Fig. 12.2
Rhinitis sicca anterior with dry skin in the nasal vestibule and thin yellowish crusts
12.2 Etiology
Possible causes of dry nose include a variety of diseases, external and internal factors and environmental conditions:
Local mechanical irritation.
Climatic or environmental factors.
Dry room or environmental air (relative humidity <50 %)
Heated room or hot environment
Long-distance flights
Workplace conditions.
Dry air and clean-room condition (Su et al. 2009)
Cold and heat
Dusty conditions (e.g. grinding/polishing of plaster, granite, chalk, cement, wood arsenic, nickel carbonyl, tobacco smoke)
Drugs (cocaine).
Side effects of medications (see Table 12.1).
Supportive nasal administration of oxygen (Miyamoto and Nishimura 2008).
Symptoms of other diseases (granulomatous, infectious, rheumatic and immunological disorders).
Wegener’s granulomatosis, sarcoidosis, tuberculosis, syphilis and leprosy (Fig. 12.1)
Wound healing phase after endonasal sinus surgery and surgery on the nose.
Anatomical changes to the outer and inner nose, with modification of normal airflow.
Allergic rhinitis, in particular house dust mites and moulds.
Permanent sequelae of surgery on the nose and paranasal sinuses.
Sequelae of head and neck radiotherapy.
Patients with obstructive sleep apnoea (OSA) or continuous positive airway pressure (CPAP) treatment in sleep apnoea patients (Brander et al. 1999). Moistening led to a reduction in symptoms (Worsnop et al. 2009).
Old age.
Table 12.1
Medications with the side effect dry nose
Substance group | Generic name | Indications |
|---|---|---|
Retinoids (1–10 %) | Isotretinoin | Severe forms of acne |
Tretinoin | Promyelocyte leukaemia | |
Doxepin (tricyclic antidepressant) | Depressive conditions, anxiety syndrome, mild withdrawal symptoms in alcoholics and drug-dependent persons, agitation, sleep disorders | |
Methyldopa (1 ‰–1 %) | Hypertension (of pregnancy) | |
Sympathomimetics (local) | Dipivefrine (eye) | Glaucoma |
Naphazoline | Diverse forms of rhinitis, only short-term use recommended | |
Oxymetazoline | ||
Phenylephrine | ||
Tetryzoline | ||
Tramazoline | ||
Xylometazoline | ||
Antihistaminics, first generation | Clemastine | Urticaria, allergic rhinitis |
Dimenhydrinate | Vertigo, nausea, vomiting | |
Dimethindene | Itching, itching dermatoses, allergies | |
Diphenhydramine | Difficulty getting to sleep, difficulty staying asleep | |
Promethazine | Agitation in underlying psychiatric illnesses, possibly vomiting, nausea and sleep disorders | |
Terfenadine | Allergic rhinoconjunctivitis, allergic skin disorders |
Dry nose may be the first symptom of an incipient cold with a runny nose; in such a case, however, it is of only limited duration.
Although an increased susceptibility for infections has frequently been postulated and is pathophysiologically plausible, it has never been confirmed as the sole cause. The mechanical and functional integrity of the mucous membrane is considered a major natural defence mechanism against infection. Depending on the degree to which it dries out, mucociliary transport and even the epithelial barrier may be impaired.
Epidemiological data on the prevalence of dry nose are not available. However, in particular when questioned, many people confess to be sufferers and admit to the use of numerous therapeutic measures, mostly ointments and sprays or nasal douches.
In old age, anatomical changes and an involution atrophy of the mucosa result in an increase in such complaints as impairment of nasal breathing and dry nose, and the following phenomena may occur:
Hanging nasal tip and shortening of the columella (Zankl et al. 2002)
Reduced mucociliary clearance (Ho et al. 2001; Sakakura et al. 1983; Armengot et al. 1993; Sunwoo et al. 2006)
Reduction in the number of goblet cells and elastic fibres in the nasal mucosa (Sahin-Yilmaz and Corey 2006)
Reduced sensitivity of the nasal mucosa (Wrobel et al. 2006)
Enlargement of the nasal cavity resulting from involution atrophy of the nasal mucosa (Kalmovich et al. 2005; Lindemann et al. 2005a)
Decrease in the body’s water content (Slavin 2009)
Altered airflow due to changes in geometry leads to changes in the conditioning situation (Lindemann et al. 2005a, b), with the result that in over 60-year-olds, the air-conditioning capacity becomes impaired: both intranasal air temperature and humidity decrease (Lindemann et al. 2008).
A familial, i.e. genetic, impairment of nasal air-conditioning has been reported by Sahin-Yilmaz et al. (2007), who investigated 47 pairs of twins (Sahin-Yilmaz and Corey 2006).
