(1)
St. Johns, FL, USA
(2)
Helen Keller Foundation for Research and Education, International Society of Ocular Trauma, Birmingham, AL, USA
(3)
Consultant and Vitreoretinal Surgeon, Milos Eye Hospital, Belgrade, Serbia
(4)
Consultant and Vitreoretinal Surgeon, Zagórskiego Eye Hospital, Cracow, Poland
The preparations for performing VR surgery are time-consuming initially, but they become much less so with time: some of the activities need a one-time effort; others become routine. However, the initial preparations are indeed necessary to reduce the unavoidable tension associated with performing complex and high-stake surgery.
Pearl
Inadequate preparation for VR surgery increases the surgeon’s stress level, the complication rate, and is, long term, threatening the surgeon’s physical health as well.
16.1 The OR Personnel
The surgeon should work with a well-trained, well-intentioned, and attentive nurse (see Chap. 6).
Anesthesiologist: if surgery is done under local anesthesia, the anesthesiologist need not be in the OR all the time, but must be available in case the patient’s systemic condition requires his intervention.
Both the nurse and the circulator need to be familiar with the location and details of a list4 that must have been compiled earlier with vital information regarding:
How to mix the intraocular (for injection or infusion) and local (fortified topical, periocular, subconjunctival) medications such as antibiotics and steroids.
How to mix intraocular gases to achieve the required concentration.5
The contact information (name and mobile phone number) for at least two representatives of all companies whose major equipment (vitrectomy machine, laser etc.) is used.6
Pearl
It is highly advisable to have a backup vitrectomy machine available, even if this is an older and less sophisticated one. It is solely for emergency purposes, in case the standard machine breaks down and cannot instantly be brought back to life.
16.2 The Operating Table and the Surgeon’s Chair
16.2.1 The Operating Table
You should be able to adjust the following:
Height.
Inclination angle in either direction.
The head part’s inclination angle (separately; see below, Sect. 16.6).
Ideally, a U-shaped wrist support7 is securely fixed to the table, and its height should also be adjustable (see Fig. 16.1).8 The table’s supporting mechanism must be far enough back from to leave space for the surgeon’s feet to have unhindered access to all three pedals.9
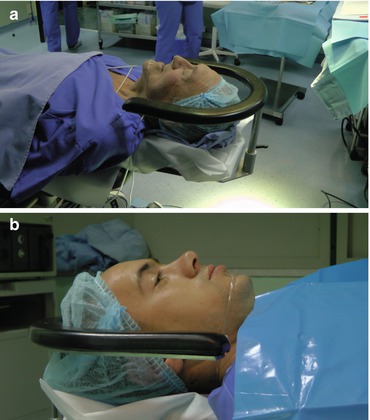
Fig. 16.1
The U-shaped wrist support on the operating table. (a) The “U” should be close enough to the patient’s head so that when the surgeon’s instruments are held in the vitreous cavity, the “U” is supporting the wrist and far enough so that the plastic bag collecting the waste fluid remains accessible (this means that the U’s shape and size need to be optimized to achieve these goals). The “U” must be padded to avoid hard counterpressure on the surgeon’s wrist. (b) The “U” must also be at the correct level as it relates to the eyeball. The most optimal height is for the top of the “U” to be just below the level of the lateral canthus: the one on this image is too low. Placing the “U” lower reduces its efficacy in providing support; if too high, it interferes with access to the eye. The latter is especially obvious when manipulations are needed in the anterior parts of the eye, such as hyphema removal or lensectomy
16.2.2 The Surgeon’s Chair
A well-designed chair should satisfy the following criteria (see Fig. 16.2):


Fig. 16.2
The surgeon’s chair: the good, the bad, and the barely acceptable. (a) A chair that satisfies all demands [SurgiLine (UFSK-International OSYS GmbH, Heidelberg, Germany)]: it easily rolls but has a surgeon-activated break acting on all legs; the legs do not protrude outward; it has a battery to operate its height adjustment; the surgeon has easy access to the pedals for the chair’s up or down movement, yet these pedals are never in the way; the back support is ideally placed; the support for the lower arm is padded and completely mobile in all directions. (b) An acceptable compromise, except that the chair has no breaks, the height adjustment upward is easy for the surgeon to accomplish and to do so in small increments but the down movement is possible only by uncontrolled and large movements, and the armrest is not padded in the back (this becomes a significant issue during a long case or day). (c) A terrible chair, which is shaky, has no breaks, and the height adjustment requires manual work
Wheels so that it can easily be rolled.
