The allergic march is a progression of atopic disease from eczema to asthma, and then to allergic rhinoconjunctivitis. It appears to be caused by a regional allergic response with breakdown of the local epithelial barrier that initiates systemic allergic inflammation. Genetic and environmental factors predispose to developing the allergic march. There are data to support 4 possible interventions to prevent the allergic march from progressing to asthma: (1) supplements of dietary probiotics, (2) exclusive breast feeding during the first few months of life, or, alternatively (3) use of extensively hydrolyzed infant formulas, (4) treatment with inhalant allergen immunotherapy by either subcutaneous or sublingual methods.
A common question, often asked by both parents and by physicians, is: will this child develop asthma? The follow-up question is: if asthma is likely, how can it be prevented? Until very recently, it was impossible to give a precise answer to either query, but increasing knowledge of the allergic (or atopic) march has now made it possible to give partial answers to both. The goals of this article are to explain the allergic march concept, review the available evidence, describe attempts to prevent the march, and, finally, outline possible intervention options for allergists and parents.
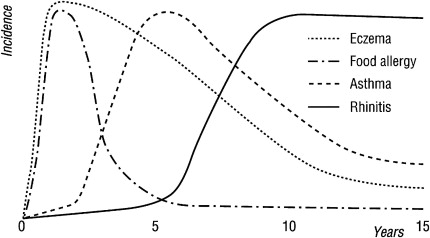
The allergic march is a postulated progression of atopic disease in infants with eczema to subsequently develop asthma, and then allergic rhinoconjunctivitis. The march was identified by many clinical observations during the 20th century, yet the first meta-analysis of this subject was prepared just 11 years ago. In this article, Catani summarized the available information on age of onset for allergic diseases. Eczema begins in the first year of life in 80% of children, with specific food allergies detected: cow’s milk allergy in 73%, egg allergy in 71%, and fish allergy in 51%. Asthma has a later onset, with only 42% evident in the first year, and 49% in the second year, but 92% develop symptoms before age 8. Rhinoconjunctivitis occurs even later, with 35% in year 1, and only 59% by age 5. The march can be visualized graphically ( Fig. 1 ). Evidence for developing food allergies generally occurs synchronously with signs and symptoms of eczema, and, in most allergic children, both precede respiratory symptoms.
Evidence for the allergic march
Clinical observations of the eczema-to-asthma-to-rhinitis progression were originally from cross-sectional studies that are subject to recall bias. Birth cohort studies have recently been done, and generally confirm the march concept. But, the initial idea of a uniform progression, in all patients, from eczema to asthma, has not been confirmed. At least 3 clinical variants occur: (1) a normal allergic march from eczema to asthma to rhinitis, (2) a reverse allergic march from asthma to eczema, (3) and a purely respiratory allergic march of rhinitis to asthma, without any eczema. The allergic march also is not restricted to children, but can occur at any age. The relative risks for eczema progressing to asthma and rhinoconjunctivitis have been calculated for 250 infant eczema patients, followed for as long as 22 years. Incidences of both asthma and rhinoconjunctivitis rise steadily with age, and by age 18, 34% develop asthma, and 66% rhinoconjunctivitis, while eczema declines to 42%. The severity of eczema is proportional to the risk of developing asthma, with the most severe eczema cases having 4.8 times the risk of mild cases ( P = .001). The risk of developing rhinoconjunctivitis is similarly increased 3.2 times by prior development of asthma in these children.
Risk factors for developing asthma
In a systematic review of 26 eczema follow-up studies from 1950 to 2006, about 30% of all eczema patients develop asthma by age 6, and those eczema patients who are atopic are much more likely to develop asthma. For example, children with eczema and early wheezing but no atopy (defined by no positive allergy tests) have a lower risk of later asthma (odds ratio [OR] 2.84), compared with similar patients who are allergen sensitized (OR 6.68). Infant wheezing is also a risk for adult asthma. Fifty-nine patients who wheezed before age 2 were re-evaluated at age 26 to 29, and 41% had asthma versus 10% of controls (OR 13.3). Family history is significant, since the presence of sibling asthma increases asthma risk (OR 5.68). In addition to the effects of atopic status and family history, in children of all ages, food allergy is an independent risk for asthma. Severe or multiple food allergies further increase the risk.
