The Facial Nerve— Cranial Nerve VII
Many of the advances in surgical and frontal techniques have forced the surgeon to understand the course of the temporal and zygomatic branches exactly. The following pictures present crucial data that involve the correlation of many studies. The numbers must be absorbed, yet the surgeon must understand that absolutes never exist in anatomy. Clinical injection studies depict the real-life effects of nerve loss, and a case will validate that study.
I have taken the liberty of making certain safety decisions. For example, if a study shows the facial nerve between 3.5 and 4.5 cm from a point, I always chose the closest number, so the surgeon would have some margin of protection.
Data to read and reread after reviewing the upcoming pictures:
1 Two to five facial nerve branches cross the zygomatic arch. These are the frontal or temporal branches of cranial nerve VII.
2 These nerves cross the arch between 0.8 and 3.5 cm anterior to the external acoustic canal (EAC). At 2.5 cm from the EAC, branches can always be found just above the periosteum on the arch.
3 The most anterior temporal branch provides motor to the upper lid orbicularis oculi, entering the orbicularis oculi 2.1 to 3.5 cm above the bony lateral canthus (average: 2.8 cm).
4 A safe zone can be designated starting at the zygomatic arch anteriorly. The first 2 cm posterior to the lower lateral orbit rim (actually, the lateral border of the orbital portion of the zygoma) is safe at the arch level.
5 At the level of the bony lateral canthus over the temporalis fascia, the most anterior branch is at least 3.5 cm away (3.9 ± 0.4 cm).
6 The nerve rarely enters the frontalis muscle beyond 4 cm above the bony lateral canthus, or usually 2 cm above the lateral brow. The brow is a less reliable anatomic point.
7 The frontal branch of the superficial temporal artery can often be noted in the lateral forehead and can be used to mark the highest possible nerve entrance into the frontalis muscle.
8 The safe zone at 3.5 cm can be marked “digitally” along the rim during sub SMAS surgery (Fig. 2.14) to allow for safe transection of ligaments that go to the skin under the superficial musculo-aponeurotic system (SMAS) layer (see Fig. 2.15).
9 The bare zygomatic arch or deep temporal fascia can be safely exposed anteriorly in the 2-cm zone behind the rim. Posterior to that, a cut in the fascia where it splits to envelop the arch is required to get to the back of the arch without any nerve injury. A similar posterior approach behind the front leaf of split fascia can be used to reach the posterior arch, and subperiosteal elevation can be performed over the arch.
10 The zygomatic branch supplies the lower lid muscle and the zygomaticus muscles and lip levators anterior to that. The zygomatic branch also curves around the lower lid to supply the medial upper lid depressors. The depressor supercilii and the medial orbicularis in the upper lid on the same side are supplied by the zygomatic branches as they curve around the canthal region.
11 The orbicularis oculi muscle (upper) is usually supplied by the most anterior temporal branch to cross the zygomatic arch. Motor shoots to the lower orbicularis oculi from the zygomatic branch often separate proximally either within or just outside the parotid to cross the arch into the deep fat before going to supply the muscle. This branch starts prior to the zygomaticocutaneous ligaments. The main zygomatic branch, however, just below the zygomaticocutaneous ligaments provides key nerves to the orbicularis oculi just before passing to the deep side of the zygomaticus major, which it supplies. This branch continues on to the surface of the zygomaticus minor (supplying it) and becomes more vertical.
Thus, the lower orbicularis muscle has transverse nerve fibers to it from the zygomatic branch which may explain why leaving this pretarsal muscle (innervated) may be helpful during blepharoplasty. Also, the preseptal and orbital fibers have vertical fibers supplying it from the zygomatic branch of cranial nerve VII.
