The Pupil: Physiology and Function
Rockefeller S.L. Young
Kenn A. Freedman
Optical Aspects
The pupil, the aperture stop of the eye, is part of the optical system that includes the cornea, lens, and photoreceptors. Although not directly involved in forming the retinal image, the pupil contributes to its quality and intensity with minimal, if any, effect on the image size or its spatial location.
Contribution to retinal image
As the aperture stop of the eye, the pupil diameter determines the amount of light entering the eye.1 The illuminance of the retinal image is maximal when the pupil is large, and minimal when small. A change in pupil size from 8 to 2 mm reduces the image illuminance by about 16 times (1.2 log units), a darkening effect comparable to wearing a pair of dark sunglasses.
The size of the pupil also affects the quality of the retinal image through its influence on diffraction and aberration.2,3 Best spatial resolution of the image is generally achieved with a pupil diameter between about 2 mm and 3 mm.4 As the pupil becomes smaller or larger, resolution falls off. When smaller than 2 mm, the quality of the retinal image is degraded by diffraction. The pupil effect of diffraction on optical resolution is described by the Rayleigh criterion. The minimum resolvable separation θmin between two points of light varies inversely with the pupil diameter p,
θmin = 1.22 λ/p
where λ is the wavelength of the light. The minimum resolvable separation qmin becomes large with small pupils p. When the pupil becomes larger than 3 mm, the quality of the retinal image is degraded by optical aberrations.5
Effects on rods, cones, and vision
When light is focused on the retina, the pupil also serves as an aperture for each photoreceptor. The optical relationship between the pupil and the photoreceptors stems from the alignment of all rods and cones toward the pupil center (Fig. 9.1A). The pupil diameter limits the incidence angle and conical volume of light focused on the photoreceptors.
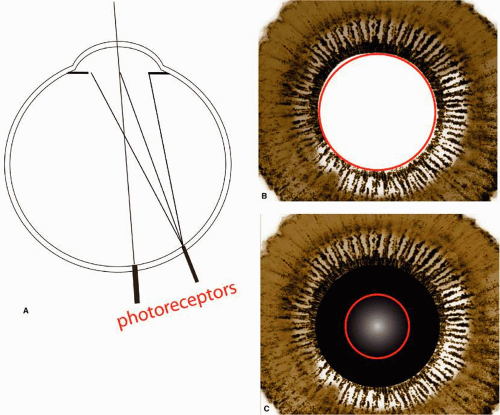 Figure 9.1 Relationship between entry of light rays through the pupil, incidence of light rays on photoreceptors, and effective pupil diameter for vision. A: Photoreceptors are generally oriented toward the center of the eye’s exit pupil (Enoch JM, Hope GM: An analysis of retinal receptor orientation 3. Results of initial psychophysical tests. Invest Ophthalmol 11(9):765–782, 1972). Pupil size limits the amount of focused light striking photoreceptors. B: Brightness of light passing through the pupil when viewed by rods. Light rays anywhere through the pupil have approximately equal effectiveness on rods (depicted as uniformly white). Thus, effective pupil diameter (red circle) is the same as actual pupil diameter. C: Light rays passing through the pupil center and edge differ in effectiveness on cone photoreceptors (Stiles-Crawford effect). Rays passing through the pupil center are generally seen as brighter. Effective pupil diameter for cone photoreceptors is illustrated by the bright area near the center of the pupil (red circle). |
The impact that the pupil has on vision varies, depending on whether vision is mediated by the rods or cones. The rod–cone difference arises from the variation in visual effectiveness of light rays entering the pupil at different points (i.e., the Stiles-Crawford effect of the first kind [SCE-1]).6 When vision is rod mediated, a ray of light passing near the center and another passing near the edge of a dilated pupil would appear equally bright (Fig. 9.1B). However, when vision is cone mediated, a ray passing through the center would appear brighter than one passing near the pupil edge (Fig. 9.1C). The relationship assumes that all light rays are focused on the photorecep–tors (Fig. 9.1A).When light rays are defocused, the relationship between the pupil entry and the effect on vision would be more complex. SCE-1 stems from the optical property of photoreceptors. Photoreceptors act as small optical fibers due to their cylindrical dimensions and higher refractive index than the surrounding tissue. Light entering along the fiber axis will be totally internally reflected, whereas light entering from oblique angles can escape into the surrounding tissue.7 Rods and cones differ in the acceptance angle of the incident light. Cones are more restrictive. Rods can capture light rays that are incident at about ±13 degrees from their axes.
