FIGURE 40.1 Exenteration defect following anterior skull base resection requiring a three-layer reconstruction.
HISTORY
In the taking of the history, it is important to note whether the patient has had prior craniotomy and if he or she has been treated with radiation in the past to the anterior cranial fossa. This is not an uncommon experience in patients with recurrent meningioma or a patient with a prior history of surgery and radiation for cancer of the ethmoid or maxillary sinus with intracranial penetration. The past history of a frontal craniotomy makes the harvest of a pericranial flap at this site extremely difficult and sometimes impossible.
A history of prior irradiation will jeopardize not only the survival of the flap but also the viability of the underlying cranial bone. The use of some form of free vascularized tissue to line the subcranial cavity is often mandated in these cases to establish a good blood supply to these compromised tissues.
PHYSICAL EXAMINATION
Examination of the defect will determine if the pericranial flap is the appropriate donor site. The blood supply to the flap should be evaluated to assure that it is intact and that the flap is well vascularized. There should be no evidence of prior surgery, trauma, or radiation to the donor site. The width of the flap should be wider than the expected cranial floor defect. Finally, before beginning the flap reconstruction, the dural reconstruction should be examined to assure that it is watertight to decrease the potential for CSF leakage.
INDICATIONS
The pericranial flap is indicated for central defects of the skull base.
CONTRAINDICATIONS
Contraindications to the pericranial flap include when the flap vascularity has been compromised by injury to the blood supply or in some previously radiated patients, the flap may not be hearty.
PREOPERATIVE PLANNING
Unless a prior craniotomy has been performed, there is little preoperative planning. If a prior craniotomy has been performed and the pericranial flap has been previously used for a reconstruction of the central skull base, I prepare for the possibility of a free flap for reconstruction. A free flap reconstruction is the only alternative because a temporalis flap will not reach the midline.
SURGICAL TECHNIQUE
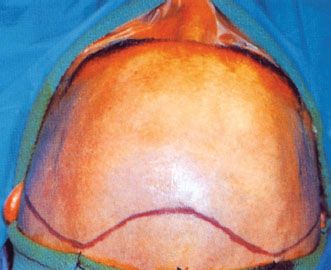
Under general anesthesia, the patient usually has a tracheostomy done, to prevent postoperative tension pneumocephalus, and the head is place in a padded Mayfield headrest. The anterior aspect of the hair is usually shaved in order to prevent hairs from prolapsing into the wound at the time of closure at the end of the procedure. The scalp incision is outlined in methylene blue in a curvilinear fashion from the anterior–superior aspect of the auricle over the vertex of the skull running about 2 cm behind the hairline to the opposite side (Fig. 40.2). Injection of the scalp along the incision line is then done with a solution of ½% Xylocaine with 1 in 20,000 epinephrine.
The coronal scalp incision is then made with a scalpel usually one side at a time, taking great care to avoid incising the pericranium. Periodic gentle blunt elevation in the depths of the incision with the back of the scalpel handle will allow easy identification of the area of the pericranium. Hemostasis is secured along the edges of the scalp incision by the placement of Raney clips and the use of the bipolar cautery. The elevation of the scalp flap proceeds toward the brows taking care not to make holes in the underlying pericranium. As the more posterior elevation of the flap proceeds over the temporalis muscle, care is taken to incise a semilunar portion of superficial temporal fascia keeping it attached to the scalp (Fig. 40.3). This will protect the temporal branch of the facial nerve as the flap elevation proceeds anteroinferiorly.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


