Key points
- •
Sinonasal and ventral skull base cancers encompass a variety of rare “orphan” tumors. Existing evidence is predominantly from retrospective single-institution series.
- •
Multimodality treatment with surgery and postoperative radiation therapy is the standard paradigm.
- •
Advances including intensity-modulated radiation therapy and charged particle therapy have allowed for improved oncologic outcomes and reduced toxicity.
- •
Radiation oncologists must balance target coverage and critical structure dose to maximize tumor control while minimizing severe toxicity.
- •
Specific radiotherapy considerations vary by histology and location and are important for optimal management.
Introduction
Sinonasal and ventral skull base malignancies are rare tumors; therefore, evidence for optimal management is limited primarily to single-institution retrospective series and population-based registry studies. Initial management is usually maximal surgical resection. Although no randomized trials exist, high rates of local failure have led to the wide adoption of postoperative radiation therapy for all except early-stage tumors without adverse pathologic risk factors. Numerous institutions published their experiences with this approach ( Table 1 ), with most reports spanning at least several decades and encompassing a mix of tumor stages and histologies. These series report 5-year overall survival (OS) rates of roughly 50% and local control (LC) of 50% to 70%. When patients present with unresectable disease or comorbidities precluding surgery, definitive radiotherapy or chemoradiation are used. In these cases, outcomes are suboptimal and toxicities significant as higher doses are needed to control gross disease. In select patients, a reassessment of resectability may occur after completion of definitive radiotherapy.
| Series | Years Treated | n | % Surgery | Results | Conclusions/Toxicity |
|---|---|---|---|---|---|
| Blanco et al, 2004 (WashU) | 1960–1998 | 106 | 65 | 5-y OS 27%, DFS 33%, LC 58% | Better outcomes in those who had surgery |
| Hoppe et al, 2007 (MSKCC) | 1987–2005 | 85 | 100 | 5-y OS 67%, DFS 55%, LC 62% | Only 1 G3+ ocular toxicity using mostly modern techniques (3DCRT, IMRT) |
| Dulguerov et al, 2001 (UCLA, Switzerland) | 1975–1994 | 220 | 71 | 5-y OS 40%, LC 57% | Better outcomes in those who had surgery |
| Chen et al, 2007 (UCSF) | 1960–2005 | 127 | 84 | 5-y OS 52%, DFS 62%, LC 54% | Decreased toxicity across decade treated due to advances in RT technique |
| Dirix et al, 2007 (Belgium) | 1976–2003 | 127 | 88 | 5-y OS 54%, DFS 37%, LC 53% | 15 patients with RT retinopathy, 2 patients with severe optic neuropathy |
| Bristol et al, 2007 (MDACC) | 1969–2002 | 146 | 100 | 5-y OS 55%, DFS 53%, LC 74% | 34% G3+ toxicity if treated before 1991 vs 8% if treated after 1991 |
| Mendenhall et al, 2009 (UF) | 1964–2005 | 109 | 49 | (Excluded maxillary tumors) 5-y OS 55%, LC 63% | 20% severe complications, including 19 patients with at least ipsilateral blindness |
| Duprez et al, 2012 (Belgium) | 1998–2009 | 130 | 78 | 5-y OS 52%, DFS 39%, LC 59% | G3+ ocular toxicity in 11 patients, but no blindness in patients who had IMRT |
| Al-Mamgani et al, 2012 (Netherlands) | 1999–2010 | 82 | 78 | 5-y OS 54%, DFS 56%, LC 74% | Decreased late toxicity and increased vision preservation with IMRT vs 3DCRT |
The combination of aggressive surgical resection and radiation therapy comes at the price of significant toxicity, particular to ocular structures and brain (eg, blindness, brain necrosis, cerebrospinal fluid leak, infection). Clinicians often face the decision of whether to sacrifice vision for cancer control, whether through orbital exenteration or radiation coverage. Conversely, surgeons may leave behind gross residual disease or positive margins adjacent to the orbit and base of skull, and radiation oncologists frequently reduce treatment volumes around these organs to prioritize sparing of vision.
