Sleep-related symptoms are extremely common in patients with allergic rhinitis. Sleep impairment is likely a major contributor to the overall disease morbidity, direct and indirect health care costs, and the loss of work productivity associated with allergic rhinitis. The association between allergic rhinitis and sleep, and the subsequent impact on disease-specific and general health quality of life measures, is well documented in large epidemiologic studies as well as controlled clinical trials. This article focuses on sleep disruption caused by allergic rhinitis, and the therapeutic and surgical options available to tackle the problem.
- •
Allergic rhinitis significantly contributes to sleep-disordered breathing through multiple mechanisms, with the greatest impact mediated primarily through nasal obstruction
- •
Sleep impairment is very common in patients with allergic rhinitis, chronic rhinosinusitis, and nasal polyposis, and has a significant impact on disease-specific and general health quality of life measures
- •
The degree of sleep disturbance is directly related to the severity of the allergic disease at a given time
- •
Nasal obstruction also demonstrates circadian rhythm and positional variability, with worsening in the overnight hours and in the supine position
- •
Nasal obstruction increases the likelihood of snoring, obstructive sleep apnea, and intolerance to medical device therapies for sleep apnea.
Allergic rhinitis and sleep impairment
Scope of the Problem
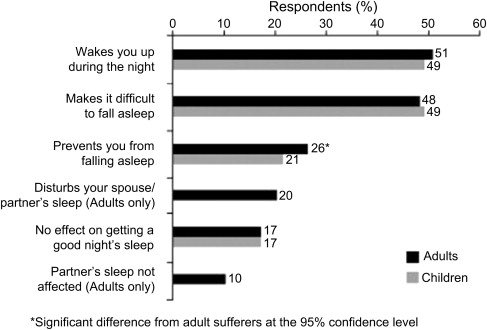
Sleep-related symptoms are extremely common in patients with allergic rhinitis. Sleep impairment is likely a major contributor to the overall disease morbidity, direct and indirect health care costs, and the loss of work productivity associated with allergic rhinitis. The association between allergic rhinitis and sleep, and the subsequent impact on disease-specific and general health quality of life measures, is well documented in large epidemiologic studies as well as controlled clinical trials. In a survey of allergy patients, 48% with seasonal allergic rhinitis (SER) and 68% with perennial allergic rhinitis (PER) reported that their condition interfered with their sleep. In another population survey by Craig and colleagues, of the more than 2000 allergy patients surveyed, approximately half reported difficulty falling asleep or staying asleep as a result of their allergic condition ( Fig. 1 ).
In a large cross-sectional epidemiologic study, Leger and colleagues showed that allergic rhinitis can affect multiple aspects of sleep, with numerous consequences on daytime function. Sleep-related breathing disorders, insomnia, as well as daytime somnolence, morning headaches, and cognitive dysfunction, were all more common in the allergic rhinitis patients than in controls. Furthermore, the degree of sleep impairment and associated symptoms appears to be directly related to the severity of the allergic rhinitis. In patients with seasonal allergic rhinitis, subjective and objective sleep measures correlate with the severity of their sinonasal disease at the time, that is, patients with predominant tree pollen allergy may have noticeable worsening in their sleep during the spring pollen season. As such, sleep disturbance is one of the key factors in the Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines that distinguishes between mild and moderate-severe disease.
Pathophysiology
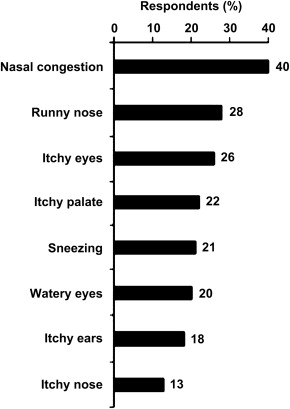
The pathophysiology of disrupted sleep in patients with allergic rhinitis is likely complex and multifactorial. Upper airway resistance, increased work of breathing, obstructive respiratory events, sleep-onset and sleep-maintenance insomnia, anxiety, depression, confounding effects of allergy medication and sedative drugs, as well as other biochemical and hormonal effects all may play a role in the negative impact on sleep quality. Clearly, however, one of the vital and well-established links between allergic rhinitis and sleep disturbance is nasal obstruction. In the large epidemiologic survey by Craig and colleagues, nasal congestion was the most commonly reported symptom of allergic rhinitis patients ( Fig. 2 ).