Largely because of the SCE-1, dilating the pupil would have a greater effect on night vision than on day vision. The perception of spherical aberration in the eye’s optics is an example. Although the amount of optical aberration that can be physically measured increases as the pupil is widened, the subjective refraction increases with pupil size only when tested in dim illuminations that favor rod-mediated vision. When tested in daylight illumination, patients’ subjective refractive changes little, if any, with pupil diameter.8
Another way to describe this is in terms of the effective pupil size. The size of the pupil opening that affects vision is not always the same as the physical pupil size. When the pupil is dilated, the effective pupil diameter for the day vision would be smaller than the physical pupil diameter (compare ring diameters and pupils in Fig. 9.1B and C). This differs for night vision in which the effective pupil diameter would always be close to the physical pupil size.9
Benefits of a mobile pupil
The mobility of the pupil, although not essential, contributes to vision in a number of circumstances. In daylight, the pupillary constriction contributes to optimizing visual acuity over a wide range of luminances.10 Experiments show that the pupil size that gives the highest spatial resolution was also found to be the natural pupil size for the same luminance. Woodhouse11 extended the same finding over a wide range of contrast levels.
When a person’s pupil is immobile, the amount of visual loss experienced varies, depending on the pupil diameter and the illumination level. At dim illuminations, patients with a small fixed pupil would experience losses of spatial resolution up to 57% at low contrast. Patients with large fixed pupils would experience little or no loss. At high luminances, one would think that patients with a fixed 8-mm pupil might perform relatively poorly because of the optical aberrations inherent in the eye. However, at the highest luminance tested, losses of visual resolution were found to be small, reaching a maximum of 18.6% or a decrease of acuity from 20/20 to only 20/25.11
A mobile pupil contributes to the speed that the retina can adjust from a bright to a dim environment. If the pupils were fixed and dilated, high outdoor illumina–tions would substantially bleach the visual pigments in the photoreceptors and delay one’s ability to see in low illuminations such as in a darkened movie theater.12 However, with mobile pupils, the constriction in outdoor illumination reduces the strong bleaching effect and prepares “the eye in advance for the return to dim illumination.”13 Experiments show that when people come into a dark environment from bright outdoor illumination, the eyes with mobile pupils have an absolute threshold 10 times lower, and a contrast threshold 2.2 times lower than eyes with a fixed dilated pupil. This advantage persists for 4 to 10 minutes during the adjustment period in darkness.
Changes in pupil size have relatively little effect on the perception of the spherical aberrations in the eye’s optics.8 Changes in pupil size also produce little differences in the depth of field (depth of field is the dioptric range for which the retinal image quality does not change appreciably).14
Pupil size and terminologies
In clinical examination, one usually does not measure the physical pupil size (i.e., the optical opening formed by the iris muscles), but rather the entrance pupil (i.e., the pupil image formed by the anterior optics of the eye). Magnified by the cornea and aqueous in front, the entrance pupil is about 10% larger than the actual pupil diameter when estimated using subjective entoptic methods.15
The optical relationship between the physical pupil (PP) and the entrance pupil (EP) can be described as
PP = EP (1 – AK/n2)
where A is the anterior chamber depth in meters, K is the corneal curvature in diopters, and n2 is 1.3375, the index of refraction of the cornea.16 Accordingly, the size of the magnified image of the pupil should vary between 7% and 20% larger than the actual pupil, depending on values chosen for A and K. For example, in a typical eye that has an anterior chamber depth of 3.5 mm and a corneal curvature of 43 diopters, the entrance pupil would be magnified by 13%.