Introduction
Sinonasal and ventral skull base malignancies are rare tumors; therefore, evidence for optimal management is limited primarily to single-institution retrospective series and population-based registry studies. Initial management is usually maximal surgical resection. Although no randomized trials exist, high rates of local failure have led to the wide adoption of postoperative radiation therapy for all except early-stage tumors without adverse pathologic risk factors. Numerous institutions published their experiences with this approach ( Table 1 ), with most reports spanning at least several decades and encompassing a mix of tumor stages and histologies. These series report 5-year overall survival (OS) rates of roughly 50% and local control (LC) of 50% to 70%. When patients present with unresectable disease or comorbidities precluding surgery, definitive radiotherapy or chemoradiation are used. In these cases, outcomes are suboptimal and toxicities significant as higher doses are needed to control gross disease. In select patients, a reassessment of resectability may occur after completion of definitive radiotherapy.
| Series | Years Treated | n | % Surgery | Results | Conclusions/Toxicity |
|---|---|---|---|---|---|
| Blanco et al, 2004 (WashU) | 1960–1998 | 106 | 65 | 5-y OS 27%, DFS 33%, LC 58% | Better outcomes in those who had surgery |
| Hoppe et al, 2007 (MSKCC) | 1987–2005 | 85 | 100 | 5-y OS 67%, DFS 55%, LC 62% | Only 1 G3+ ocular toxicity using mostly modern techniques (3DCRT, IMRT) |
| Dulguerov et al, 2001 (UCLA, Switzerland) | 1975–1994 | 220 | 71 | 5-y OS 40%, LC 57% | Better outcomes in those who had surgery |
| Chen et al, 2007 (UCSF) | 1960–2005 | 127 | 84 | 5-y OS 52%, DFS 62%, LC 54% | Decreased toxicity across decade treated due to advances in RT technique |
| Dirix et al, 2007 (Belgium) | 1976–2003 | 127 | 88 | 5-y OS 54%, DFS 37%, LC 53% | 15 patients with RT retinopathy, 2 patients with severe optic neuropathy |
| Bristol et al, 2007 (MDACC) | 1969–2002 | 146 | 100 | 5-y OS 55%, DFS 53%, LC 74% | 34% G3+ toxicity if treated before 1991 vs 8% if treated after 1991 |
| Mendenhall et al, 2009 (UF) | 1964–2005 | 109 | 49 | (Excluded maxillary tumors) 5-y OS 55%, LC 63% | 20% severe complications, including 19 patients with at least ipsilateral blindness |
| Duprez et al, 2012 (Belgium) | 1998–2009 | 130 | 78 | 5-y OS 52%, DFS 39%, LC 59% | G3+ ocular toxicity in 11 patients, but no blindness in patients who had IMRT |
| Al-Mamgani et al, 2012 (Netherlands) | 1999–2010 | 82 | 78 | 5-y OS 54%, DFS 56%, LC 74% | Decreased late toxicity and increased vision preservation with IMRT vs 3DCRT |
The combination of aggressive surgical resection and radiation therapy comes at the price of significant toxicity, particular to ocular structures and brain (eg, blindness, brain necrosis, cerebrospinal fluid leak, infection). Clinicians often face the decision of whether to sacrifice vision for cancer control, whether through orbital exenteration or radiation coverage. Conversely, surgeons may leave behind gross residual disease or positive margins adjacent to the orbit and base of skull, and radiation oncologists frequently reduce treatment volumes around these organs to prioritize sparing of vision.
Radiation therapy: indications and techniques
Postoperative radiation therapy is indicated when adverse features are found at the time of surgery. These include advanced T stage, high tumor grade or high-risk histology, perineural invasion, lymphovascular space invasion, positive lymph nodes, positive margins, and surgeon concern about the adequacy of resection or tumor spillage. One could consider radiation therapy for most patients, as margin status may always be considered close because of the “close quarters” and anatomic constraints in which these operations are performed and surgical techniques used, that is, piecemeal resection in a difficult anatomic area. Postoperative doses typically range from 50 to 66 Gy, but doses of 70 to 74.4 Gy or higher may be necessary to control gross residual or unresectable disease. Fraction size is usually 1.8 Gy or 2 Gy using once-daily fractionation or 1.2 Gy twice daily.
The necessity for high-dose for disease control and the sensitivity of adjacent structures presents challenges to the treating radiation oncologist. Advances in radiotherapy technique have altered the therapeutic ratio and allowed better coverage of tumors and increased sparing of these normal structures. Historically, sinonasal radiation was delivered using 2-dimensional portals using a 3-field technique drawn based on skull radiograph anatomy. Three-dimensional conformal radiotherapy (3DCRT) allowed planning based on computed tomography anatomy and led to improvements in target coverage and normal tissue sparing. In most modern centers, however, these techniques are no longer used for sinonasal and ventral skull base cancer.
Intensity-Modulated Radiation Therapy
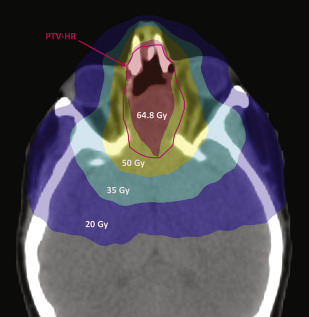
Intensity-modulated radiation therapy (IMRT) was one of the most important advances in modern radiotherapy planning and is the most common technique used for the treatment of sinonasal and ventral skull base malignancies in the United States. IMRT uses computational mathematics and inverse radiation planning combined with multiple beams of varying shapes and intensities to create an optimal radiation plan that conforms around irregular targets and avoids critical structures. Dosimetric studies have found that IMRT allows for better sparing of optic and brain structures and improved coverage of tumor. Fig. 1 shows an example of an IMRT plan.