12.2.1 Clinical Entities
In common with the symptom itself, a number of individual diseases associated with the symptom dry nose and crusting are not only unclearly defined but also overlap. In the literature, the following descriptions are to be found:
Rhinitis sicca anterior (Fig. 12.2)
Primary rhinitis atrophicans/primary atrophic rhinitis (= PAR) – rhinitis atrophicans with foetor (ozaena) (Fig. 12.3)
Secondary rhinitis atrophicans/secondary or diffuse atrophic rhinitis (= SAR)
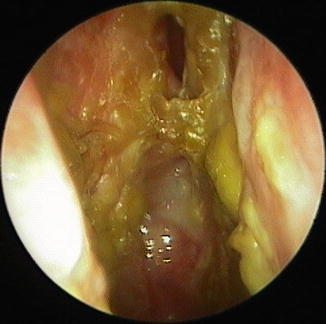
Fig. 12.3
Dry nose with persistent excessive crusting in a female patient with primary atrophic rhinitis
12.2.1.1 Rhinitis Sicca Anterior
The term rhinitis sicca anterior defines a chronic inflammation in the region of the anterior part of the nose usually affecting the anterior and caudal septum and/or the corresponding lateral nasal vestibule. Due to irritation (mechanical, finger picking; toxic; persistent secretion; respiration; (air)flow characteristics; dry, hot and dusty environment), drying, superficial erosion and/or ulceration with (thin) crust formation occur.
Patients experience a sensation of dryness, itching and increased crust formation. The crusts are thin and dry and do not extend into the posterior part of the nasal cavity, as is the case with atrophic rhinitis. Usually there is no foetid smell – only an occasional patient experiences mild foetor caused by bacterial colonisation of the small crusts. Manipulations may give rise to a vicious circle of increased crusting and persistent complaints. In the individual case, continued irritation and manipulation may result in perforation of the nasal septum.
Treatment consists in the application of a protective film to the skin of the nasal vestibule, to allow the chronic inflammation disrupting its integrity to self-heal while avoiding mechanical irritation (Fig. 12.1). This is usually achieved by the application of ointments. Nasal sprays containing dexpanthenol have also been used with success (Kehrl and Sonnemann 1998).
12.2.1.2 Primary Atrophic Rhinitis (PAR)
Primary atrophic rhinitis is a gradually progressive chronic degenerative condition of the nasal mucosa of unknown etiology. Progressive atrophy of all the constituents of the mucosa (epithelium, glands and vessels together with osteoclasis) mainly affects the turbinates. The respiratory epithelium undergoes stepwise metaplastic changes. Histologically, atrophy of the serous and mucous glands, loss of the cilia and goblet cells, chronic infiltration of the lamina propria with granulations and scar formation are seen. Some publications also report diminished vascular density together with peri- and endarteritis. The histological changes explain the disturbance to mucociliary transport. Thick secretion that is not transported away promotes the formation of bacterially contaminated crusts that may then be a source of recurrent bacterial Infection. If rhinitis atrophicans is complicated by foetid crust formation, rhinitis atrophicans with foetor (stinking nose, ozaena) results. Microbiological investigation usually detects Klebsiella ozaenae (100 % of the 45 patients of Moore and Kern (2001)) but also Staphylococcus aureus, Proteus mirabilis, E. coli and other bacteria (Bordetella bronchiseptica and Pasteurella multocida). Endoscopic examination reveals a markedly large and wide nasal cavity and visibly dry mucosa. The turbinates are clearly diminished in size. With ozaena, yellowish-green crusts are found on the mucosa. Apart from crusting, the patient usually also suffers from hypo- or anosmia. Foetor may give rise to social problems.
The cause of PAR is unknown, but both genetic and infectious causes are under discussion. The condition is more commonly seen in association with low socio-economic status, a poor diet and iron deficiency. A much less frequent use of antibiotics in countries with a higher incidence of the condition may have a role to play. The fact that women are more frequently affected suggests a possible endocrinal factor. Over the past years and decades the prevalence of PAR has declined.
12.2.1.3 Secondary Atrophic Rhinitis (SAR)
Secondary atrophic rhinitis develops in the soil of an underlying disease or may result from previous therapeutic measures. Therefore, it is a collective term for several conditions with a different etiology but a similar clinical feature with the subjective feeling of a dry nose, crusting, gegebenenfalls nasal obstruction, foul smelling and epistaxis as outlined above. In contrast to PAR, there is no osteoclastic activity, so the term diffuse atrophic rhinitis may be more suitable. Pathogenetic factors leading to SAR are:
Prior radical endonasal surgery. Persistent chronic rhinosinusitis in addition may increase the probability of the development of SAR (Ly et al. 2009).
Prior radiotherapy of the head and neck.
Sjögren’s syndrome.
Extremely rarely: prior trauma.
