The Nasal Dorsum: Management of the Upper Two-Thirds of the Nose
Randolph B. Capone
Ira D. Papel
Of all the aesthetic facial units, the nose plays a predominant role in facial proportion and harmony. As a single unpaired structure occupying the midface, it serves to balance the facial thirds and fifths as well as those aesthetic units surrounding it. Seemingly small changes after rhinoplasty or traumatic injury frequently effect dramatic changes in nasal appearance. The nose is not, however, only an aesthetic structure but also a respiratory and olfactory organ. This duality of nasal form and function mandates that rhinoplasty must enhance nasal appearance and optimize the nasal airway. It is essential, therefore, that the nasal surgeon have a detailed understanding of nasal anatomy and physiology and a thorough grasp of the many interventions available in rhinoplasty. In this chapter, we discuss these issues with regard to management of the upper two-thirds of the nose, that is, the bony and cartilaginous vaults.
ANATOMY
The upper two-thirds of the nose contains the dorsum and sidewall aesthetic subunits, whereas the tip, columella, soft tissue triangles, and alae constitute the lower third of the nose (Fig. 181.1) (1). Topographically, the upper twothirds of the nose is that portion from the nasion to the level of the alar groove (Fig. 181.2), where the nasion is defined as the intersection of the internasal suture with the nasofrontal suture in the midsagittal plane. The radix is the root of the nose and defines the most posterior point along the curve from the glabella to the nasal dorsum.
Skin and Subcutaneous Tissue
The skin overlying the upper nasal two-thirds has variable thickness. Relatively thick at the nasion (2 to 5 mm), it becomes thin and mobile over the dorsum (3.2 mm) and thinnest at the rhinion (2 to 2.2 mm) and gradually thickens again, becoming sebaceous toward the tip (5 mm) (2). This variability is important in planning the dorsal profile because creation of a straight skeletal profile will not likely create a straight postoperative profile. When edema diminishes, the surgeon may find that the rhinion has been overresected if no allowance for skin thickness was considered during surgery.
Beneath the skin is a thin fibrous layer designated the nasal superficial musculoaponeurotic system (SMAS) (3). Analogous to the facial SMAS, the nasal SMAS encompasses the nasal musculature and is located immediately superficial to the periosteum and perichondrium. Dissection just below the nasal SMAS provides a less traumatic and easier dissection plane during rhinoplasty, with preservation of nasal vasculature, nerves, and lymphatics that lie within the skin-soft tissue envelope (4).
Nasal Bones and Upper Lateral Cartilages
Deep to the nasal SMAS are the paired nasal bones and upper lateral cartilages. The nasal bones fuse with the frontal bone approximately 11 mm superior to the intercanthal line and are on average 2.5 cm in length (5). The length can be quite variable and represents a significant risk factor for airway compromise after rhinoplasty, for the shorter the nasal bones, the greater the proportion of cartilaginous nasal anatomy that is cantilevered and supported (6). The caudal margin of the nasal bones overlaps the cephalic margin of the upper lateral cartilages, which in turn interlock with the paired lower lateral cartilages at the scroll (Fig. 181.3). Each of these connections is an important structural component that contributes to nasal integrity and support.
Laterally, the caudal margin of the nasal bones and the anterior margin of the ascending processes of the maxilla form the piriform aperture. The lateral margin of the upper lateral cartilages fuses with dense connective tissue, and the
medial margin fuses with the septum superiorly but separates and is mobile inferiorly. Mucosa is tightly adherent to the internal surface of the cartilages and is continuous with the lining of the septum and lateral nasal wall.
medial margin fuses with the septum superiorly but separates and is mobile inferiorly. Mucosa is tightly adherent to the internal surface of the cartilages and is continuous with the lining of the septum and lateral nasal wall.
