Purpose
To determine the 24-hour effects of travoprost with sofZia on intraocular pressure (IOP) and ocular perfusion pressure as well as the endurance of IOP lowering after last dosing.
Design
Prospective, open-label study.
Methods
Forty subjects with open-angle glaucoma or ocular hypertension were admitted to our sleep laboratory for three 24-hour sessions monitoring IOP, blood pressure (BP), and heart rate. The first baseline session occurred after medication washout or immediately after enrollment for treatment-naïve patients. A second 24-hour monitoring session was performed after 4 weeks of once-nightly treatment of travoprost with sofZia. The medication was then discontinued and a third 24-hour session was completed 60-84 hours after the last dose taken. IOP measurements were taken using a pneumotonometer every 2 hours in the sitting position during the 16-hour diurnal period and in the supine position during the 8-hour nocturnal period. Ocular perfusion pressure was defined as 2/3[diastolic BP + 1/3(systolic BP − diastolic BP)] − IOP.
Results
Treatment with travoprost with sofZia significantly lowered mean diurnal and nocturnal IOP levels from baseline (diurnal 18.1 ± 3.9 to 15.3 ± 3.3 mm Hg; nocturnal 20.6 ± 3.6 to 19.4 ± 3.4 mm Hg, P < .01 for both). Once treatment was discontinued, mean IOP remained at levels significantly less than baseline during both the diurnal (16.6 ± 3.8 mm Hg) and nocturnal periods (19.4 ± 3.5 mm Hg). Mean baseline ocular perfusion pressure was significantly increased during the diurnal but not the nocturnal period (diurnal 73.7 ± 11.4 to 76.5 ± 10.3 mm Hg, P = .01; nocturnal 64.4 ± 12.6 to 64.2 ± 11.1 mm Hg, P = .67).
Conclusion
Travoprost with sofZia significantly lowers IOP throughout the diurnal and nocturnal periods, and increases ocular perfusion pressure in the diurnal, but not the nocturnal, period in open-angle glaucoma and ocular hypertension. The treatment effect on IOP endures for at least 84 hours after the last dose.
Treatment of glaucoma centers on the reduction of intraocular pressure (IOP). While several laser and surgical therapies are available, topical medication continues to be a commonly used initial treatment option. Owing to their once-daily dosing, excellent efficacy, and favorable side effect profile, the prostaglandin analogues are frequently chosen as the first-line medication for the reduction of IOP in most forms of glaucoma and ocular hypertension. It is believed that prostaglandin analogues lower IOP primarily by increasing aqueous outflow through the uveoscleral pathway. Based on more recent evidence, these medications may also augment the traditional outflow pathway through the trabecular meshwork and Schlemm canal. There are currently several molecules within the prostaglandin analogue class that are commercially available, with each having a distinct profile for pressure lowering and tolerability.
Travoprost (Travatan; Alcon, Fort Worth, Texas, USA) was first approved by the Food and Drug Administration (FDA) in 2001. The multi-dose bottle for travoprost available in the United States was originally preserved with the detergent preservative benzalkonium chloride (BAK). This formulation has been previously shown to significantly lower IOP during both the diurnal and nocturnal periods in patients with open-angle glaucoma and ocular hypertension. A report by Sit and associates has demonstrated a durable IOP-lowering response of travoprost with BAK for 41-63 hours after last dose. Despite its efficacy and widespread use in ophthalmic medications, chronic use of BAK can have several negative effects on ocular tissues in specific patient populations. Prolonged BAK exposure in cell culture models results in arrest of cell growth, apoptosis, and even necrosis at very high doses. These detrimental effects are implicated in ocular surface disease that is frequently present in patients taking multiple BAK-preserved medications. In 2006, BAK was removed from travoprost and replaced with a novel ionic-buffered preservative system called sofZia (Travatan Z; Alcon). After application on the ocular surface, sofZia components break up into innate ingredients with the theoretical benefit of decreased hyperemia and improved tolerability, although results from published studies are conflicting.
Recent studies have shown that travoprost with sofZia lowers IOP with a profile similar to the original formulation; however, the effects throughout a 24-hour cycle including the nocturnal period are poorly characterized. In a report by Gross and associates, travoprost with sofZia was shown to have a prolonged duration of action up to 60 hours. The effect of travoprost with sofZia on IOP beyond this time remains unknown. In this study, we seek to further evaluate the IOP-lowering effect of travoprost with sofZia in patients with open-angle glaucoma and ocular hypertension and assess the durability of effect up to 84 hours after last dose taken. Furthermore, we aim to characterize the medication’s effect on ocular perfusion pressure across the diurnal and nocturnal period.