Estimating what a person’s pupil size is in everyday life is not a straightforward matter. The terms mydriasis and miosis refer to a generally large or small pupil, respectively. A person’s actual pupil size fluctuates over time. Even when observed under standard illumination conditions such as in a laboratory or clinic setting, the pupil size varies from moment to moment, depending on a person’s emotional state, wakefulness, and other factors. Terms such as pupillary unrest, pupil noise, and pupillary fatigue waves all refer to the fluctuation in pupil size, albeit, in the context of different situations. When the magnitude of the pupillary oscillations is marked, the term hippus is used. Loewenfeld15 defined hippus as “irregular, fairly large, seemingly spontaneous fluctuation in pupil size.” Pupil fluctuations occur throughout the day. However, they do not follow a circadian rhythm. The maximum pupil diameter appears to occur randomly.17
The pupil size varies from person to person.18 Studies of the dark-15 and light-adapted19 pupil diameters suggest that people’s age accounts for a substantial portion of the variability in the population. Beginning with a small pupil at birth, the pupil diameter increases reaching a peak around 12 to 18 years of age and thereafter declines steadily (0.4 mm per decade from ages 20 to 60 years). The pupil size under photopic illumina–tion decreases in almost a linear manner with increasing age.19 There appears to be little or no evidence that women or myopes have larger-than-normal pupils.19,20
The size of the left and right pupils in normal individuals is approximately equal. When there is a noticeable difference between eyes (i.e., a diameter difference of ≥0.4 mm) the condition is known as anisocoria.21 Anisocoria can be simple or physiological (i.e., occurring in otherwise healthy subjects), or it can be a sign of abnormal–ity. Simple anisocoria needs to be distinguished from pathological conditions such as Horner syndrome, Adie tonic pupil, and third nerve palsy (clinical correlates D and E).
The incidence of simple anisocoria depends in part on the illumination used to detect the condition. When tests are conducted in a dimly lit room, approximately 20% of healthy subjects are found to have anisocoria. When tests are conducted in ordinary room illumination, the prevalence drops to 8%.22
Pupil shape: actual and apparent
In humans, the normal pupil is round, and its edge is smooth. Deviations from roundness and smoothness can be caused by iris pathology such as congenital malformation, inflammatory diseases, trauma, atrophy or posterior synechiae, or destruction of part of the sympathetic or parasympathetic nerve fibers.23 The normal pupil, however, is neither perfectly circular nor concentric with the limbus (Fig. 9.2). The exact shape and location of the pupil vary between and within subjects. Although the deviations are not likely to be of great optical significance,24 the pupil variations in the normal population are important to know.
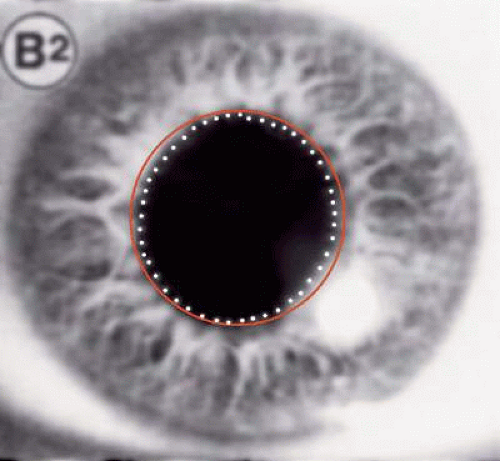 Figure 9.2 Pupil shape in normal eye. Shape of the pupil margin (white circle) is not truly circular, as can be more easily seen when compared to a geometric circle (red). The pupil center is also located slightly off the limbus center. Source: Photo of eye from Loewenfeld IE: The Pupil: Anatomy, Physiology, and Clinical Applications. Ames: Iowa State University Press, 1993:fig 9-10. |
The pupil shape generally tends to be elliptical in that there is usually a difference between the length of its major and minor axes.25 Mathematically, pupil noncircularity can be quantified in polar coordinates by Fourier harmonics above the second. Mathematical tests of the shape show noncircularity in all subjects tested.24
