The Lower Eyelid and Beyond
The earlier edition treated the eyelids together, but here the dissections go beyond that to expose those structures in separate zones. This chapter exposes the lower eyelid inferolateral zone.
These studies extend downward to expose the suborbicularis oculi fat (SOOF), orbital retaining ligaments (ORL), and the zygomatic/elevator muscles. Ligaments and nerves are emphasized, key for performing subsuperficial musculo-aponeurotic system dissections. The dissection continues laterally and upward to expose the fascia below the lateral orbicularis muscles. This lateral orbital thickening (LOT), is triangular with the apex laterally placed. The size of this fascial area decreases with age.
Inferior and Lateral to the Orbital Rim
1 The orbicularis oculi attaches directly to the inferior orbital rim from the anterior lacrimal crest to the medial limbus of the cornea. Thus, to approach the medial SOOF, you must transect this muscle at the bony rim. As the patient ages, some of the more lateral muscle attachment may pull away from the rim as the check droops.
1a If you continue dissection medially through the orbicularis oculi, the next key structure you would approach is the levator labii superioris alaeque nasi, under which resides the infraorbital foramen with its nerve and vessels.
2 Laterally, the orbital septum attaches along the rim and a little beyond, but the orbicularis muscle attaches to the rim indirectly here via multiple ligaments. Thus, to expose the SOOF, here these ligaments (ORL) need to be transected. These are the orbital retaining ligaments (ORL).
3 These retaining ligaments, which go from the periosteum to the suborbicularis fascia, continue laterally and upward to the lateral orbital rim.
3a The zygomaticofacial nerves exit the bone inferior to these ligaments to supply sensation over the cheek prominence and inferiorly. The sensory area can be represented by an inverted triangle with the apex downward.
3b These ORLs continue around and upward in continuity with the suborbicularis fascia below the orbicularis muscle laterally. The “lateral orbital thickening” as noted LOT varies in size; older bodies seem to have less.
3c If the ORLs are released below the inferior orbital rim and laterally (i.e., the LOT as well), the orbicularis connections with the lower lid to bone will be severed, and this will allow movement of the entire lid. Thus, redraping of the pretarsal and preseptal orbicularis would require release of the ligaments. With medial release of rim attachments the orbicularis oculi can be fully redraped if necessary.
4 A thick, subcutaneous malar fat pad overlies the cheek bone from the rim downward. The fat pad covers the lower orbital fibers of the orbicularis oculi, which extend considerably over the cheek. Fibers are interspersed with fat.
5 If by dissection the orbicularis oculi muscle and fascia are elevated from below after malar fat pad is swept down, these orbital retaining ligaments can be approached from below. This area up to the ligaments has been dubbed the “prezygomatic space.”
6 By elevating the lower orbicularis muscle and fascia upward, the zygomaticus major muscle fibers become exposed. The lateral zygomaticus fibers begin on a plumb line dropped down a little laterally to the lateral part of the lateral orbital rim. (Remember this!)
7 The zygomatic branch of cranial nerve VII innervates the zygomaticus muscles and continues onward to innervate the lower orbicularis oculi, levator muscles, and even the upper lid depressor supercilii and medial orbicularis oculi (and perhaps the procerus).
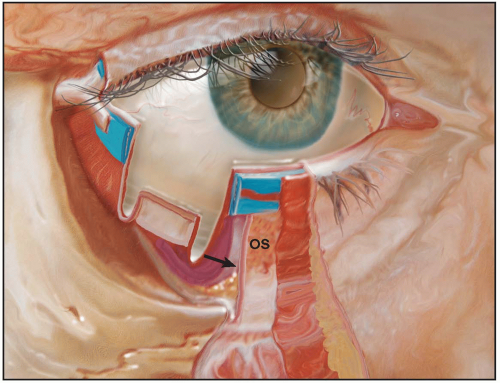 Figure 3.1 The anterior lamella of the lower lid consists of skin and underlying muscle. Note the cut edge of the orbital septum (OS), which meets at the junction of periosteum and periorbita, the arcus marginalis (lower arrow). The upper arrow denotes the capsulopalpebral fascia, an extension of the inferior rectus muscle that acts to lower the eyelid in unison with the globe during downward gaze. |
 Figure 3.2 The skin and malar fat pad of the lower eyelid are retracted inferiorly, exposing the orbicularis oculi muscle. Note the horizontal orientation of the blood supply in the upper portion of the muscle. These represent branches of the inferior medial and lateral palpebral branches derived from the infratrochlear and lacrimal arteries, respectively. The arterial supply courses in a submuscular plane and receives anastomosing twigs from the angular, infraorbital, transverse facial, and zygomaticofacial vessels. Note that the orbicularis oculi muscle originates from the medial canthal tendon (T) and from the lower medial orbital margin. The orbicularis fibers sweep temporally, covering the origins of the elevators of the upper lip and nasal ala. They extend across the cheek to overlie the anterior part of the temporalis fascia. The upper orbicularis is supplied by the temporal branch of cranial nerve VII with some small twigs off the zygomatic branch. Lymphatic drainage from the lateral side is into the preauricular and parotid nodes. The medial side drains into the submandibular regional nodes. |
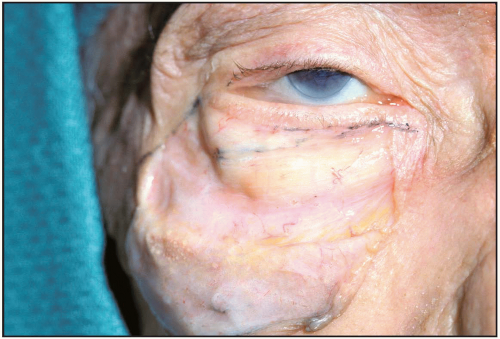 Figure 3.3 Muscle thickness varies from person to person. In this dissection, the orbital septum and fat are visible in spite of “skin-only” removal. The muscle, therefore, is quite thin, easily explaining how scant muscle, bony hypoplasia (“negative vector”), and thin septum would predispose to bulging fat, as well as a possible ptotic lid. |
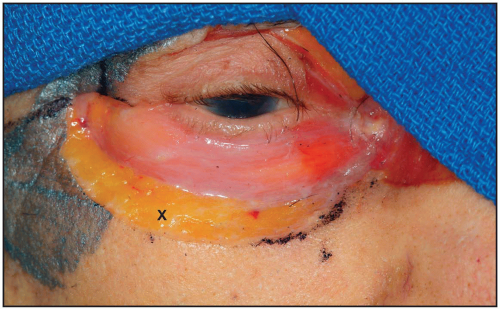 Figure 3.4 In this younger specimen, the orbicularis muscle (pretarsal and preseptal portions) covers the orbital septum evenly. Note the thick malar fat pad (X) under the cheek skin. |
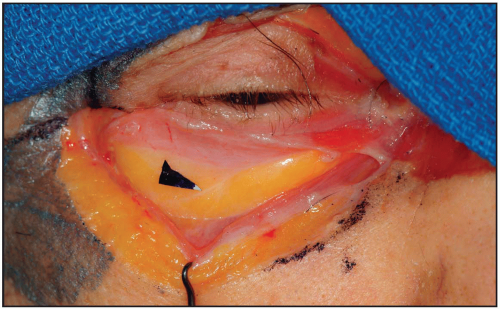 Figure 3.5
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|