confirm the validity of any positive or negative skin tests. The type of negative control used will depend on any diluents used in the antigen testing vials. If an antigen is presented in a mixture containing 50% glycerin, then 50% glycerin should be used as the negative control and so forth. Skin testing has the advantage of providing the patient with an immediate answer as to which allergens do or do not potentially cause his or her symptoms but it can be time consuming, carries the risk of a systemic reaction or anaphylaxis, and involves some discomfort. Its accuracy is also subject to medication effects and skin disorders, so not all patients may be eligible candidates for skin testing. Patients with dermatographism or active eczema, who are actively taking antihistamines or antihistamine-containing over-the-counter cold preparations, or who are on beta-blockers are just a few examples of patients who are more appropriate for an alternative method of allergy testing, such as in vitro allergy testing.
Prick Testing in Allergies
Prick testing can be used to confirm clinical sensitivity to inhalant and other types of allergens and can be done in a number of ways with different devices. Prick testing is a type of epicutaneous test and involves placing an antigen concentrate on the patient’s skin after small, superficial punctures have been made to the epidermis, placing the antigen concentrate on the skin, and making a small puncture through the concentrate, or using a device that applies the antigen concentrate to the skin at the same time the puncture is made ( Fig. 2 ). These devices can be either a single-prong device or a multiprong device ( Fig. 3 ) or the testing can be done with needles or lancets. There are no objective data comparing devices that support a clear-cut advantage of using one type of device over another and good results can be achieved with any device, as long as there is consistency in its use and proper training.


After a period of time, generally 15 to 20 minutes, any resulting wheals are noted and measured. Assuming appropriate responses to control tests, the size of any resulting wheals can be graded, termed “qualitative scoring,” and used to confirm presence of allergic disease or can be used to guide placement of an intradermal test, if a blended technique like MQT is used. There are a variety of wheal-grading systems and scales that categorize size of the resulting wheal and erythema (ie, flare reaction); an example of one such grading system for classifying wheals is in Table 1 . Many practitioners no longer grade wheals because of the demonstrated variability between physicians, and solely judge wheals as positive or negative. If a grading scale is used, which scale or system is used is not so important as the consistency of its application. Depending on the system or scale used, +3-sized or +4-sized wheals are considered positive and a wheal smaller than 3 mm is considered negative.
| Grade | Wheal Size |
|---|---|
| 0 or Negative | Less than 3 mm |
| +1 | 3 mm to 5 mm |
| +2 | 6 mm to 10 mm |
| +3 | 11 mm to 15 mm |
| +4 | Greater than 15 mm or pseudopods |
Intradermal Testing in Allergies
Intradermal testing involves injecting dilute solutions of antigenic material into the patient’s dermis. This can be a single intradermal injection placed after a negative prick test, as part of a blended testing method, or as a part of a progressively stronger series of dilutions, such as intradermal dilutional testing (IDT). Intracutaneous tests, such as intradermal tests and the various intradermal testing techniques, are more sensitive and will identify a large number of patients with lower skin sensitivity than epicutaneous tests, like skin-prick testing.
In general, a small needle is used to inject a dilute quantity of antigen into the superficial dermis, raising a wheal of roughly 3 to 4 mm in size ( Figs. 4 and 5 ). Appropriate positive and negative controls are placed for intradermal tests as well. If a positive control has been placed for prick testing, then a subsequent positive control for intradermal testing is not necessarily needed if the prick test positive control was positive and the prick test negative control was negative. It is important to note, however, that if no positive control was previously placed, an intradermal positive histamine control is placed, which is different from that placed for prick testing. This type is generally an aqueous form of histamine in a more dilute strength. A negative control is almost always placed, as the diluents used for intradermal testing are different from those used in prick testing and, depending on the concentration of the intradermal dilution used, an intradermal glycerin control or controls may need to be placed if there are suspicions of glycerin sensitivity.