The pupil shape is not fixed. The shape varies a little as the iris contracts and relaxes. For example, the shape has been found to change with light levels (Fig. 9.3). In dim illumination that produces an average diameter of about 5 mm, the pupil tends to be slightly more elongated in the vertical orientation (i.e., about 0.3 mm longer).24,25 At higher light levels that produce an average diameter of about 3 mm, the pupil tends to be relatively more elongated in the horizontal orientation. The noncircularity increases with age,26 and the increase is about the same in the dark and in the light.24 There is also a tendency for mirror symmetry in the pupil shape between fellow eyes.24
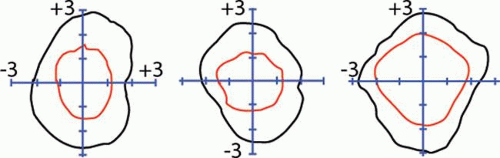 Figure 9.3 Pupil shape in light (red) and in darkness (black) for three subjects, one eye each. Pupils are shown as if viewed from the vitreous. All noncircularities were magnified by 5× for clarity. In general, light tends to contract the pupil near a vertical axis. Source: Adapted from Wyatt HJ: The form of the human pupil. Vis Res 35(14):2021–2036, 1995 |
The appearance of the pupil is also influenced by the angle that an examiner views the eye. When viewed at a substantial angle from the optic axis, the apparent pupil would have a pronounced elliptical like shape oriented vertically. Photographs and measurements have been published of pupils viewed at obliquities from 20 degrees nasal to 105 degrees temporal.27 In general, the horizontal diameter systematically decreases as the pupil is viewed at increasingly oblique angles.27 The shape and size projections at large angles of view are important aspects of the optics subserving peripheral vision.
Pupil centration and visual quality
The location of the pupil center is important to the quality of vision. The visual effects of decentered pupils have been studied experimentally by restrict–ing the light entering the eye with a small artificial pupil (or comparable method) and by systematically displacing the artificial pupil position. The visual effects of decentering include the loss of brightness,6 loss of contrast sensitivity or spatial resolution,10,28 changes in depth perception,29 and color distortion (i.e., the Stiles-Crawford effect of the second kind).30 SCE of the second kind refers to the change in color appearance as one changes the angle of incidence of a beam of light on the retina. In the laboratory, the effect is observed by displacing the point that the light rays enter the pupil.30a
Reductions in foveal spatial resolution caused by decentered pupils are associated with the transversed chromatic aberration rather than spherical aberration or coma.31,32 The cornea and lens, like other refractive material, exhibit chromatic dispersion. Obliquely incident rays will be spectrally dispersed because short wavelengths are refracted more than long wavelengths, producing a spatial smearing over one another due to transverse chromatic aberration. Thus, from this perspective, the ideal location of the pupil should be around the observer’s achromatic axis (Fig. 9.4), where light rays would be minimally refracted and thus minimally dispersed. In a sample of five subjects, the pupil center was found close to the ideal. The pupil center was on average 0.14 mm temporal to the visual axis and the angle ψ was only 2 degrees.33
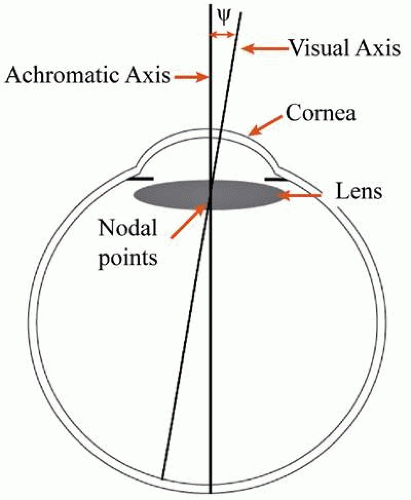 Figure 9.4 Schematic eye showing the optical surfaces and anatomical structures relevant to understanding importance of the pupil center. Achromatic axis follows path of chief nodal ray (passes through the center of the pupil and nodal points) and is the axis for which chromatic dispersion vanishes. Visual axis is the axis connecting fovea and fixation target via the eye’s nodal points. Optimal foveal resolution is expected when achromatic and visual axes are coincident (i.e., ψ = 0). Source: Adapted from Bradley A, Thibos LN: Modeling off-axis vision—I: The optical effects of decentering visual targets or the eye’s entrance pupil. In Pelli E (ed): Vision Models for Target Detection and Resolution. Singapore: World Scientific Press, 1995:313–337. |
Among clinical problems affecting pupil centration are wide arrays of disorders that displace the pupil or produce irregularities in the pupil margin. These distortions are broadly referred to as corectopia. Disorders that produce corectopia include ocular trauma, uveitis, and neurologic developmental and congenital disorders.
