The Aging Neck
Edwin Francis Williams
Henry Haipei Chen
The typical appearance of the aging neck is caused by a constellation of changes associated with both heredity and the aging process. Each patient will demonstrate different anatomic components contributing to the overall appearance of an aging neckline. The anatomic factors that contribute to an ideal cervical contour include a strong chin, a distinct mandibular border, a cervicomental angle of 105 to 120 degrees, a visible subhyoid bone depression, a gentle indentation at the thyroid notch, and visible anterior borders of the sternocleidomastoid muscles (1) (Fig. 189.1). Obtaining these ideal contours should be the goal of any surgical correction of the aging neck. To achieve these goals, however, the surgeon must carefully and systematically analyze each patient to determine the anatomic abnormalities that need to be addressed. An individualized approach ensures that specific deformities are clearly delineated so a youthful and graceful neckline may be restored.
ANATOMY
The aging process exerts an impact on each anatomic element of the cervical region to varying degrees in each patient. Additionally, some patients also display hereditary abnormalities contributing to an unfavorable cervical contour, including a low-positioned hyoid bone, poor chin projection, and a congenital collection of submental fat. Each element of the contributing anatomy should be identified preoperatively and sequentially addressed in the surgical correction to provide an optimal aesthetic outcome. The anatomic areas to be addressed include skin, fat, platysma muscle, chin position, and other unfavorable anatomy (2).
Skin
With time, collagen and elastin fibers degenerate so the overlying skin loses its tone and no longer adheres to the soft tissue contours of the neck. The skin becomes redundant and sags, leading to the development of horizontal cervical rhytids and effacement of the cervicomental angle.
Fat
Fat deposition in the neck can be congenital or acquired. Several anatomic studies have shown that the fat in the submental region is found in discrete compartments (3,4). These areas include (a) a supraplatysmal (subcutaneous) layer diffusely distributed throughout the cervical region, (b) a subplatysmal compartment that overlies the mylohyoid muscle, and (c) facial fat from the cheek and inferior buccal fat pad contributing to a ptotic jowl and loss of the definition of the inferior mandibular border (Fig. 189.2). The subplatysmal layer is further divided into a central compartment between the anterior bellies of the digastric muscles and paired medial and lateral compartments.
Clinically, it is difficult to discern the exact anatomic compartment(s) of submental lipodystrophy, especially in heavy necks. While the use of ultrasonography can be helpful to delineate the areas of excess fat (5), its use is certainly not required as a part of a routine preoperative workup.
Platysma Muscle
The platysma is a paired muscle that is innervated by the cervical branch of the seventh cranial nerve. It originates from the fascia of the pectoralis major and deltoid muscles and ascends in the neck to insert on the inferior border of the mandible (Fig. 189.3). Laterally, the posterior border of the platysma muscle ends in front of the sternocleidomastoid muscle. As the platysma muscle is followed superiorly to the mandible, the medial fibers insert into the periosteum to stabilize one end of the muscle during contraction. The central fibers blend intimately with the risorius muscle. The posterior third of the platysma muscle
sweeps up over the mandible to course anteriorly and fuse with the superficial musculoaponeurotic system (SMAS). The cervical skin receives part of its blood supply from perforating vessels arising from the platysma muscle. These vessels and thick fibrous septa coursing through the subcutaneous fat anchor the dermis to the superficial cervical fascia and platysma muscle.
sweeps up over the mandible to course anteriorly and fuse with the superficial musculoaponeurotic system (SMAS). The cervical skin receives part of its blood supply from perforating vessels arising from the platysma muscle. These vessels and thick fibrous septa coursing through the subcutaneous fat anchor the dermis to the superficial cervical fascia and platysma muscle.