Small “footprint”: the legs do not reach too far out, which would prevent the surgeon from moving close to the operating table.
Locking mechanism against rolling and shaking.
The surgeon himself should be able to activate/deactivate the break with a central pedal, and the break should work simultaneously on all wheels.
Batteries to help unclog the OR floor.
Electric, surgeon-operated height adjustment.
Easy-to-adjust arm support that can be moved in several dimensions (up-down; forward-backward; inward-outward both in whole and its distal end). The armrest should easily be secured.
Comfortable padding on the armrests, which also provide support for the lower arm.
Back support, which is adjustable in height and not positioned too far back.
16.3 The Vitrectomy Machine,10 Its Footpedal, and the Arrangement of All the Pedals
Different surgeons prefer different parameters (pump type, aspiration/flow values etc.). Yours should be stored in the machine under your own name.
Always make sure that the display shows you as the surgeon.
The pedal can be programmed, on modern machines, to work in a linear, dual linear, or 3D mode.11
When pressing down with the pedal, the aspiration/flow starts and gradually increases, and eventually cutting kicks in (linear).
Many surgeons use a modified option: they activate the aspiration/flow function by pressing down with the pedal, and they turn the pedal sideways to add cutting as well.12
When pressing down with the pedal, both the aspiration/flow and the cutting start and gradually increase (dual linear).
With pressing down with the pedal, both the cutting and aspiration/flow rates change, but in opposite directions (3D).
As indicated in Table 12.2, I prefer a set cut rate and liner aspiration/flow (linear).
Some vitrectomy machines allow more functions13 to be operated by the surgeon via the footpedal. He has to make an individual decision whether he prefers this option or choose instead the minimalistic one, asking the nurse/circulator to make the adjustment on the machine interface as needed.
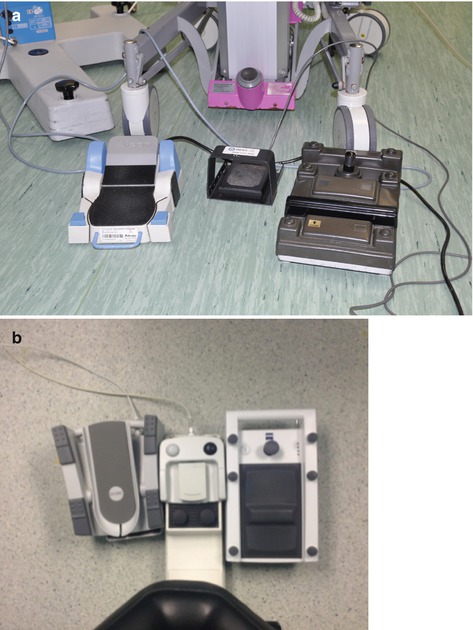
Fig. 16.3
The arrangement of the pedals under the surgeon’s feet. (a) A right-footed surgeon should have the microscope pedal placed on the right and the vitrectomy pedal on the left; the laser pedal is in the middle (to be operated by the left foot). The pedals are angled outward, not parallel with each other. (b) Some surgical chairs come with a built-in anterior platform so that all pedals can (in fact, must) be placed on this. A somewhat cumbersome option, especially if the pedals are too large for the platform, and their position is not secure
Q&A
Q
Why place the microscope pedal under the dominant foot?
A
Because the foot operating the microscope will be much more active during PPV than the foot used to drive the PPV machine. It makes sense to employ the dominant (in 90% of the surgeons the right) foot the active one. This foot must control the X-Y joystick (see below), and the two focus and two zoom pedals. The nondominant foot basically controls the cutting/aspiration functions – with a single movement in my setup version. Both feet, of course, will have additional functions (such as the diathermy by the nondominant and the microscope’s light switch by the dominant foot), but even here the dominant foot will remain more active.
16.4 The Microscope
Before starting the operation or before scrubbing in, adjust the X-Y, zoom, and focus speed.18
Adjust the power of the illumination. The brightness level should be the lowest that still allows you to work on the eye surface.19 You will need to turn on/off the microscope light several times during the operation, even after you have already reached partial or full adaptation. It is unwise to get blinded by the reflection of too bright a light from the sclera or the contact lens.
16.5 The BIOM
For practical reasons, most of the information about using this indispensable tool is presented here (see also Sect. 12.3).
16.5.1 BIOM: The Advantages
See Table 16.1.