With the advent of refractive surgery, another consideration regarding centration has emerged (i.e., the centration of keratorefractive procedures over the pupil). Studies show that surgical errors can arise from incorrectly locating the center of the entrance pupil (Table 9.1).24,34,35 A common cause of this error is the shift in the pupil center as the iris contracts and dilates. Pharmacologically induced dilations appear to produce the largest shift in pupil center when dilated.36 Different types of mydriatic could also result in a different direction in the shift of the pupil center.37 Such decentration can produce postsurgical side effects that would appear to patients as star bursts, ghosting, halos, or double vision. These side effects are also referred to as high-order aberrations. Even with surgical methods that apply a spatially varying correction to the cornea (i.e., wavefront-guided surgery), postsurgical aberrations can still occur leading some investigators to hypothesize that the cause might be due to small errors in centration of the keratorefractive area.37
Table 9.1 Distance and direction in shift of pupil center (mean ± SD) | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
A proposed alternative to centering the keratorefractive procedure uses the corneal light reflex as a reference point. Studies by Nepomuceno et al.38 and Chan and Boxer Wachler39 reported on the centration of the LASIK ablation zone over the coaxial corneal light reflex for hyperopic patients. Their results suggest that the procedure could minimize unintentional decentra–tion of the ablation zone.
Pupillary light reflex
The pupillary light reflex (PLR) refers to the involuntary widening or narrowing of the pupil in response to changes of the retinal image. Constriction is the narrowing, whereas dilation is the widening.
When only one eye is stimulated, direct and indirect aspects of the reflex can be distinguished. The direct reflex refers to the pupillary reaction observed in the eye stimulated by light. The indirect, or more commonly, the consensual reflex refers to the reaction observed in the unstimulated eye.
The pupil constricts more when both (rather than one) eyes are stimulated. This is referred to as binocular summation. The effect of both eyes is roughly the same as stimulating one eye over twice the retinal area.40 An alternative method of demonstrat–ing binocular summation is to cover one eye of a subject who has been seated in a lighted room. With normal subjects, covering one of the two eyes removes the binocular summation and causes both pupils to widen.
Failures of the pupil to respond to light provide objective evidence of an abnormality. The finding of a poor pupillary reaction can be attributed to either extremes of the reflex pathway. Possible sites of defect in the afferent limb include the retina, optic nerve, chiasm, or optic tract. The swinging flashlight test is probably the simplest of clinical tests developed to evaluate afferent defects (clinical correlate A).
Possible sites of defect in the efferent limb include the third cranial nerve, ciliary ganglion, posterior ciliary nerves, and the iris dilator and sphincter muscles. When the efferent pathway is affected, a poor or absent pupillary light reaction is usually associated with miotic (constricted) or mydriatic (dilated) pupils. If the efferent limb is affected in only one of the two pupils, then a difference in pupil size between eyes appears (i.e., anisocoria). If a pupil is totally nonreactive to light or darkness, the pupil is referred to as fixed. The condition when the pupil is nonreactive to light but constricts to a near target is called light-near dissociation (clinical correlate C).
Pupillary reaction to features of the retinal image
Features of the retinal image that elicit the PLR are generally similar to the features that are perceptually salient. This is perhaps not surprising because both the pupil and perception depend on information processed through the retina and optic nerve. However, in comparison to perceptual processes that tend to discount the illuminance (i.e., make objects look the same even when viewed under different illuminances), the image illuminance is among the strongest determinants of pupil diameter. The relationship between pupil diameter and illumination levels is described by an “S-shape” function in which the steady-state pupil diameter becomes smaller as the illumination level is raised.