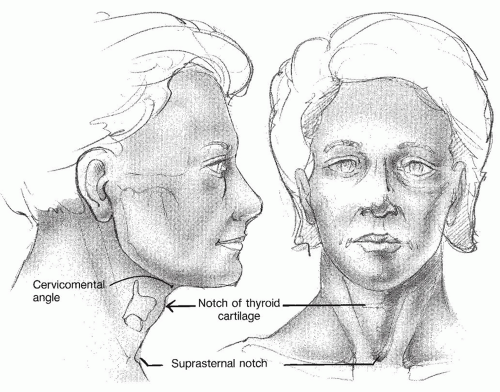 Figure 189.1 The anatomic factors that contribute to an ideal cervical contour include a strong chin, a distinct mandibular border, a cervicomental angle of 90 degrees, a visible subhyoid bone depression, a gentle indentation at the thyroid notch, and visible anterior borders of the sternocleidomastoid muscles. |
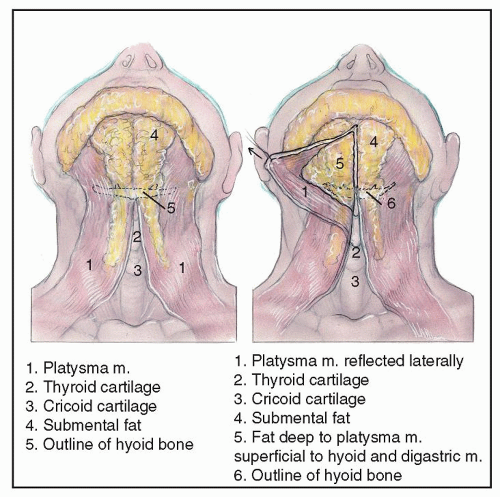 Figure 189.2 Fat is found both superficial and deep to the platysma. |
Different degrees of decussation in the midline of the neck have been documented in anatomic studies, and there is also ethnic variability (6,7). The “turkey gobbler” deformity is caused by a laxity in the platysma muscle that does not decussate in the midline.
The platysma muscle functions to stabilize the chest muscles against the jaw during heavy lifting. It also provides a layer over vital structures of the neck. It is a somewhat vestigial structure in humans, corresponding phylogenetically to the panniculus carnosus muscle that forms a continuous subcutaneous layer in lower mammals (8).
With aging, the platysma muscle becomes atrophic and falls toward the midline. First, convexity occurs in the submental region; then, as the muscle loses tone, it forms the pathognomonic anterior banding of the aged neck. On profile, the apex of the cervicomental angle is blunted by the anterior border of the muscle as it runs diagonally from the mandible to the lower neck. Loss of the platysmal muscle sling also allows ptosis of the underlying cervical contents.
Chin Position
An appropriately projected chin is prerequisite for an optimal aesthetic cervical contour. A poorly projected chin creates an illusion of blunting of the cervicomental angle, and aging contour deformities tend to be worse in patients with smaller mandibles and chins (9,10).
Ideally, in a patient with Angle class I occlusion, the pogonion (the most anterior projecting point of the chin) should touch a line dropped vertically from the vermillion border of the lower lip on profile view. It is aesthetically acceptable in women if the chin is slightly posterior to this
line; however, in men, this line should be tangent to the pogonion (11) (Fig. 189.4). The chin contour is determined by the shape and position of the mandible as well as the overlying soft tissues. A weak chin, or microgenia, is most commonly congenital; however, senile absorption of alveolar bone should also be considered in the older patient.
line; however, in men, this line should be tangent to the pogonion (11) (Fig. 189.4). The chin contour is determined by the shape and position of the mandible as well as the overlying soft tissues. A weak chin, or microgenia, is most commonly congenital; however, senile absorption of alveolar bone should also be considered in the older patient.
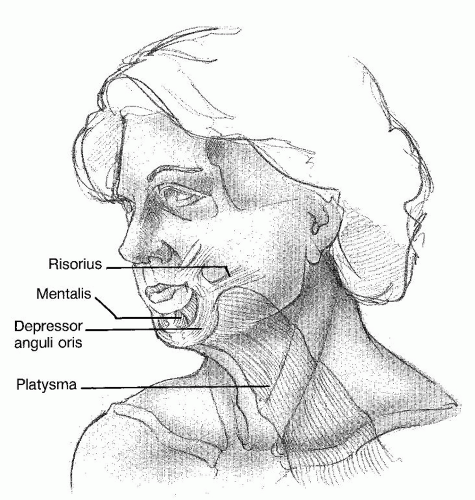 Figure 189.3 The platysma muscle ascends in the neck to blend with the SMAS. |
Mandibular hypoplasia is an acquired condition secondary to varying degrees of bony resorption of the mandible. With aging, specific progressive soft tissue atrophy and bone reduction occur in the region between the chin and jowl. This resulting groove has been termed the “prejowl sulcus” (11). Mandibular hypoplasia should not be confused with retrognathia. Patients with retrognathia demonstrate Angle class II occlusion and are optimally treated with a bony advancement technique (e.g., sagittal-split osteotomy), whereas patients with microgenia or mandibular hypoplasia are better treated with alloplastic augmentation.
