FIGURE 24.1 Osteocutaneous radial forearm free flap.

FIGURE 24.2 Diagram noting the extent of radial bone that can be harvested between the brachioradialis and pronator teres muscle insertions.
In an effort to reduce the morbidity at the donor site and therefore safely make use of the superior soft tissue characteristics of the volar forearm, biomechanical studies demonstrated greatly improved strength when a reconstruction plate is prophylactically applied to the donor radius after graft harvest. Studies from two institutions assessing over 100 patients, who underwent osteocutaneous radial forearm free flap (OCRFFF) harvest and prophylactic plating, reported only two instances of postoperative fracture of the radius. In both cases, the fracture occurred distal to the reconstruction plate after the patient fell. The OCRFFF has the advantage of tremendous soft tissue versatility. A long vascular pedicle, large amounts of thin pliable skin, and reliable sensory innervation make the soft tissue components of the RFFF ideal for the reconstruction of the tongue, floor of the mouth, alveolar ridge, pharyngeal wall, and soft palate. The available radius bone (9 to 12 cm) is of adequate length for reconstruction of many limited defects of the mandible and maxilla.
SURGICAL TECHNIQUE
Flap Harvest Technique
The RFFF is based on the radial artery, which branches from the brachial artery in the antecubital fossa. Its venous drainage is provided by the paired venae comitantes that run with the radial artery, and the superficial venous system, which contains the cephalic and basilic veins. The lateral intermuscular septum, which contains perforators from the radial artery supplying the periosteum of the radius, passes between the flexor carpi radialis and the brachioradialis muscles and must be preserved. Sensation of the flap is provided by the lateral and medial antebrachial cutaneous nerves.
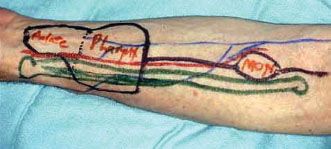
Preoperatively, an Allen test is performed to confirm adequate circulation to the hand via the ulnar artery and to assist in the selection of the donor arm. At surgery, the radial artery and cephalic vein are marked, along with the proposed skin paddle. The soft tissue component is measured, and the flap outline is drawn on the volar aspect of the forearm (Fig. 24.3). The skin paddle is positioned at least 2 cm proximal to the wrist crease and with an ulnar bias. This ensures adequate skin coverage of the internal fixation plate. The soft tissue component of the flap is raised in the standard fashion, with care taken to preserve the lateral intermuscular septum. An incision is made in the skin proximal to the paddle up to the antecubital fossa, and the skin flaps are reflected. The skin paddle is the outlined and raised with the deep fascia to the level of the brachioradialis and flexor carpi radialis tendons. Careful dissection medial to the cephalic vein and radial artery to the vascular pedicle preserves the superficial branch of the radial nerve intact. The radial artery and the vena comitans are ligated, and the pedicle and the fascia are raised for approximately 1 to 2 cm. The available bone lies in between the insertion of the pronator teres muscle and the insertion of the tendon of the brachioradialis muscle. Lateral retraction of the brachioradialis tendon exposes the radial surface of the bone.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


