The Fadenoperation
James B. Sprague
In 1974, Cüppers described the “Fadenoperation” at the second meeting of the International Strabismological Association.1 Two years later, Mühlendyck presented this new procedure to a US audience.2 Numerous reports subsequently appeared in the US and European literature on appropriate applications for this new technique, and on their success.3,4,5,6,7,8,9
Cüppers called his technique the “Fadenoperation,” or “string operation” because “faden” means suture or string in German. The common English usage, “faden suture,” is thus redundant. The procedure has also been called “arc of contact surgery,” “the posterior fixation procedure,” and “retro-equatorial myopexy.” In this chapter, I have used de Decker’s abbreviation “Fd” for the procedure as both noun and adjective.
This chapter describes the theory of Fd, its indications, surgical techniques and complications. Although I have relied primarily on material readily available in English for the US reader, I have expanded the European references in this revision because Fd remains more popular in Europe than in the United States.
THEORY
In 1941, Peter suggested weakening a rectus muscle by suturing it posteriorly to the sclera.10 In 1958, Tour and Asbury11 noted that the rectus muscle has rotational effect that extends as long as its direction of tangency, at which point the muscle becomes progressively more of a retractor and less of a rotator. Cüppers1 reasoned that suturing the muscle to the posterior sclera would create artificial paralysis, or a controlled incomitance, by weakening the rotational ability of a muscle only in its field of action. This was his so-called dynamic angle. He felt that the balance of forces between agonist and antagonist in primary position would not change. If there was strabismus in primary gaze, the so-called static angle, he added a standard recession to the muscle treated with posterior fixation.
Alan Scott diagrammed the mechanics of Fd.12 He suggested that changing the arc of contact of the muscle with the globe reduces the lever arm formed by the muscle insertion, the center of rotation of the globe, and the origin of the muscle (Fig. 1). Scott’s mechanical model suggested that the posterior suture needed to be 10 to 12 mm from the insertion for the medial rectus, 12 to 14 for the superior and lateral recti, and 14 to 16 for the lateral rectus.
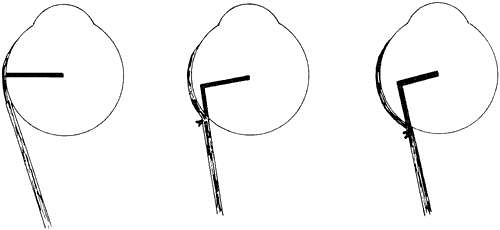 Fig. 1. The lever arm between the center of rotation and the muscle’s insertion and origin is shortened as the effective insertion of the muscle is moved posteriorly. |
Kushner measured saccadic velocity after the Fd.13 He expected to find decreased velocity in the field of the operated muscle but did not. He questioned whether the Fd changed the torque active on the muscle as would be suggested by the lever arm theory and also noted that the lever arm theory would not explain the effect of Fd without a recession. He stressed the effect of the amount of muscle contained in the suture and how effectively it was immobilized to explain the clinical effect of the operation.
Clark and colleagues14 examined the theory of the Fd in the context of the extraocular muscle pulleys previously described by Demer and coworkers,15 who described connective tissue sleeves that envelop and position each rectus muscle. Given that the anterior portion of the sleeve overlies the area at the equator where the posterior fixation suture is placed, they suggested that displacement of the pulley sleeve by the posterior suture itself or by extensive sharp dissection posteriorly results in mechanical restriction rather than a reduction in torque during muscle contraction. Their studies that used magnetic resonance imaging (MRI) did not show a change in tangency and thus did not predict a reduction in torque to explain the effect of the Fd. Mechanical restriction created by the Fd would explain the effect of the procedure without simultaneous recession of the muscle. It could also explain the variable results that many researchers have noted.
Regardless of the theory of how it works, there are five points to consider in applying the theory of the Fd in clinical practice and also in evaluating the literature:
First, it is important to determine how far posteriorly the fixation suture ought to be placed from the limbus. From the point of view of the mechanical model, this determines how much the lever arm is shortened, and thus the farther back such placement is made, the better will the result be. With the pulley model, extensive posterior orbital dissection could damage the anterior pulley slings and reduce the desired mechanical restriction to ocular movement. However, many surgeons try to put the suture(s) as far back as possible. For example, Biglan (Biglan AW, personal communication, 2000) has suggested going back 14 mm on the superior rectus for mild dissociated vertical deviation (DVD), 14.5 mm for moderate, and 15 mm for severe deviations. H. Eggers (personal communication, 2000) attempts to go back 15 mm on the medial rectus for high accomodative:convergence accommodation (AC:A) esotropia. Peterseim and Buckley16 placed medial rectus sutures an average of 18.3 mm (range, 15 to 20.5 mm). De Decker4 found that unsuccessful cases on reoperation did not have the suture placed as far posteriorly as the initial surgeon had claimed.
