(1)
Department of Ophthalmology and Visual Sciences, University of Iowa Hospitals and Clinics, Iowa City, IA, USA
The cilioretinal arteries belong to the posterior ciliary artery system. They usually arise from the peripapillary choroid or directly from one of the short posterior ciliary arteries. The existence of the cilioretinal arteries is a congenital anomaly rather than one acquired due to some disease, inflammatory, or other morbid process. It was first described by Müller [1] in 1856 (Fig. 3.1) and first demonstrated histologically in 1876 by Nettleship [2], who stated that in sectioning of a human eye, he found “a small artery from the choroid turning round the edge of the disc, and running uninterruptedly for some distance in the retina, where it breaks up into capillaries.” Since then, there have been many reports of the presence of a cilioretinal artery (Table 3.1) [3–26]. Nettleship [27] in 1876 reported 7 cases of cilioretinal arteries. In 1879, he [3] published many important observations, still relevant, about the cilioretinal arteries. He stated the following:
Table 3.1
Presence of cilioretinal arteries in reported series
Author(s) | Year | Incidence | Number of cilioretinal arteries | Miscellaneous |
|---|---|---|---|---|
Nettleship [3] | 1876b | Usually one and sometimes 2 | ||
Loring [4] | 1872 | Only three cases | ||
Randall [5] | 1887 | 20 % | ||
Lang and Barrett [6] | 1888 | 16.7 % | One | |
1897, 1898 | 14 % | |||
Jackson [9] | 1911 | 19.1 % | Usually one and sometimes 2–3 | Large in 22.5 %, medium in 28.3 %, and small in 49.2 % |
Salzmann [10] | 1912 | 16.4 % | Small in 11 % and of some size in 6 % | |
Bailliart [11] | 1923 | 19 % | ||
Adachi [12] | 1928 | 8.7 % | ||
Bullwinkel [13] | 1954 | 16 % | On left side in 56 % | |
Bonamour and Gaillot [14] | 1956 | 15–20 % | ||
Collier [15] | 1957 | 21.6 % | Bilateral in 17 % | 1,000 subjects, most commonly in hypermetric astigmatism |
Mann [16] | 1957 | 25 % | ||
Blunt [17] | 1956 | None | In 76 eyes | |
Steele and Blunt [18] | 1956 | None | In 76 eyes | |
Mehra [19] | 1965 | 6.9 % | 1,448 subjects, bilateral in 1.1 %, unilateral in 5.8 % | |
Justice and Lehmann [20] | 1976 | 49.5 % | Bilateral in 14.6 % | Fluorescein angiographic study of 2,000 eyes of 1,000 patients |
Shihab et al. [21] | 1985 | 100 open-angle glaucoma patients | 44 eyes of 34 patients had one or more arteries | Studied 20 patients with unilateral arteries |
Mikelberg et al. [22] | 1990 | 33 % | Unilateral | In 33 patients with normal tension glaucoma |
Wang [23] | 1991 | 40.2 % | 1–6 arteries, supplying 1–4 quadrants of the retina | Fluorescein angiographic study of 2,050 eyes |
Lee and Schwartz [24] | 1992 | 38 % | One or two temporal cilioretinal arteries | Among 34 eyes with open-angle glaucoma |
Theodossiadis et al. [25] | 1992 | 64 % | 2 in 87.5 % | Fluorescein angiographic study in 25 cases with optic disc pit |
Nipken and Schmidt [26] | 1996 | 38.6 % | In 140 persons |
1.
It is common to see healthy eyes in which a cilioretinal artery on reaching the disc turns sharply back and disappears under the rim of the sclera, as if running into (or emerging from) the choroid.
2.
The cilioretinal artery is generally very small, but may be as large as one of the main divisions of the central retinal artery.
3.
They are always situated on the temporal side of the disc and pass to the foveal region of the retina.
4.
No practical significance can at present be attached to this peculiarity in the blood supply of the fovea of the retina.
5.
Such a vessel is generally present in only one eye, but it is occasionally seen in both. It is usually single, but may be two in the same eye.
6.
A cilioretinal artery can in most cases be readily distinguished from the other retinal arterial branches (generally of small size), which are often seen to enter (or emerge from) the optic nerve at various points between the temporal border and the physiological pit. In some cases when the vessel disappears very near to the border of the disc, it may be impossible to say whether it passes straight down the nerve or curves around the sclera.
7.
Anatomists do not agree as to whether those vessels, which disappear between the optic disc border and the physiological pit, are branches of the central retinal artery given off before reaching the eyeball or branches of the ciliary vessels.
8.
The cilioretinal arteries do not appear to anastomose with the other retinal vessels either on the retina or optic disc.
9.
The presence and size of the cilioretinal artery does not appear to bear any relation to disease. It often seems to taper off a little toward its point of submergence in the choroid or sclera, this appearance being explained in the same manner as the similar apparent tapering of the central retinal artery and vein in the physiological pit and not indicating any diminution in size.
He stated that this cilioretinal vessel may be either an artery or a vein. We now know that it is almost always an artery and only rarely a vein.