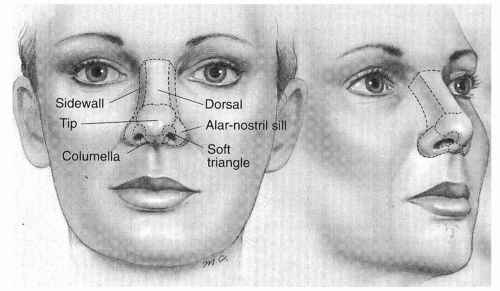 Figure 181.1 Nasal aesthetic subunits. (From Burget GC, Menick FJ. Aesthetic reconstruction of the nose. St. Louis, MO: Mosby, 1994:7, with permission.) |
The caudal margin of the upper lateral cartilage, the anterior head of the inferior turbinate, the proximate septum, and floor of the nose define the borders of the internal nasal valve. The angle between the upper lateral cartilages and the septum is the nasal valve angle, normally 10 to 20 degrees. The internal nasal valve typically has a crosssectional area of 55 to 83 mm2 and represents the site of greatest nasal resistance. It is the primary airflow-limiting segment of the nasal cavity in the human nose (7).
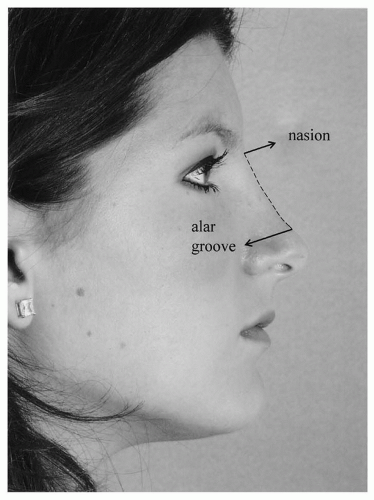 Figure 181.2 Upper nasal two-thirds: nasion to alar groove. |
The Bony and Cartilaginous Vaults
The upper nasal two-thirds can be thought of as two contiguous arches, or vaults—a superior bony vault and an inferior cartilaginous vault. The nasal bones and the paired ascending processes of the maxilla comprise the bony vault, and the cartilaginous vault is composed of the upper lateral cartilages and the cartilaginous dorsal septum. The region of transition of the bony vault to the cartilaginous vault is known as the rhinion. The soft tissue linkage that occurs at the rhinion is comprised of upper lateral cartilage perichondrium that inserts on the undersurface of the paired nasal bones. This union allows for motion of the inferior vault relative to the superior vault.
As the name implies, nasal vaults are critical for support, distribution of forces, maintenance of dorsal height, and maintenance of nasal projection. As with any arch, the most essential support element occurs at the keystone. The nasal keystone area is the convergence of the caudal margin of the nasal bones, the perpendicular plate of the ethmoid bone, the cephalic margin of the upper lateral cartilages, and the cartilaginous septum. Understanding this area is critical during planning and execution of osteotomies so as to effect a change without disruption of important support mechanisms.
NASAL ANALYSIS
The face is a complex set of surfaces with tremendous variability. The goal of facial analysis is to provide a consistent framework to compare pre- and postoperative results despite this variability. Nowhere is this more important
than in rhinoplasty. Every rhinoplasty candidate should have high-quality six-view photography to facilitate analysis. In addition, an additional chin-down view is especially useful in evaluation of patients with nasal vault deformity (Fig. 181.4).
than in rhinoplasty. Every rhinoplasty candidate should have high-quality six-view photography to facilitate analysis. In addition, an additional chin-down view is especially useful in evaluation of patients with nasal vault deformity (Fig. 181.4).