Risk factors for developing asthma
In a systematic review of 26 eczema follow-up studies from 1950 to 2006, about 30% of all eczema patients develop asthma by age 6, and those eczema patients who are atopic are much more likely to develop asthma. For example, children with eczema and early wheezing but no atopy (defined by no positive allergy tests) have a lower risk of later asthma (odds ratio [OR] 2.84), compared with similar patients who are allergen sensitized (OR 6.68). Infant wheezing is also a risk for adult asthma. Fifty-nine patients who wheezed before age 2 were re-evaluated at age 26 to 29, and 41% had asthma versus 10% of controls (OR 13.3). Family history is significant, since the presence of sibling asthma increases asthma risk (OR 5.68). In addition to the effects of atopic status and family history, in children of all ages, food allergy is an independent risk for asthma. Severe or multiple food allergies further increase the risk.
Allergic march variations
A reverse allergic march has been reported by Canonica and Passalacqua’s group, in a study of 692 child asthmatics without either food allergy or eczema. During the 9-year follow-up, 20% developed eczema. Mite monosensitization was more common in those who developed eczema.
Settipane made the first clinical observations of a purely respiratory allergic march in a 23-year follow-up of 738 atopics who had no eczema and were allergy tested as college students. The incidence of both allergic rhinitis and asthma continued to increase with age in these patients. Similar to eczema patients, positive allergy tests were a risk factor for asthma development ( P = .001), but in addition, so was the presence of allergic rhinitis ( P = .002). Two other long-term studies, a 20-year follow-up of 252 infant eczema patients, and a 40-year follow-up of 2100 adult rhinitis patients, have confirmed that allergic rhinitis is an independent risk factor for developing asthma (independent of eczema). A recent 467-member birth cohort study has also confirmed, using Allergic Rhinitis and its Impact on Asthma (ARIA) criteria, that at least to age 13, the prevalence of allergic rhinitis continues to increase, and there is a clear genetic risk component. In this cohort, symptomatic allergic rhinitis occurs in 44% of patients with at least 1 allergic parent versus 24% with no parental allergy.
The last variation of the allergic march is possible sex specificity. A surprising finding of a large birth cohort study of children with an atopic family history, studied from birth to age 7, was that eczema in the first 2 years predicts asthma in boys (OR 2.45), but not girls (OR 0.88). There were no changes in the conclusions if the data were adjusted for early allergy sensitization or wheezing, and these results remain unexplained.
Role of food allergens in triggering the allergic march
The average age of sensitization to various allergens varies substantially, and this has a bearing both on which allergens are more likely to trigger the allergic march, and where preventative measures should be focused. Egg and milk food allergies are among the very first allergies to appear, often before 12 months, while sensitivity to other staple foods usually begins in the second year, and does not reach the same prevalence level until around age 5. Sensitivity to indoor inhaled allergens (mites and animals) also is rare before age 2, and increases thereafter similarly to staple foods. Sensitivity to outdoor pollen allergens also is rare before age 2, and increases markedly only after age 3. As a result of these data, both egg and milk allergy have been scrutinized closely for possible roles as allergic march and asthma triggers. A subgroup of allergic rhinitis patients has been found to have food allergy-mediated rhinitis. In one study, open oral food challenge positive, cow’s milk allergic infants, who had only rhinitis and no positive inhalant tests, were followed from age 1 to 5 years. During this time, milk allergy decreased from 100% to 14%, while asthma increased from 0% to 72%, identifying another large asthma risk factor. Ricci and colleagues similarly identified a very strong risk for later asthma and allergic rhinitis associated with early sensitization to eggs.