Table 16.1
The advantages of the BIOM*
No | Corneal damage since there is no physical contact |
Contamination by blood from the operative fielda | |
Assistant required to hold the lens/system in place | |
Easy | Mounting of the adapter plate |
Removal of the reduction lens | |
Focusing with a wheel that is in a permanent position | |
Exchanging of the front lenses | |
Large selection of | Front lenses for different viewing options |
Superior | Observation angle/surgical field (wide, magnified, combined) |
Resolution | |
Depth of focus | |
Unhindered | Mobility of eyeball during surgery |
Access to eyeball around the swung-in front lens | |
No/little interference fromb | Hazy media (cornea, AC, lens, vitreous) |
Small pupil | |
Microscope mounting and operation | Permanent and easy |
Available for most types of microscopes | |
No interference with the use of microscope-mounted other devices (video camera, laser filter) | |
Automatic SDI activation |
16.5.2 BIOM Use: Practical Information
See Table 16.2.
Table 16.2
Useful hints for BIOM users
Working with (switching to) the BIOM requires some getting used toa | Do not give up after the initial frustration during the first few casesb The benefits soon become obvious if you are persistent, and soon you could not imagine operating without itc |
Microscope’s focus pedal | This is one of the most important adjustments the surgeon must make. Once the BIOM is swung in place, the microscope’s focus pedal does not control the focus anymore, it now changes the field of view: going down makes the field largerd The focus is adjusted using the BIOM’s focusing wheel |
The ideal working distance from the cornea | The front lens should be at ~2 mm from the cornea. This avoids dipping into the visco yet provides the largest possible field If the cornea has to be recoated with visco, it is best to lift the front lens first, but it is not necessary to swing it out |
Scleral indentation | Even when using the widest-angle front lens, scleral indentation is recommended to view the vitreous base |
Working in close proximity to the posterior capsule in phakic eyes | Unless there is substantial cataract to clearly show the border between lens and vitreous, swing out the BIOM to avoid biting into the lens (see Sect. 27.5.3) |
Fine work on the posterior polee | Use a contact lens instead of the BIOM, unless you are a very experienced surgeon (see Sect. 13.1) |
Do not turn the microscope light on while the BIOM is swung in | The light reflex is blinding. Condition your brain to follow these sequences: (1) Microscope light off; (2) BIOM in (1) BIOM out; (2) microscope light on (see also Sect. 16.4) |
16.5.3 BIOM: Setting Up for Daily Use
Follow these steps to optimize the use of the BIOM (see Table 16.3).

Table 16.3
Basic setting up of the BIOM
Variable | Make sure that: |
|---|---|
View through the microscope | The view is sharp for the surgeon’s either eye, even at high magnificationa |
BIOM adapter plate | It is securely fixed to the microscope and the screw is tightened |
BIOM reduction lens | The lens is not too hot and it properly clicked in place |
BIOM | It is securely fixed to the adapter plate |
BIOM front lens | The desired type of lens has been selected It is pushed all the way into its slot The focusing wheel is at the lowest positionb |
Imaging | With the light pipe inside the vitreous cavity, the image is sharpened at the highest magnification of the microscope. The position of the front lens is then appr. 20% higher than the lowest possible point |
Corneal surface | After squirting, it is coated with visco (see Table 16.4) |
The microscope | It is lowered to be close to the eye so that the BIOM front lens is ~2 mm from the surface of the visco; this process is checked by the surgeon viewing it from the outside, not by looking through the microscope (see Fig. 16.4) |
Fig. 16.4
The BIOM front lens. When in position, the lens should be about 2 mm from the top of the visco on the cornea. Note that the distance is measured not from the rim of the lens but from the apex of its inferior dome, which is much closer to the cornea
16.5.4 BIOM: Checklist
There are numerous practical tricks to maintain excellent visualization throughout the operation (see Table 16.4).
Table 16.4
The BIOM checklist per operation
Make sure that youa: | Comment |
|---|---|
Have properly secured all attachments | Pushed all the way in, with screws tightenedb |
Selected the front lens you want to use | Choose from the following lenses: 60° (macula), 70°, 90°, 120°, 60–125° (wide field, high definition). In general, the wider the field, the worse the resolution |
Cleaned both the reduction and front lenses, and they have cooled off | The lenses must be carefully wiped before, occasionally during, the operation; the reduction lens usually only before, the front lens sometimes during the operationc |
Firmly pressed the draping onto the patient’s skin, 360° around | To prevent endophthalmitis from contamination on the skin (or discharge from the nose, see Fig. 15.1) and avoid breath-related fogging |
Gently squirted the corneal epithelium with BSS and then coated the cornea with visco before swinging the BIOM into position | You must avoid splash back from the corneal surface or coating the front lens itself (see Sect. 25.1.4)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|