 Figure 2.1 The purple line along the anterior tragus (T) is the front of the external acoustic canal (EAC). Most of the cranial nerve VII branches can be found about 2.5 cm in front of the EAC (range: 0.8 cm to 3.5 cm). The lower arrow shows the articular eminence to be at about 2.5 cm from the anterior border of the canal. |
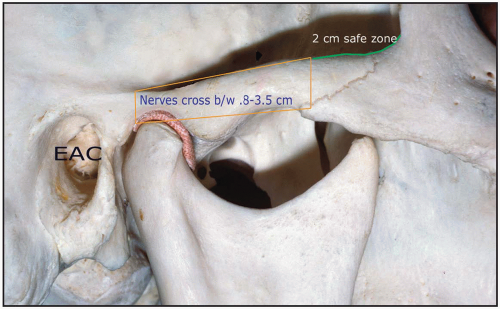 Figure 2.2 Along the upper arch anteriorly, for the 2 cm posterior to the lateral orbital rim, there are no key nerves, so this area and the fascia above are safe for sutures for that 2-cm distance. |
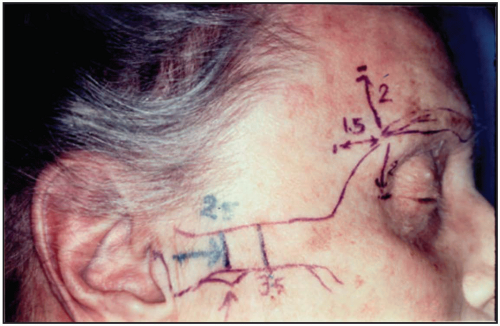 Figure 2.3 The eyebrow is a soft reference point. Therefore, saying the nerve is usually 1.5 cm lateral to it also becomes soft information. Note the horizontal line above the 2 on the forehead. Here, the anterior branch of the superficial temporal artery can often be palpated in vivo. The nerves are practically below the artery, usually in the first 2 cm above the lateral brow. Rarely are the nerves beyond 4 cm from the bony lateral canthus (horizontal line lateral to canthus). |
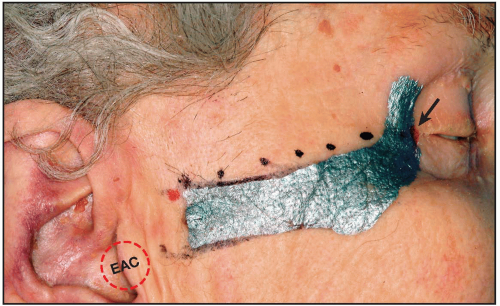 Figure 2.4 1. The bone is marked with silver. 2. Posterior red dot is 8 mm from the EAM (external acoustic meatus) or EAC. 3. Anterior red dot (canal) (arrow) appears at the bony lateral canthus. 4. Black dots connect the red dots and follow the upper arch closely. Note that the horizontal width of the lateral orbital rim prior to its turn back to become arch is about 1.3 cm to 1.5 cm. |
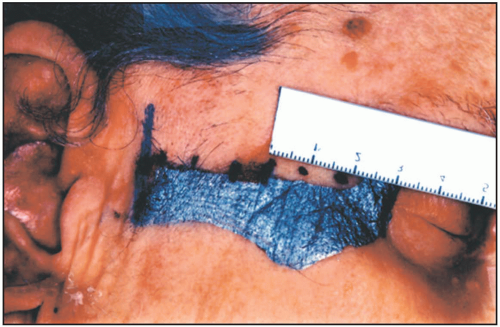 Figure 2.5 The first 2 cm behind the lateral orbital rim is a safe area. The long vertical blue line is at 0.8 cm. The most anterior vertical blue line is at 3.5 cm. Nerves are always between the front and back blue lines. |
 Figure 2.6 The black fill indicates the start of marking a safe zone 2 cm behind the lateral orbital rim (LOR). |
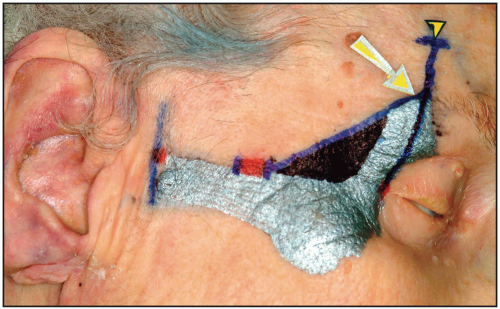 Figure 2.7 The highest point where the nerve enters the frontalis (yellow/black dart) is at least 4 cm above the bony lateral canthus (red dot) (range 2.85 ± 0.7 cm). The height of the yellow arrow at 2.85 cm above the bony canthus is the level where the most anterior branch enters the orbicularis oculi lateral border. Note, however, that the orbicularis border is more than 1 cm lateral to this point, as you will see. |
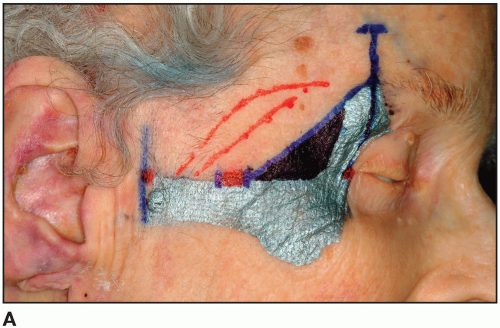 Figure 2.8A The red lines show that the nerve’s pathways may be relatively straight or curved as shown. The red lines stop at the point where the anterior branch would enter the upper orbicularis oculi. |
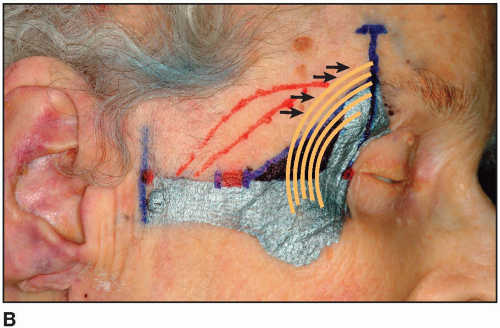 Figure 2.8B The longer arrow in Figure 2.7 shows the average height at which the most anterior branch of the frontal group enters the orbicularis. In fact, its from 2.1 to 3.5 cm from the bony canthus. If the orbucularis oculi muscle is then ghosted in (orange brown), the arrows then depict the possible entrance of the anterior branch into the upper lid orbicularis. See Figures 2.10B, 2.12, and 2.13 for actual dissections of this.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|