Independent risk factors for developing asthma are therefore: early eczema, eczema severity, atopy (allergic sensitization), early persisting wheezing, allergic rhinitis, male sex, and food allergy, especially allergy to cow’s milk and chicken’s egg.
Relationship of environmental and genetic factors to eczema prevalence
National eczema prevalences range from 0.3% to 20.5%, are highest in Scandinavia, Canada, Australia, Chile, and the United States, and lowest in the tropics and Russia. Eczema is increasing in 70% of nations, where the prevalence correlates directly with national per capita income. The very rapid rate of change in eczema prevalence strongly suggests environmental, rather than purely genetic, factors are involved. There is also good evidence for genetic influence, since atopic children are much more likely to develop eczema than nonatopics. This genetic influence is seen most strongly in affluent nations, where many eczema cases are positively correlated to atopy (OR 2.69). However, only in 15% of poor nations is correlation with atopy found, which supports the existence of environmental influences on eczema, influences that vary with economic status. One possible explanation for the difference in eczema cases seen in different nations can be inferred from longitudinal studies in locales that are undergoing urbanization, such as in Africa. There, atopy is increasing everywhere with national income level. In South African cities, the rise in atopy correlates both with assuming an urban, Western diet, and with less exposure to infections. Several environmental factors have now been postulated to be affecting eczema and the allergic march, including the hygiene hypothesis, vitamin D levels, maternal nutrition, infant feeding practices, chemical pollution, and antibiotic and anti-inflammatory drugs.
Hygiene hypothesis
This is the most frequently considered hypothesis to explain historic increases in atopic diseases during 20th century, including the allergic march. Newborns have a predominately Th2, allergic immune response, and acquire Th1 responses by infection exposures. Environmental changes have been dramatic in the 20th century: small families, cleaner, almost entirely indoor living, processed and sanitized foods with chemical additives, infection prevention and antibiotic treatments, and world-wide pollution. These changes either directly reduce exposure to pathogens, or can alter immune functioning, so the hygiene hypothesis posited that these environmental influences caused a shift in the balance between Th1- and Th2-mediated immunity to favor a continued allergic, Th2 state, rather than the development of a normal balance between Th1 and Th2 responses.
This simple paradigm is not entirely correct, because
Th2 responses to parasitic infestations protect from allergies
Th1 autoimmune diseases are increasing at the same time allergies are
Both Th1 and Th2 diseases may occur in the same patients
High-dose exposures to allergens that generate a Th2 response can cause tolerance, rather than sensitization.
Furthermore, at the time the hygiene hypothesis was first proposed, the full extent of the T-cell network was not known, including the existence of Th17, a third class of CD4+ helper T-lymphocytes, and Treg, a class of regulatory T- lymphocytes. In light of these points, a modified hygiene hypothesis has been proposed: that the modern increase in allergic diseases is due to an imbalanced, misregulated, or inappropriate T-cell response, which leads to excessive immune stimulation from Th1, Th2, and/or Th17 classes of T helper cells.
Evidence for the hygiene hypothesis
One of the observations providing strong support for the hygiene hypothesis is that farm life protects from atopy, allergic rhinitis, and asthma, either when infants or their pregnant mothers are exposed to farm living. When farm children are compared with carefully matched controls, early exposure (under 1 year) or prolonged exposure (until age 5) is strongly protective. Key antiallergy factors are exposure to stables and drinking unpasteurized milk. Mothers living on a farm have significantly higher levels of the cytokines transforming growth factor beta (TGF-β) and interleukin (IL)-10 ( P = .05 for both) in their colostrum and mature milk, compared with control nonfarm rural mothers. TGF-β helps establish innate immunity, and IL-10 has broad antiallergic activity, which may influence the infant’s immune balance away from allergy.
A second area of support for the hygiene hypothesis comes from the effects of early life infections. Attending group daycare or having many older siblings reduces the risk of developing atopy or asthma, presumably because of increased infections. The role of specific viruses is not as clear, since, in some reports, certain viruses protect, but human rhinoviruses and respiratory syncytial virus normally initiate or aggravate asthma. In a birth cohort study, infections (colds, diarrhea with fever, or any fever) in the first 3 months of life increased wheezing risk by age 2 years.