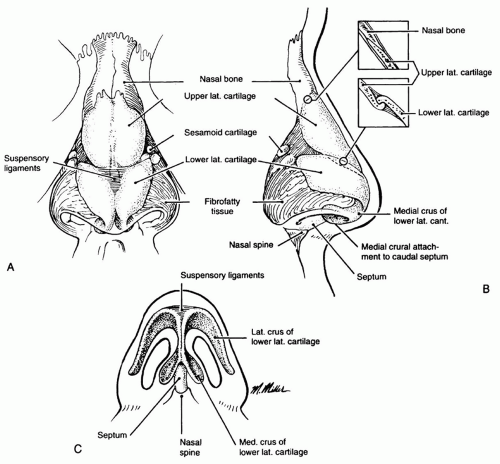 Figure 181.3 Anatomic relationships of the nasal bones, upper lateral cartilages, and lower lateral cartilages. (Modified from Papel ID. Management of the middle vault. In: Papel ID, ed. Facial plastic and reconstructive surgery, 2nd ed. Stuttgart, Germany: Thieme, 2002:408, with permission.) |
Aesthetic Angles
Analysis of the nasal aesthetic angles reveals the importance of the dorsum in evaluation of the rhinoplasty patient. Of the five facial aesthetic angles, three are determined using the geometry of the nasal dorsum: the nasofacial, the nasofrontal, and the nasomental angles. The nasofacial angle is the angle prescribed by the intersection of the facial plane (glabella to pogonion) and a line tangent to the nasal dorsum. Ideally, it is 36 to 40 degrees. The nasofrontal angle is determined by the intersection of the line connecting the nasion and glabella and the nasal dorsum tangent, ideally 115 to 130 degrees. Lastly, the nasomental angle is determined by the intersection of the line connecting the tip-defining point to the pogonion and the nasal dorsum tangent. The ideal nasomental angle is 120 to 132 degrees. Each of these angles should be carefully considered during the examination and photographic evaluation of the rhinoplasty candidate.
Nasal Length
Leonardo da Vinci introduced the practice of dividing the face into equal vertical thirds and horizontal fifths for the purpose of facial analysis. Later modified by Powell and Humphreys (8), this serves as the basis for modern-day facial analysis. A method more specific to nasal analysis, however, divides the lower face into two parts using the nasion, subnasale, and menton as landmarks (9). Using this method, nasal length (nasion to subnasale) should be three-fourths the distance from the subnasale to the menton (Fig. 181.5).
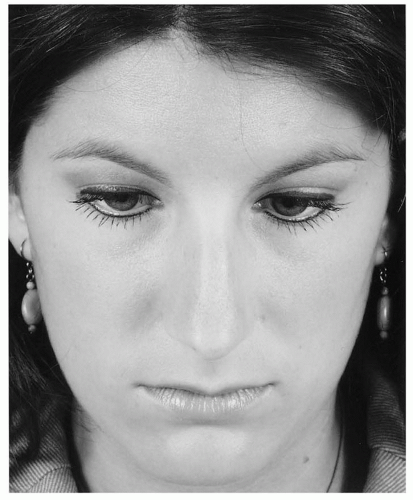 Figure 181.4 The chin-down view of nasal dorsum is useful to detect the presence of subtle radix contour irregularities or asymmetry. |
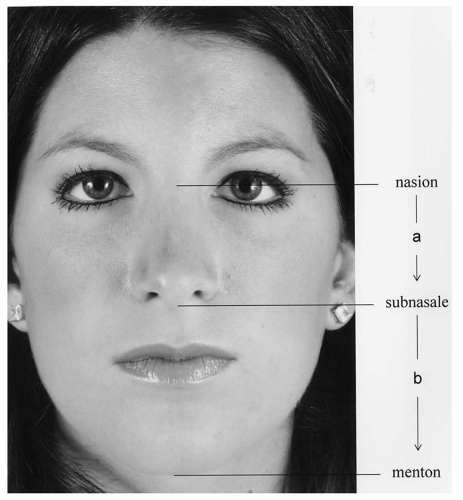 Figure 181.5 Determination of nasal length using the nasion, subnasale, and menton: ideally a = ¾ b. |
Nasal Width and Radix Contours
On frontal view, nasal width should increase along its length, with a minima occurring at the intercanthal line. Maximal nasal width occurs at the alae and should equal one-fifth the width of the face. The upper nasal contour should follow a gentle curve from the medial eyebrow to the ipsilateral tip-defining point. Any irregularities in this brow-tip aesthetic line will quickly be noted as different from the contralateral side, thereby contributing to asymmetry and an unsightly appearance. The pair of these lines (also referred to as radix contours) is highlighted by the nasal light reflex and are ideally symmetric (Fig. 181.6).