Multiple studies report reduced toxicities with the use of IMRT compared with older techniques. Perhaps most striking are the studies that show reductions in toxicity across decades of treatment alongside advances in radiotherapy technique. Chen and colleagues reported the University of California, San Francisco experience over 5 decades and found a linear decrease in grade 3/4 late toxicities from 53% in the 1960s to 16% in the 2000s, with most of the latter patients treated with IMRT. Similarly, Dirix and colleagues compared patients treated with postoperative 3DCRT before 2003 versus postoperative IMRT after 2003 and found better disease-free survival and reduced cutaneous, salivary, and ocular toxicity in the patients treated with IMRT.
Charged Particles
Charged particle therapy using protons or carbon ions have garnered particular interest in the treatment of sinonasal and ventral skull base cancer. Charged particles are characterized by maximal dose deposition at an energy-specific depth (the “Bragg peak”) with minimal dose within the build-up and fall-off regions characteristic of photon beams ( Fig. 2 ). Therefore, charged particles have the potential to maintain target coverage and further lower dose to surrounding normal organs. Protons may be delivered via 2 techniques: passive scanning 3-dimensional conformal proton therapy and pencil beam scanning intensity-modulated proton therapy.
Dosimetric studies have found better normal tissue sparing with protons versus photon techniques. An example of proton versus IMRT dosimetry is shown in Fig. 3 . Mock and colleagues compared protons with conventional, 3-dimensional, and IMRT photon plans in 5 patients with paranasal sinus carcinoma. Protons reduced the mean dose to all normal structures compared with photon techniques, but the maximum dose to ipsilateral critical structures (adjacent to the postoperative bed) was not significantly different. Similarly, Lomax and colleagues and Chera and colleagues compared IMRT and photon plans in patients with paranasal sinus cancer. Protons and IMRT delivered similar maximum doses to adjacent critical structures, but protons were superior in lowering mean dose to more distant normal tissues. These findings suggest that charged particles may provide significant advantages over IMRT in reducing regions of low dose (eg, 20–50 Gy) but may not have the same perceived advantage for sparing brain and visual pathway structures adjacent to target. Thus, the long-term toxicities of vision loss and other central nervous system (CNS) toxicities may not be significantly reduced with protons compared with IMRT. In addition, sinonasal anatomy constitutes a mixture of air, fluid, and bone that may confound the robustness of proton radiotherapy plans, which are inherently more sensitive to daily changes in tissue heterogeneity. For example, a proton beam planned through a fluid-filled obstructed sinus may unintentionally overdose organs downstream of the target if that obstruction were relieved and that sinus filled with air.

Nonetheless, several centers report promising clinical results using charged particle therapy for sinonasal cancers. In addition, charged particle therapy has an established role in skull base chondrosarcoma and chordoma, which are discussed in further detail below. Of note, a large systematic review of single-institutional retrospective studies suggested that charged particle therapy improved survival and cancer control compared with photon therapy in patients with sinonasal tumors, although this analysis is limited by the heterogeneity of patients and inclusion of studies with older (2-dimensional, 3DCRT) radiation techniques in the photon group. Although data for charged particles are encouraging, the lack of widespread access and high cost associated with these facilities limits their routine use.
Stereotactic Body Radiation Therapy
Conceptually, stereotactic body radiation therapy (SBRT) and stereotactic radiosurgery are similar to IMRT but with sharper dose gradients and higher dose per fraction delivered in only 1 to 5 treatments. These highly conformal treatments historically were limited to specialized platforms such as Gamma Knife (Elekta, Stockholm, Sweden) and Cyberknife (Accuray, Sunnyvale, CA, USA), but modern linear accelerators are now capable of similar precision. The use of SBRT is not indicated in the primary treatment of most sinonasal and ventral skull base cancers because of the need to cover large elective regions and concern for excess late toxicity with higher dose per fraction, that is, hypofractionation. However, SBRT may have a role in the setting of reirradiation and for small ventral skull base tumors.
Reirradiation
Reirradiation for recurrent sinonasal tumors is not usually performed because of the potential for excessive ocular and neurologic toxicities along with poor prognosis; the chance for severe toxicity is often equivalent or even greater than the chance for cure. Nonetheless, there are reports on reirradiation with acceptable toxicity using modern techniques capable of maximal normal tissue sparing such as IMRT, SBRT, and charged particles.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