Several mechanisms have been proposed to explain how nasal obstruction negatively affects breathing during sleep ( Table 1 ). Nasal obstruction may result in decreased stimulation of nasal receptors that are critical to control of breathing during sleep. Abolishment of the nasal receptor reflexes with topical lidocaine appears to increase airway obstruction and depress the central respiratory drive. In a controlled crossover study, patients were evaluated with in-laboratory polysomnography and randomized to either (1) topical nasal saline with decongestant or (2) topical nasal lidocaine (4%) with decongestant, and then subsequently crossed over to the other group for a second night. The mean apnea-hypopnea index (AHI) increased from 6.4 with nasal saline to 25.8 with topical lidocaine. Of note, the increased apneic events observed with topical nasal lidocaine were split between both central and obstructive events, leading the investigators to conclude that nasal receptor stimulation is critical for central respiratory control of ventilation as well as maintenance of pharyngeal muscle tone.
| Acute | Chronic |
|---|---|
|
|
These findings have been supported by additional studies comparing the nasal and oral routes of breathing. Oral breathing appears to have a detrimental effect on sleep, leading to loss of protective pharyngeal muscle activity and loss of control of breathing. The nasal route of breathing, however, has been shown to improve minute ventilation and increase pharyngeal muscle activity. In a randomized single-blind placebo and sham-controlled crossover study, McLean and colleagues compared the impact of the fraction of oral breathing on objective sleep measures. With polysomnography, they demonstrated that patients with lower nasal resistance and a normal nasal route of breathing had decreased light sleep (stage 1), increased deep sleep (slow-wave), increased rapid eye movement sleep (REM), and improved sleep efficiency. Multiple human studies of experimental nasal occlusion support these findings as well, demonstrating abnormal sleep continuity, abnormal sleep architecture, and increased respiratory events in normal patients with experimentally induced nasal obstruction.
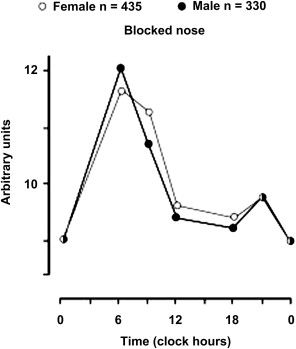
Further contributing to the sleep effects of allergic rhinitis is the diurnal variation of nasal congestion, with a predictable worsening overnight in most patients. This physiology is also likely multifactorial, and attributable to the gravity effect of the dependent sleeping position and a natural decrease in serum cortisol levels overnight. In addition, inflammatory mediators associated with allergic rhinitis demonstrate a circadian rhythm with progressive worsening after midnight in most individuals, peaking in the early morning hours (average peak ∼6:00 am ) ( Fig. 3 ).
Besides the acute nightly effects of allergic rhinitis on sleep, chronic nasal obstruction and persistent allergic disease can also contribute to long-term, potentially irreversible, changes in breathing and sleep as well. These long-term effects are particularly concerning in pediatric allergy patients in whom the craniofacial skeleton is still rapidly developing. Rhesus monkey studies at the University of California, San Francisco in the 1970s compared the craniofacial development in animals with experimental nasal occlusion with that of controls. The studies showed that over time, young animals with chronic nasal obstruction developed maxillary deficiency, posterior/inferior displacement of the mandible, and other severe maladaptive skeletal changes (see Table 1 ), all of which have been associated with sleep-disordered breathing in adulthood. It has been hypothesized that a vicious cycle evolves in some patients in whom nocturnal breathing abnormalities cause unstable oral breathing and secondary impaired craniofacial growth, which then reinforces abnormal breathing.