The amplitude of the luminance-evoked reflex correlates with perceptual visual losses in a number of clinical conditions. In patients with optic nerve disorders, the amplitude of the luminance-evoked PLR correlates highly with losses in the visual field. Pupil amplitude, however, only weakly correlates with visual acuity losses.41 When a fully dark-adapted eye is stimulated by full-field illumination, the amplitude of the pupillary contractions is determined to a large extent by rods.42,43 This has led several investigators to use the PLR as a correlate of night blindness in adults44 and in children.45
Stimulating the eye with incremental or decremental luminance steps illustrates several notable features about the temporal waveform of the pupillary reaction (Fig. 9.5, top). When moderately bright lights are used, the pupil typically constricts following the luminance onset and dilates following its offset. When a luminance increment is presented for a long duration, the initial pupillary constriction is often followed by dilation even while the light is still on. This dilation is referred to as pupillary escape. (The term should not be confused with the dilation of both pupils when a light is moved from the nonaffected eye to the affected eye during a swing flashlight test.)45a When the luminance is low (e.g., near perceptual threshold), the recordings expose another kind of pupillary dilation (i.e., TRPR in Fig. 9.5, top). Because the dilation typically occurs prior to the light onset, it cannot be attributed to the stimulus per se. Rather, the dilation is believed to be a reaction produced by the mental preparation or the execution of some task that the subject was required to perform.46
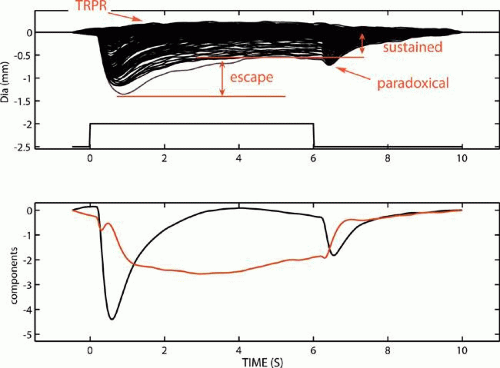 Figure 9.5 Pupillary light reflex to a chromatic flash against white background. Top: Time-averaged waveforms evoked by series of flash intensities. Waveforms for various intensities illustrate pupillary escape and paradoxical pupil. Waveforms for lowest intensity show dilation reflex associated with a task the observer was instructed to undertake. These dilations are called task-related pupillary responses. Bottom: Some scientists hypothesize that the pupillary light reflex waveform is composed of components with transient (black) and sustained (red) temporal characteristics, perhaps relating to the discharge characteristics of the underlying neurons. Source: Data from Kimura E, Young RSL: Nature of the pupillary responses evoked by chromatic flashes on a white background. Vision Res 35(7):897–906, 1995. |
The term paradoxical is used to describe instances where the direction of pupillary response is unexpected. Paradoxical constriction is commonly used in the ophthalmic literature to refer to the pupil contraction observed following the offset of light. Paradoxical constriction has been observed in patients with congenital stationary nightblindness,47 congenital achromatopsia,48 blue-cone monochromatism,49 dominant optic atrophy, bilateral optic neuritis, and other disorders. Although questions about why patients with different disorders all exhibit similar paradoxical constrictions have largely remained unanswered, it might be important to mention that similar paradoxical reactions occur in normal subjects (Fig. 9.5). The appearance of the paradoxical constriction depends in part on the previous light intensity. The constriction becomes less obvious after a bright light exposure (Fig. 9.5, top).47 Statistical analyses of the components common to the intensity series of waveforms suggest that the constriction following the light offset is a transient reaction. This constriction might not be as obvious at high light levels because the sustained pupillary component tends to mask its appearance (Fig. 9.5, bottom).
The prominence of the pupillary escape and sustained contraction in the PLR depends in part on the location of the retina stimulated. Neurons mediating the central retinal field apparently contribute greater to the sustained constriction than neurons in the peripheral retina. So, when patients lose central visual field, their PLR tends to exhibit smaller sustained constrictions and more obvious pupillary escape.50
Luminance increments and decrements are not the only features of the retinal image that elicit a pupillary reaction. The pupil also reacts to the change in the spatial dimension and contrast of the image contours.51,52,53,54,55,56,57,58 The pupil constricts when an observer views a change from a spatially homogenous field to that of a spatial grating with identical space-averaged luminance. The magnitude of the PLR evoked by such image features is relatively small in comparison to the luminance-evoked effects. But the PLR can be assessed reliably by magnifying the pupil image and using signal enhancing methods to estimate the evoked changes in pupil diameter.