Dorsal Projection
The nose projects anteriorly from the face, with its forward thrust orthogonal to the facial plane and parallel to the midsagittal plane. Quantification of nasal projection is a critical component of the rhinoplastic evaluation, yet of the many methods previously described, none specifically address dorsal projection (i.e., dorsal height) (10, 11, 12). Determination of proper tip projection using Crumley’s method, however, utilizes the geometry of the 3:4:5 triangle; that is, projection of the nasal tip should equal three-fifths (0.6) the length from the nasion to the tip-defining point. This method can be used simultaneously to yield the ideal dorsal projection at any point along the dorsum,
because the proportions of a 3:4:5 triangle are constant (Fig. 181.7). If dorsal projection exceeds this limit (0.6), it is indicative of the presence of a dorsal hump. Because a slight dorsal concavity can be attractive, dorsal projection just less than this limit is allowable, but a significantly lower measurement could be indicative of a saddle-nose deformity.
because the proportions of a 3:4:5 triangle are constant (Fig. 181.7). If dorsal projection exceeds this limit (0.6), it is indicative of the presence of a dorsal hump. Because a slight dorsal concavity can be attractive, dorsal projection just less than this limit is allowable, but a significantly lower measurement could be indicative of a saddle-nose deformity.
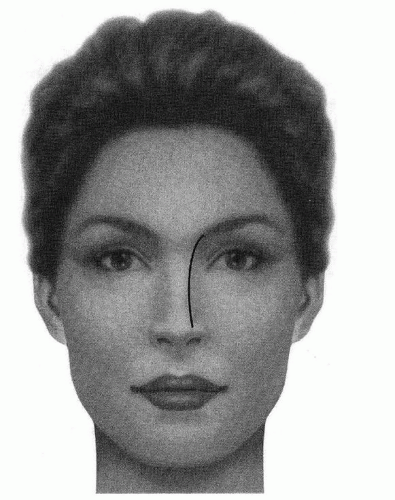 Figure 181.6 Brow-tip aesthetic line. (From Orten SS, Hilger PA. Facial analysis of the rhinoplasty patient. In: Papel ID, ed. Facial plastic and reconstructive surgery, 2nd ed. Stuttgart, Germany: Thieme, 2002:361, with permission.) |
DEFECTS OF THE NASAL VAULTS
Bony Vault Defects
Most deformities involving the bony vault arise from blunt trauma (Table 181.1). Fractured nasal bones can be comminuted and/or displaced, often resulting in an unsightly twist, depression, spur, or hump. Frequently, the skin overlying the bony dorsum is lacerated causing additional deformity by the presence of cicatrix and adherence of the dermis to the nasal bone periosteum. Severe fractures such as nasoorbital ethmoid (NOE) fractures are often quite disfiguring due to retrodisplacement of the nasal bones, deprojection and flattening of the nasal dorsum, and shortening of the nose. The resultant telescopic defect is often associated with traumatic telecanthus due to the disruption of the medial canthal tendon insertion on the nasal bones. Trauma involving the bony vault will commonly contribute to functional deficits if the keystone area, the septum, or the middle vault is also affected. Less common causes of upper vault deformity include prior rhinoplasty, neoplasia, and congenital anomalies (13, 14).
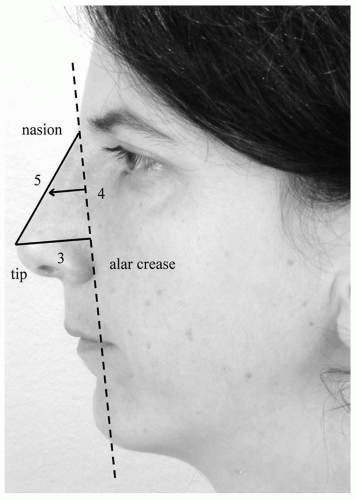 Figure 181.7 Determination of ideal dorsal projection using Crumley’s tip projection analysis. At any point along the dorsum, the ratio of dorsal projection to the distance from the nasion should equal 3/5 (0.6). |
Cartilaginous Vault Defects
Deformity of the middle nasal vault can be more complex than that of the bony vault because it is frequently accompanied by internal nasal deformity contributing to airway compromise. The internal nasal valve occurs near the junction of the upper lateral cartilages and the dorsal septum and is often weakened or narrowed subsequent to




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