Methods
Approval for this prospective, open-label study was obtained from the Colorado Multiple Institutional Review Board prior to initiation of the study, and the tenets of the Declaration of Helsinki were followed. Informed consent was obtained from all subjects prior to enrollment in the study. A total of 40 patients with open-angle glaucoma (OAG) or ocular hypertension (OHTN) were recruited during regularly scheduled examinations at the Rocky Mountain Lions Eye Institute, University of Colorado Denver. Inclusion criteria included patients of any sex or ethnicity with an existing or new diagnosis of ocular hypertension or open-angle glaucoma. Patients with ocular hypertension had untreated IOP reading >21 mm Hg on 2 or more office visits with otherwise normal optic nerve appearance and visual field testing. Patients with open-angle glaucoma possessed abnormal visual field testing (Humphrey Field Analyzer; Zeiss, Dublin, California, USA) and/or optic nerve findings consistent with glaucomatous damage including increased cup-to-disc ratio, notching, rim defects, hemorrhage, nerve fiber layer defects, or a combination of these. Office IOP readings were not considered in the inclusion or exclusion criteria. Exclusion criteria included women who were pregnant or planning to become pregnant, angle-closure glaucoma, narrow anterior chamber angle by gonioscopy (Schaffer grade <2), current smokers, irregular sleep patterns, inability to safely discontinue ocular glaucoma medications for 4 weeks, and history of cystoid macular edema, inflammatory eye disease, or herpes simplex viral infection.
After enrollment, subjects already taking topical glaucoma medications underwent a wash-out period of 4 weeks regardless of drug class before starting the study. Subjects not taking any glaucoma medications were allowed to proceed immediately to the first 24-hour study session. For each of 3 study sessions, subjects were admitted to a private bedroom at the University of Colorado Hospital Clinical and Translational Research Center for a 24-hour period. The first baseline session was performed off all glaucoma medications. A supply of travoprost with sofZia was then dispensed to the subject with instructions to place 1 drop nightly at approximately 9:00 PM in both eyes. After 4 weeks of therapy, subjects returned for their second 24-hour session. During this visit, the study medication was self-administered under supervision at the usual dosing time of 9:00 PM. After completion of the second study session, subjects were asked to discontinue the study medication and return for a third 24-hour session 3 days after the last dose was taken.
Subjects were not restricted in their activity during daytime hours of 6:00 AM to 10:00 PM, but were required to remain supine in bed during nighttime hours of 10:00 PM to 6:00 AM. Food and drink were provided to the subjects at their leisure. Measurements of IOP, blood pressure (BP), and heart rate were recorded every 2 hours by a trained ophthalmic technician or clinical nurse on each study session. All measurements were performed with the subject in the habitual position for that time. Readings taken during the diurnal period of 6:00 AM to 10:00 PM were done in the sitting position and those taken during the nocturnal period from 10:00 PM to 6:00 AM were done in the supine position. A total of 8 readings were performed during the diurnal period (7:00 AM, 9:00 AM, 11:00 AM, 1:00 PM, 3:00 PM, 5:00 PM, 7:00 PM, and 9:00 PM) and 4 readings in the nocturnal period (11:00 PM, 1:00 AM, 3:00 AM, and 5:00 AM) for each study session. A Model 30 pneumotonometer (Reichert Inc, Depew, New York, USA) was used for all IOP measurements. Topical proparacaine 0.5% was used for anesthesia before each reading. Measurements with standard deviations greater than 1.0 were discarded and retaken. All measurements were performed on both eyes as long as the eye met inclusion criteria. A standard automated sphygmomanometer was used to measure blood pressure and pulse at the time of each IOP measurement.
As previously described, ocular perfusion pressure was calculated as the difference between two thirds of the mean arterial blood pressure (MAP) and IOP (ocular perfusion pressure = 2/3MAP − IOP), where MAP was calculated as the diastolic blood pressure plus one third of the difference between systolic and diastolic blood pressures [MAP = DBP + 1/3(SBP − DBP)]. The means of IOP, ocular perfusion pressure, SBP, and DBP were calculated for each 2-hour time point as well as the diurnal period (8 readings in the upright position) and nocturnal period (4 readings in the supine position). For comparison of study metrics during each study period, mixed models were fit to the data and various contrasts were reported through linear combinations of the models’ parameters. Mixed models were specifically designed to take correlation from repeated measurements into account. The Pearson correlation coefficient (PCC) was used to assess the relationship between baseline IOP and absolute IOP reduction during treatment. All statistical analyses were performed using SAS 9.3 software (SAS Institute Inc, Cary, North Carolina, USA). Statistical significance was defined as P < .05.