In the largest collection of cases to date 197 patients with sRA the following causes were identified (Moore and Kern 2001):
Complete removal of the lower and middle nasal turbinates (24 %)
Partial removal of the lower and/or middle nasal turbinates (56 %)
Endonasal sinus surgery without turbinectomy (10 %)
Partial maxillectomy to remove a tumour (6 %)
Nasal trauma requiring surgical reconstruction (1 %)
Granulomatous disease (1 %)
Empty nose syndrome (ENS) is defined as a form of iatrogenic SAR, occurring after radical endonasal surgery in particular resection of the nasal turbinates (lower and/or middle), usually in connection with an operation on the nasal sinuses (Chhabra and Houser 2009; Payne 2009; Scheithauer 2010). It is characterised by the symptoms nasal and pharyngeal dryness, paradoxical impairment of nasal respiration, dyspnoea and hyposmia, in some cases associated with depression (Houser 2007).
The disturbed sense of smell is the result of the changed airflow. The dryness of the pharyngeal mucosae is due to the fact that, in contrast to the normal situation, drier intranasal air (no moisture since turbinate mucosa is lacking) results in disrupted airflow in the region of the choanae and also impinges on the posterior wall of the nasopharynx at increased velocity (Scheithauer 2010). According to Houser, pain too is a typical symptom caused by the action of cold air on the mucosa covering the sphenopalatine ganglion (Houser 2007).
Resection of the lower and middle turbinates reduces the effectiveness of the climatisation function of the nose by 23 % (Naftali et al. 2005; Passàli et al. 1999). The paradoxical impairment of nasal respiration is explained by the unphysiological airflow, the reduced nasal airway resistance, the lack of areas of functional mucosa together with the simultaneous enlargement of the nasal cavity and the curtailed contact between air and mucosa (Scheithauer 2010). Enlargement of the nasal cross section reduces the airway resistance and thus the pressure gradient at the air/mucosa surface. In turn, this causes malfunction of the nasopulmonary reflexes, which may lead to a worsening of pulmonary function. In contrast, optimal nasal airway resistance is important for the dilatation of the peripheral bronchioles and for improved alveolar gas exchange.
The risk to develop SAR after resection of the turbinates depends on the extent of resection, individual factors of the patient itself and other external factors which are not clearly defined up to now. Some authors did not find any sign of SAR after total resection of the inferior turbinates (Cook et al. 1995; Eliashar 2001; Ophir 1990; Talmon et al. 2000); others report SAR in 2–22 % (Passàli et al. 1999; Courtiss and Goldwyn 1990; Elwany and Harrison 1990; Martinez et al. 1983; Oburra 1995; Odetoyinbo 1987).
12.3 Diagnosis
Extensive history taking is always followed by inspection of the outer and inner nose (Table 12.2). This should, for example, identify any anatomical deformations that might cause dry nose by changing the flow of air through the nose. For the purpose of detecting minor lesions in the nasal vestibule in patients with rhinitis sicca anterior, the use of a microscope may prove useful. Endonasal inspection should look for septal deviation or perforation and note the size and shape of the turbinates, the presence and nature of crusts, the humidity of the mucosa, polyps or tumours, postnasal secretion and the nasopharyngeal status.
Table 12.2
Diagnostic workup of dry nose
Medical history |
Inspection of the external and inner nose |
Endoscopy of the nasal cavity and nasopharynx, where indicated, also of (operated) paranasal sinuses |
Where indicated, CT of the paranasal sinuses |
Allergy testing |
Microbiological swab |
A CT of the nasal sinuses is indicated when signs of chronic rhinosinusitis are found or to obtain adjunctive evidence of PAR. Typical signs of PAR in the CT include:
Thickened mucosa in the paranasal sinuses.
The osteomeatal complex can no longer be defined due to the destruction of the normal anatomy.
Hypoplasia of the maxillary sinus.
Enlargement of the nasal cavity with destruction of the lateral nasal wall.
Bony destruction of the inferior and middle turbinates.
Testing for allergy is important, for example, in order to diagnose a house mite allergy, which may be associated with the symptom dry nose. When endoscopic examination reveals purulent streaks or crusting, swabs should be taken for a microbiological examination.
The diagnosis is based on the case history, endoscopic findings and, where necessary, adjunctive diagnostic measures.
12.4 Treatment
Treatment of dry nose comprises:
Elimination or amelioration of triggering or promoting factors
Moisturisation (Table 12.3)
Sufficient daily drinking amount
Cleansing (when crusts are present) and care of the mucosa
Treatment of obvious infections
Where applicable, the elimination of an overlarge endonasal air space
The individual may have only limited control over environmental factors. The importance of the latter is obvious when dry nose is no longer experienced during a holiday but reappears when this is over.
By far the most common complaint is a subjective dry nose with no endoscopic findings with the possible exception of a somewhat dry mucosa in the anterior nose. This is the case in almost all those patients exposed to unfavourable climatic or workplace conditions and also the large group of patients with obstructive sleep apnoea syndrome undergoing CPAP treatment. Also affected are patients operated on the nose, before the climatisation function has normalised.
Apart from the strict avoidance of local manipulation, these patients require humidification and care of the dry areas. For this purpose the market offers wide range of ointments, oils, sprays and nasal irrigation (Table 12.4).
Table 12.4




Basic rules for the treatment of dry nose
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