Unfavorable Anatomy
The hyoid bone supports the floor of the mouth as it is suspended by the digastric, mylohyoid, stylohyoid, and tongue musculature. Ideally, it should be at the level of the third or fourth cervical vertebrae (12). A more posterior and superior hyoid produces a more aesthetic cervical contour. A hyoid bone that is in a relatively inferior position in the neck causes the suprahyoid musculature to course in a more vertical direction, blunting the angle between the chin and neck (13). With advancing age, gravity may favor the drag of the infrahyoid musculature over the suprahyoid musculature, inducing further descent of the hyoid (12). A low hyoid bone position is a major limiting factor in the optimal rejuvenation of the cervical region.
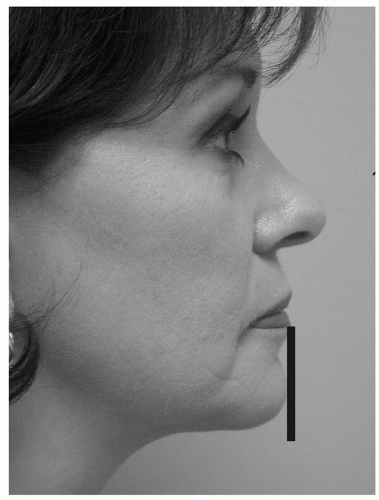 Figure 189.4 The anteriormost projection of the chin (pogonion) should touch a line dropped vertically from the vermillion border of the lower lip on profile view. |
Submandibular gland ptosis is commonly seen with aging, which is identified as two bulges at the anterior edge of the submandibular triangle. Diagnosis is confirmed by palpation of the gland’s cobblestoned surface. The position of the glands should be elucidated preoperatively for both patient counseling and surgical planning.
Overdevelopment of the suprahyoid bone musculature, especially the digastric muscles, can also lead to fullness of the submental region. Identification is facilitated by having the patient flex the neck with the mouth closed (2).
CLASSIFICATION AND EVALUATION
Numerous classification schemes describing the aging neck exist (2,14,15). Dedo’s (14) preoperative classification of the neck is the most commonly used. It is a useful tool to help delineate the features contributing to a particular patient’s pathology and to help guide targeted surgical intervention (Fig. 189.5).
A patient with a class I neck is typically a younger patient who has minimal, if any, deformity, which may or may not require surgical intervention. A patient with a
class I neck should ideally wait until more of an aesthetic problem develops, because any intervention at this time is essentially prophylactic.
class I neck should ideally wait until more of an aesthetic problem develops, because any intervention at this time is essentially prophylactic.
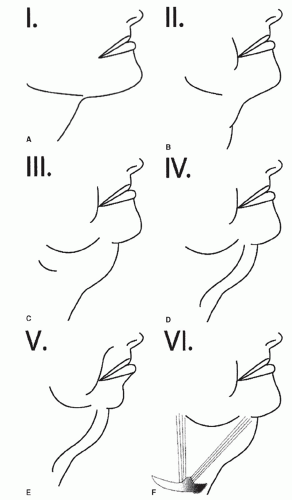 Figure 189.5 Dedo classification of cervical abnormalities: A: Class I deformity describes only minimal cosmetic deformity. B: Class II deformity describes only skin laxity. C: Class III deformity refers to the excessive submandibular and submental adipose. D: Class IV deformity refers to anterior banding of the platysma. E: Class V deformity describes the condition of microgenia or retrognathia. F: Class VI deformity describes a low-positioned hyoid bone. |
The class II patient has skin laxity only, without significant fat or muscle pathology. The class includes the “turkey gobbler” deformity often seen in elderly males.
A class III deformity is caused by excessive cervical liposis. Excess adipose can accumulate in the supra- or subplatysmal layer. Both contribute to jowling.
The class IV patient has a pathologic platysma muscle either in repose or on voluntary contraction. This is usually diagnosed in the thin neck as anterior platysmal banding; however, in patients with submental adiposity or redundant anterior cervical skin, it is often not readily apparent that the platysma muscle is contributing to the deformity. In fact, the full neck does not evidence platysmal banding, even with aging (3




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