By examining the change in contraction amplitude to progressively finer gratings, previous investigators estimated the minimal grating width required to evoke a just-detectable response. Such spatial thresholds provide a pupillometric correlate of the perceptual spatial acuity. Under photopic illumination, the pupillometric acuity was found to be 20/20.51 Under scotopic illumination, the pupillometric acuity was similar to that for night perception (i.e., about three cycles per degree).56 Photopic pupillometric spatial acuities can be assessed in both infants and adult subjects. The spatial acuity is determinable in those older than 1 month.57,58
The shape of the temporal waveform changes when evoked by spatially fine in comparison to spatially coarse patterns.53,55 When a fine pattern was displayed for 6 seconds, the pupil constricted and maintained a small diameter over the duration of the display. Following the offset, the pupil redilated to its original diameter. When a coarse pattern is displayed for the same duration, the pupil constricted transiently following the pattern onset and again following the pattern offset. Significant temporal differences between patients with glaucoma and healthy control subjects were recently reported.59
The temporal change in image color also produces a transient constriction.60,61,62,63 Studies ruled out the trivial possibilities that the pupillary constriction is produced by unintentional changes in luminance or to spatial changes produced by chromatic dispersion.62,64,65 The chromatic reaction probably originates from visual signals downstream of the photoreceptors that differentiate the wavelength from the intensity aspects of the light. Using experimental paradigms similar to those used in psychophysical color vision studies, investigators found that the pupillary action spectrum for chromatic flashes on a bright white background was similar to that derived by perceptual threshold criteria.66,67 Specifically, the transient responses following the onset and offset of the chromatic flash exhibited a “Sloan notch” in the action spectra, suggesting a subtractive L- and M-cone interaction. The sustained portion of the pupil response exhibited a different spectral property. These findings imply that the PLR has at least two functionally distinct components. Investigators showed that the effects on the pupil to reddish lights can be reduced, if not nulled, by adding green.68 Such property is analogous to perceptual red-green (hue) cancellation. Investigators also showed that subtractive interactions mediated by L- and M-cones were complemented by subtractive interactions between the S- and the longer wavelength sensitivity cones.69,70 In brief, the available evidence suggests that the pupillary responses to color changes are mediated by opponent cone interactions not dissimilar to those mediating perceptual color thresholds. Tsujimura et al.63 however offered a different theoretic framework for understanding this effect. Instead of attributing the pupillary reaction to the change in image color, they hypothesized that the response was caused by the appearance of afterimages following the color change. The investigators provided evidence that the pathway underlying the offset response has properties similar to the magnocellular pathway.63 However, more insights regarding the retinal substrate underlying the chromatic responses await the results of studies concerned with giant retinal ganglion cells that project to the pretectum and have known color opponency.
The transient pupillary constriction to color changes can be used to discriminate protans and deutans from color normals.71 Although such a test is not likely to replace the traditional color tests in the clinic, the pupillometric test provides an alternative that would be suitable for evaluating nonverbal subjects.
The pupillary responses to spatial gratings or to the temporal exchange of chromatic lights can also be recorded in monkeys.72 However, although the responses were qualitatively similar to those observed in humans, the pupil response latencies were some 80 to 100 milliseconds shorter, and the pupil showed a more rapid recovery from constriction.
The effect of image motion was studied the least. Barbur, Harlow, and Sahraie,73 however, developed the basic paradigm for study, whereby observers first viewed a dynamic display of dots randomly displaced over time. Then motion was introduced by displacing all of the dots in the same direction. Such paradigm creates image motion without introducing global changes in the light flux on the retina. Image motion produced a pupillary constriction.
In summary, studies from several laboratories have independently established that the pupil light reflex does not only respond to the luminance of the retinal image, but also responds to features related to the spatial frequency composition, chromaticity, and motion of an image. Such findings suggest that the scope of clinical pupil evaluations could be expanded.