Nasal Obstruction and Sleep-Disordered Breathing
Several large population-based studies have analyzed the association of nasal obstruction and subjective sleep measures, snoring, and sleep apnea. In the Wisconsin cohort of almost 5000 patients, patients with chronic rhinitis symptoms were more likely to report habitual snoring, nonrestorative sleep, and daytime sleepiness. Patients with nasal congestion due to allergy were 1.8 times more likely to have moderate to severe obstructive sleep apnea (OSA) compared with allergy patients without nasal congestion. Other epidemiologic studies have confirmed that across a large population, nasal obstruction is an independent risk factor for both snoring and OSA.
On the spectrum of sleep-related breathing disorders, nonapneic snoring is a very common condition. In the Wisconsin cohort, patients with chronic nasal congestion had a threefold increased risk of habitual snoring, even after controlling for OSA. Snoring is often the chief sleep complaint in many patients, and subjectively is more important to most patients than daytime sleepiness. Snoring has been shown to disrupt bed-partner sleep and have a negative impact on marital relationships. Further, treatment of snoring not only improves the patient’s sleep but has also been documented to improve the bed-partner’s sleep, with a reduction in the bed-partner’s arousal index and improvement in sleep duration and efficiency.
Recent evidence also suggests that vibratory trauma from snoring may cause direct endothelial injury and may be an independent risk factor for carotid atherosclerosis. Researchers in Australia have developed a rabbit model to evaluate the effects of snoring on the carotid artery. These investigators conclude that significant vibrational energy is transmitted to the carotid arterial wall during snoring, and may provide a link to carotid atherogenesis and cerebrovascular risk. Even in pediatric populations, primary snoring has been directly linked to elevated nocturnal diastolic blood pressure, even after controlling for other clinical factors. In summary, reports of snoring in patients with allergic rhinitis should not be overlooked. What was previously considered “benign” or “simple” snoring may actually have significant psychosocial and physical health consequences.
The Impact of Medical Therapy
It is clear that nasal obstruction can have significant negative effects on both subjective and objective sleep measures as well as on the risk of sleep-disordered breathing. Until recently, however, it has been less clear as to what effect treatment of the nose has on these parameters. If nasal obstruction is the driving force behind much of the sleep disturbance in patients with allergic rhinitis, it would stand to reason that treatment of nasal obstruction and lowering of the nasal resistance would improve sleep in these patients.
Much of the research into medical therapy for allergic rhinitis and sleep-disordered breathing has focused on the role of nasal steroids. In a group of allergic rhinitis patients with subjective nasal congestion and sleep disturbance, Craig and colleagues demonstrated that topical nasal steroid therapy improved subjective sleep quality and daytime function. Pediatric patients with symptomatic nasal obstruction and OSA have also been shown to respond favorably to nasal steroid therapy. Brouillette and colleagues reported a reduction in the AHI from 10.7 to 5.8 with fluticasone nasal spray in a selected group of pediatric patients. Nevertheless, long-term adherence to nasal steroids may be suboptimal and difficult to monitor, particularly in pediatric patients with parental concerns about side effects.
Although treatment of allergic rhinitis and associated nasal obstruction can improve sleep, some of the medical therapy, notably antihistamines, may actually cause sleep-related symptoms. As such, the medical evaluation of allergy patients with nocturnal and daytime sleepiness must also take into account the side effects of the medications used to treat the underlying condition. Oral decongestants (ie, pseudoephedrine) and inhaled β-agonists (ie, albuterol) have been associated with insomnia symptoms in some patients. Conversely, oral antihistamines, particularly first-generation drugs, commonly cause sedation and may, at least in part, contribute to a patient’s complaints of hypersomnia.
The Impact of Surgical Therapy
In many patients with allergic rhinitis, the symptomatic nasal obstruction and sleep-disordered breathing may be attributable to a combination of both inflammatory and structural pathology ( Table 2 ). The management approach to the patient generally involves first identifying and medically treating any underlying inflammatory process that may be present. For structural anatomic problems, surgical therapy can be very effective, but the specific procedures indicated vary from patient to patient and depend on the specific anatomic problem. Benninger and colleagues recently reported that subjective sleep quality improved significantly following endoscopic sinus surgery in patients with chronic rhinosinusitis ( Fig. 4 ).