Like Nettleship [3], Lang and Barrett [6] in 1888 defined a cilioretinal vessel as “one which dips into the nerve near the margin of the optic disc and which can be seen to arch outwards,” and did not regard a vessel without this curve as cilioretinal. Jackson [9] stated that the artery curved as it emerged. This characteristic sharp hook-like appearance at its site of entry into the retina at the optic disc margin was described as a diagnostic feature of this artery by Salzmann [10] and Duke-Elder [28].
Salzmann [10] stated that a nasal cilioretinal artery was associated with anomalies of the optic disc. Collier [15] demonstrated an association of cilioretinal arteries with congenital anomalies of the optic disc and fundus and with refractive errors (he found ametropia in 195 eyes, of which 47 % were astigmatic; 40.2 % had hypermetropia, with or without astigmatism, and 32.5 % had myopia). Glees [29] suggested some genetic association between cilioretinal vessels and various abnormalities of the retinal vessels, cerebral angiomata, and aneurysms of the cranial vessels and stressed their value as diagnostic signs. Loring [4] stated that cilioretinal arteries were seen where the nutrition of the retina had suffered from morbid processes, but Nettleship [3] found no association with any disease. In my clinic, I have seen a cilioretinal artery as a common finding in normal eyes, with no evident association with any ocular disease.
Birnbacher [30] in 1887 rightly stated that every artery which appeared at or near the disc margin was not necessarily a cilioretinal artery. Duke-Elder and Wybar [31] described the division of the central retinal artery within the substance of the optic nerve into two, four, or even eight arteries, which emerged separately at the disc, no parent trunk being visible ophthalmoscopically. Blunt [17] found the central retinal artery bifurcating 0–4 mm behind the disc in one case, and one of the branches passed to the margin of the lamina cribrosa to emerge from the disc at the periphery. The condition described resembles somewhat the left side of my reported cases in a rhesus monkey [32]. Bloch [33] and Salzmann [10] saw patients with arteries at the periphery of the disc and no central artery. According to Parsons [34], this possibility cannot always be eliminated. Thus, rarely the artery that looks like the cilioretinal artery ophthalmoscopically may in reality be an early branch of the central retinal artery, arising within the optic nerve, and in such cases a normal central retinal artery would also be seen. In such cases, fluorescein fundus angiography is helpful, because normally the cilioretinal artery fills at the same time as the choroid and usually before the onset of filling of the central retinal artery or its branch (Fig. 3.2). On the other hand, if it is an early branch of the central retinal artery, the branch and the main central retinal artery fill simultaneously.
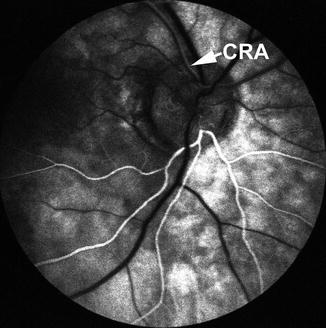
Fig. 3.2
Fluorescein fundus angiogram of right 13 s after the injection of fluorescein. It shows normal filling of the cilioretinal artery supplying the inferior half of the retina; it fills synchronously with the choroidal filling. The central retinal artery supplying the superior half of the retina has just started to fill
Anatomical Proof of the Presence of the Cilioretinal Artery
This is very rare in the literature. Anatomically this was shown by Müller [35] in one case, Nettleship [2] in one, Randall [5] in one, Birnbacher [30] in one, Fuchs [36] in five, Beauvieux and Ristitch [37] in one, and Wybar [38] in one. Only the last named followed the whole course of a cilioretinal artery in latex casts and conclusively proved that it arises from the posterior ciliary arteries, thus definitely proving it a cilioretinal artery. In my study of two eyes of a rhesus monkey, in serial sections of the optic nerve, I was also able to trace the arteries to their origin from the posterior ciliary arteries, showing them to be true cilioretinal arteries [32]. However, most previous authors have based their statistics and conclusions only on ophthalmoscopic appearances, but, as mentioned above, no absolute reliance can be placed on the ophthalmoscopic findings. Those who have based their observations on the ophthalmoscopic appearances have found the cilioretinal arteries to be very common, whereas a detailed anatomical examination of 72 eyes [17, 18] revealed no such artery (though such a negative observation is to be taken cautiously). Similarly, the anatomically based reports of the incidence of cilioretinal arteries in the rhesus monkey also seem to be low, because no example was found in about twenty eyes examined both ophthalmoscopically and either histologically or by latex injection [39].
Origin of Cilioretinal Arteries
In the literature, there is controversy about the origin of the cilioretinal arteries. According to Nettleship [3], these vessels were seen going to the choroid. Randall [5] found that most of them arose directly from the short posterior ciliary artery and passed through or around the edge of the choroid. Birnbacher [30] found one arising from the choroidal artery in a histological section, and similar formations were seen by others [7, 36, 40]. Elschnig [7] further stated that they might arise from an artery communicating with the circle of Haller and Zinn and with the choroid. Others [2, 11, 28, 36] stated that they usually arose from the circle of Haller and Zinn. According to Bailliart [11], they arose at times from the posterior ciliary artery and very rarely from the choroidal artery, but Elschnig [8] did not find one arising directly from the posterior ciliary artery. According to Parsons [34], they were mostly derived from the posterior ciliary arteries and not from the choroidal artery. In my study of two eyes of a rhesus monkey, I was also able to trace the cilioretinal arteries to their origin from the posterior ciliary arteries in serial sections of the optic nerve [32].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