Intestinal flora and infections have also been studied. Early oro–fecal exposure, as measured by exposure to hepatitis A, toxoplasmosis, or parasite infestations, protects from asthma, as does administration of many types of probiotic bacteria. Reducing gut levels of lactobacilli and bifidobacteria (eg, by antibiotic use) increases the risk, as does abnormal intestinal microbial balance, for example, when pathogenic bacteria like Clostridium difficile predominate. Neonatal antibiotic use is statistically correlated with later asthma, and there is a dose effect, with more courses of antibiotics increasing asthma risk, but the overall increase in risk, in 1 study, is only about 15%.
A final group of supportive studies involves birth-related infections. Elective cesarian section decreases asthma risk (OR 0.34), and a lengthy time of ruptured membranes (>3 hours) before delivery increases asthma risk (OR 6.7). These reports are believed to be due to varying degrees of infant exposure to vaginal flora, including Ureaplasma and staphylococci, which are known to be associated with subsequent asthma development.
A meta-analysis of 46 papers reporting the effects of early life exposures on the risk of triggering the allergic march has been done. Exposure to pets (n = 27) slightly reduces risk, dog exposure being better than cat (OR 0.84, confidence interval [CI]: 0.73–0.96). Exposure to endotoxin (n = 13) slightly reduces risk, (OR 0.90 CI: 0.78–1.0). Drinking unpasteurized milk (n = 7) reduces risk (OR 0.68 CI: 0.61–0.76). Finally, livestock exposure (n = 8) produces a sizable risk reduction, (OR 0.58 CI: 0.39–0.87). Tse and Horner believe, based on their studies, that normal levels of respiratory exposure to a variety of allergens found in house dusts are naturally tolerogenic. But, intermittent high exposures can break through this normal tolerance, to cause symptomatic allergic disease.
Effects of vitamin D on the allergic march
Vitamin D has broad immune effects, since vitamin D receptors are present in the nucleus of B- and T-lymphocytes, monocytes, macrophages, and dendritic cells, where vitamin D modulates cytokine levels, including thymic stromal lymphopoetin (TSLP), IL-2, 4, 5, and 13, interferon gamma (IFN-γ), and many others. Vitamin D deficiency increases infections, all allergic diseases, and autoimmunity risk. The effects on allergy depend on both vitamin D dose and patient age. Vitamin D supplements may have a steroid-sparing effect in asthma, and high levels are associated with better lung function. High maternal vitamin D is associated with less wheezing in those mother’s children, but, there is evidence that the dose–response curve may be U-shaped, so that both low and very high vitamin D levels may increase allergy risk.
Vitamin D should benefit eczema because of its known biologic effects of increasing keratinocyte proliferation, promotion of wound healing, stimulation of skin antimicrobial canthelicidins, and suppression of skin inflammation. In a small study, vitamin D supplements improved winter eczema.
Effects of maternal nutrition on the allergic march
Three recent reports agree that insufficient maternal nutrition during pregnancy increases the risk for children to develop allergies, eczema, and asthma. The studies focused on different aspects of nutrition, but found that increased maternal zinc and antioxidant intake are protective, and that vitamin E, citrus fruits, and green and yellow vegetables are possibly protective.
Effects of chemical pollution on the allergic march
Chemical pollutants are associated with increased risk of both atopy and asthma. Respiratory exposure to natural gas cooking fumes and tobacco smoking both increase only asthma, while traffic exhaust increases eczema, asthma, and rhinitis. In a prenatal birth cohort study, the active fractions in traffic pollution were identified as polyaromatic cyclic hydrocarbons (PAH) and ultrafine particulates, and both maternal prenatal and infant postnatal exposure were found to be important. Traffic exhaust may injure the lung surface barrier, increasing pulmonary sensitization.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