Second, the scleral suture (or sutures) needs to be heavy and deep enough to hold firmly4 and the knots into the muscle have to be tight enough to stay posterior.17 The amount of muscle incorporated in the sutures is important and could explain variable results.13
Third, simultaneous recession augments the procedure. Sprague and colleagues5 advocatedrecession of the superior rectus for DVD after disappointing results without it. Although undercorrection is a problem with DVD, large simultaneous medial rectus recessions may lead to overcorrections. In addition, if the posterior suture is placed before the muscle is recessed, the slack in the muscle will be anterior to the posterior attachment. Alan Scott pointed out that it is more effective to allow the slack created by the recession to fall behind the posterior suture, in effect doing the recession first and then placing the posterior suture (Fig. 2).12
Fourth, previous recession can be augmented with the Fd alone without the need to recess the muscle further or consider a marginal myotomy.16,18,19
Fifth, the Fd may weaken the operated muscle by tissue destruction and scarring.4,7 In rabbit studies, Alio and associates20 found muscle degeneration at the point of posterior fixation as well as anterior to the insertion. The Fd may lead to muscle stiffening, as shown by Castenera.21 De Decker found on reoperation that there was adherence of the muscle to the globe anterior to the posterior suture if a recession had been done.4
 Fig. 2. A. Posterior fixation alone. Recession added with the slack created left in front of the suture (B) and with the suture brought forward in the muscle, so that the slack is posterior to the suture (C). |
TECHNIQUE
Cüppers1 described disinserting the muscle, placing two sutures though the sclera under the muscle, and then bringing them through the muscle. This is thought to spare the center of the muscle and the circulation of the ciliary vessels. De Decker4 used two sutures at the muscle edge, but preferred to leave the muscle in place if a simultaneous recession was not needed. He also preferred to secure the muscle with a triple loop to prevent it’s sliding through the suture. Mühlendyck2,17 used a similar technique including 2 mm of the muscle on each side. He stressed the importance of the knot’s being tight and described a patient who had initially done well but whose ocular deviation had returned. The suture had slipped and the knot had migrated forward.17 He also stressed the importance of avoiding the long ciliary arteries and parasympathetic nerves. For the superior rectus, Sprague and colleagues5 preferred a single double armed suture brought up through the middle of the muscle and tied on its orbital surface.8
When simultaneous recession was not indicated, Castilla and colleagues22 passed a suture over the muscle with attachments to the sclera at each edge. Eggers (personal comunication, 2000) has used Supramid sutures for this. Schroeder and Schroeder23 suggested tying a 17-mm section of 2-mm wide silicon band across the muscle. The muscle can then slide under the suture or band, with an effective posterior point of tangency. This technique is claimed to restrict the muscle without increasing muscle stiffness and with minimal scar, thus facilitating reoperation.
Exposure is a major problem in performing the Fd, so as to place the suture posteriorly while at the same time avoiding unnecessary dissection. A fiberoptic headlight and loupe magnification are always used. The technique followed by Sprague and colleagues5 uses a limbal incision. The muscle is isolated on a suture and cleaned of fascial attachments. An extra suture marks the muscle where the posterior fixation suture will engage it (Fig. 3). This indicates the distance back from which that the posterior fixation suture will be placed, less the amount of recession. The slack created by the recession is therefore posterior to the posterior fixation suture.
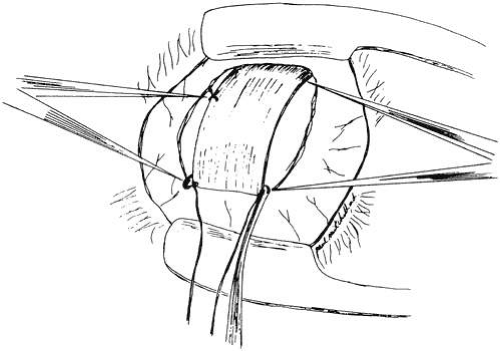 Fig. 3. The muscle (here the superior rectus) is isolated. The muscle is marked where the suture will come through it (caliper on left), anterior to the point on the sclera where the suture will be placed (caliper on right). |
The muscle is released from the globe and the globe is held over with a traction suture woven through the insertion. Small, malleable brain retractors or thin orbital retractors under the muscle hold the muscle and orbital contents back (Fig. 4). The scleral sutures will determine how the muscle is to be displaced: vertically in the case of the horizontal recti, horizontally in the case of the vertical recti. Two sutures are used on the medial rectus to avoid the long ciliary vessels in the sclera that can be cut with a single central suture. On the vertical muscles, a single suture in the middle can be used (Fig. 5). In both the one- and two-suture techniques, the needle pass through the sclera must be deep enough to prevent the suture from pulling out. The suture is brought through the muscle (see Fig. 5) and tied (Fig. 6). The recession is completed (see Fig. 6). There should be no tension on the muscle between the posterior suture and the new insertion of the recessed muscle. A videotape has been produced by Gerhard Cibis, which illustrates this surgical procedure.24
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