Results
Of the 40 subjects enrolled, there were 28 women and 12 men with a mean age of 65 years (range: 43-84 years). There were 21 white, 13 African-American, 4 Hispanic, and 2 Asian patients. Diagnoses of subjects included primary open-angle glaucoma (37), ocular hypertension (2), and pigmentary glaucoma (1). All subjects completed the 3 study visits. The medication was well tolerated by all subjects, with no serious adverse events related to drug administration. Mean central corneal thickness was 541.0 ± 34.0 μm.
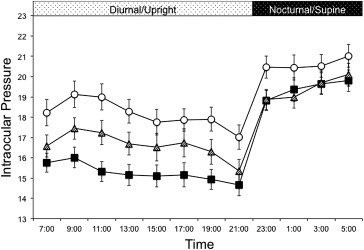
The 24-hour IOP profiles for each study visit are displayed in Figure 1 . After 4 weeks of travoprost with sofZia therapy, the mean IOP was significantly reduced at all time points during both the diurnal period (upright positioning) and nocturnal period (supine positioning) ( P < .05). The mean IOP for the entire diurnal period was significantly lowered from a baseline of 18.1 ± 3.9 mm Hg to 15.3 ± 3.3 mm Hg during treatment ( P < .01). Similarly, mean IOP during the nocturnal period was lowered from 20.6 ± 3.6 mm Hg at baseline to 19.4 ± 3.4 mm Hg on treatment ( P < .01). Three days after the last dose taken, the mean IOP during the diurnal period remained significantly lower than baseline (16.6 ± 3.8 mm Hg, P < .01) for the entire period and at each individual time point. The magnitude of IOP-lowering effect was less than during treatment ( P < .01). For the nocturnal period, the IOP-lowering effect was unchanged from active treatment even after 3 missed doses (19.4 ± 3.5 mm Hg, P = .4). The mean IOP for each study visit during the diurnal, nocturnal, and 24-hour period are listed in Table 1 . The relationship between baseline IOP level and absolute IOP reduction during treatment is displayed in Figure 2 . A significant, negative correlation was found with a PCC of −0.80 (95% confidence interval: −0.84 to −0.76, P < .01).
| Study Visit | Diurnal Period (Upright) | Difference From Baseline | P Value | Nocturnal Period (Supine) | Difference From Baseline | P Value | 24-Hour (Habitual) | Difference From Baseline | P Value |
|---|---|---|---|---|---|---|---|---|---|
| Baseline | 18.1 ± 3.9 | – | – | 20.6 ± 3.6 | – | – | 19.0 ± 3.8 | – | – |
| On treatment | 15.3 ± 3.3 | −2.9 | <.01 | 19.4 ± 3.4 | −1.2 | <.01 | 16.6 ± 3.3 | −2.3 | <.01 |
| After 3 missed doses | 16.6 ± 3.8 | −1.5 | <.01 | 19.4 ± 3.5 | −1.2 | <.01 | 17.5 ± 3.7 | −1.4 | <.01 |
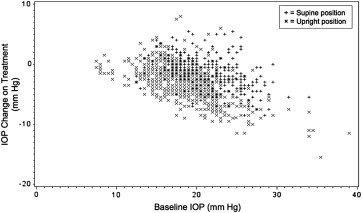
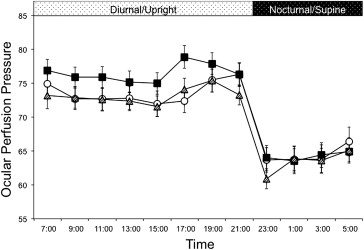
Figure 3 displays the 24-hour ocular perfusion pressure profiles for each study visit. The mean ocular perfusion pressure was significantly increased during travoprost with sofZia therapy, from a baseline of 73.7 ± 11.4 mm Hg to 76.5 ± 10.3 mm Hg ( P = .01) during the diurnal period, but was unchanged during the nocturnal period (64.4 ± 12.6 mm Hg to 64.2 ± 11.1 mm Hg, P = .67). This effect was no longer seen after 3 missed doses. The mean ocular perfusion pressure for each study visit during the diurnal, nocturnal, and 24-hour period are listed in Table 2 .