Current views regarding the temporal shape of the pupillary waveform
The temporal shape of the PLR waveform was believed to reflect two underlying processes: one that transformed visual images into unidirectional rate sensitive and the other into bidirectional proportional response components.60,73 The observed pupillary response waveform was the sum of the outputs from the two processes. The unidirectional component corresponded with the observed transient constrictions produced when, for example, a red light is temporally exchanged with a green light of the same brightness. The exchange from red to green or green to red both produced the same direction of response (i.e., constrictions). The bidirectional component corresponded with the sustained aspects of the pupillary reaction, such as the pupillary constriction produced by the presence of light and dilation produced by the absence of light.
More recent investigators suggested the similarities between the uni- and bidirectionality in the pupillary reactions with the transient-sustained aspects of perception and the phasic-tonic electrophysiological characteristics of M- and P-pathways.55,62,64 However, although parallels could be drawn, the properties of the pupillomotor system were also different. Whereas perceptual color information is conveyed by a temporally sustained pathway, the pupillary reaction to color changes is temporally transient in character. Conversely, whereas perceptually achromatic processes are believed to be transient (phasic) in character, the pupillary reactions to luminance steps are sustained. The physiological basis for the similarity and differences remains unknown.
Variability in magnitude
The variability in the magnitude of the luminance-evoked PLR is noteworthy. Between-subject variability is important because it reflects how well abnormal responses would be distinguished from normal population values. Within-subject variability (i.e., repeated measures or between eye measurements) provides information about the reliability of an observed effect or the significance of an observed change in a patient’s performance. In general, within-subject variability in the PLR is usually much smaller than between-subject variability.
Individual differences in the constriction versus illumination relationship have been reviewed previously.18,74 As with estimates of the pupil diameter at rest, the variability in the contractions evoked by luminance is in large part accounted for by age. At the earliest extreme of life, very premature infants have large pupils that do not exhibit a reflex constriction to light.74a The pupil decreases in diameter from week 26 to week 29 of gestation. A response to light is not found before about week 30 of gestational age. Factors influencing the development of the PLR in infants include the immaturity of the autonomic pupil innervation, photoreceptors, and iris muscles.74a The maturation of the iris sphincter muscle is delayed relative to the dilator.
Between-subject variability is partly attributed to the mechanical property of individual irises. According to Loewenfeld,15 “all other features being equal, smaller pupils have more difficulty than large pupils in constricting under the influence of light or other stimuli.” Consequently, the amplitude of the PLR depends on the initial size of the pupil.15 The mechanical properties of the iris are also believed to account for differences in the PLR observed with different flash durations. The age dependency is strongest when the reflex is evoked by intense 3-second lights. When evoked by weaker 1-second lights, the amplitude of the reflex is more constant with age until well into the seventh decade, consistent with the fact that the reflex to weak lights requires less mechanical range of the iris.
Intraocular differences have also been studied. Comparisons of pupillometric field sensitivities, for example, showed similar shape and heights in the hill of vision between eyes of the same observer (i.e., r = 0.83). The similarity between eyes is about the same as that found when visual fields are assessed by perceptual criteria (i.e., r = 0.79).75 The pupillometric field sensitivities, however, only account for about l9% (r2) of the total variance observed in the perceptual visual field measurements. Differences between the pupillometric and perceptual assessments were attributed to the kinds, the number, and the receptive field properties of retinal ganglion cells underlying the pupillomotor as compared to perceptual responses.
Because between-subject variability is generally much larger than within-subject (between eye) variabil–ity, clinical tests have focused on evaluations of relative afferent pupillary defects (RAPD). For example, the swinging flashlight test is performed by comparing the pupillary reactions to light shone alternately in a patient’s left and right eyes (clinical correlate A). The relative afferent test is sensitive when the problem is uniocular. However, the relative test is insensitive to problems involving both eyes to similar degrees. In addition, some normal subjects may show a persistent but small RAPD in the absence of detectable pathological disease.76 So, a RAPD abnormality must be assessed relative to the degree of asymmetry present in the normal population.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


