The Aging Forehead
Kian Karimi
Peter A. Adamson
Addressing the upper third of the face is an important component of facial rejuvenation. For many patients, descent of the eyebrows leads to exacerbation of periocular aging, which is inadequately treated with blepharoplasty. Without correction of eyebrow ptosis, the aging face often conveys fatigue and even anger. Forehead rejuvenation procedures have been utilized with increasing frequency over the last several decades. The forehead lift, or the “facelift of the upper third,” is an essential tool in providing a harmonious rejuvenation in patients.
HISTORY
As examined in a recent review by Matros et al. (1), changes in eyebrow position and shape with aging have been described and refined for the past four decades. Some of the earliest descriptions of brow lifting date back to 1919 as described by Passot, Hunt, and Lexer (2). Vinas is credited for noting the difference between static and dynamic rhytids and importantly recognized that treatment would differ between the two types, including the necessity to free adhesions over the orbital rims to mobilize and elevate the brows. An important development in brow lifting occurred in 1992 with the first description of the endoscopic technique (3). Despite multiple modifications of the brow lift trending toward less invasive approaches purporting lower complication rates and higher patient acceptability, a recent review by Cilento and Johnson of over 1,000 coronal or trichophytic brow lifts demonstrated extremely high rates of patient satisfaction with an acceptably low complication rate including no permanent motor nerve dysfunction.
FOREHEAD ANATOMY
The forehead represents the upper third of the face and can be divided into vertical fifths as well, yielding five aesthetic subunits: the central forehead, lateral temporal units, and the brows. The lower anatomic boundaries include the supraorbital rim, nasal root, and bony zygomatic arches. The supraorbital rim is usually the landmark by which brow ptosis is measured. The trichion and natural hairlines represent the upper limit. Perhaps the most important division of forehead anatomy lies on either side of the temporal line, which divides the temporal regions from the forehead and intersects with the peak of the brow in both men and women.
Branches of the external and internal carotid arteries provide the blood supply to the forehead. The external carotid artery provides the superficial temporal artery and subsequent zygomaticotemporal branch, which supply the temple region and lateral forehead. The internal carotid artery supplies the midforehead via branches of the ophthalmic artery, the supratrochlear artery medially, and the supraorbital artery laterally, typically 2.5 cm lateral to the midline (Fig. 185.1).
Sensation is provided by the supraorbital and supratrochlear nerves, which are branches of the trigeminal nerve (V). The supratrochlear nerve exits the orbit, alongside the artery, and travels through the medial corrugator supercilii, providing sensation to the medial forehead. The supraorbital nerve exits the superior orbit through a foramen along the rim in nearly 90% of patients but can also exit the orbit through a foramen up to 1.5 cm above the orbital rim (4). Laterally, sensation is provided by the lacrimal (V1), zygomaticofacial (V2), and auriculotemporal (V3) nerves. Motor innervation is provided exclusively by the notoriously fragile temporal branch of the facial nerve.
The temporal branch exits the parotid gland and courses superiorly from a point 1.5 cm below the external auditory canal, crosses the zygomatic arch approximately 2.5 cm (0.8- to 3.5-cm range) anterior to the auditory canal, and runs superomedially toward the frontalis muscle but remains 2 cm posterior to the lateral bony orbital rim. This nerve can be reliably predicted by its relation to what
is known as the cephalic or “sentinel vein,” running just superficial to this vessel. The temporal branch remains just deep to the temporoparietal fascia and runs within the substance of this fascia, which is continuous with the superficial musculo-aponeurotic system (SMAS) inferiorly.
is known as the cephalic or “sentinel vein,” running just superficial to this vessel. The temporal branch remains just deep to the temporoparietal fascia and runs within the substance of this fascia, which is continuous with the superficial musculo-aponeurotic system (SMAS) inferiorly.
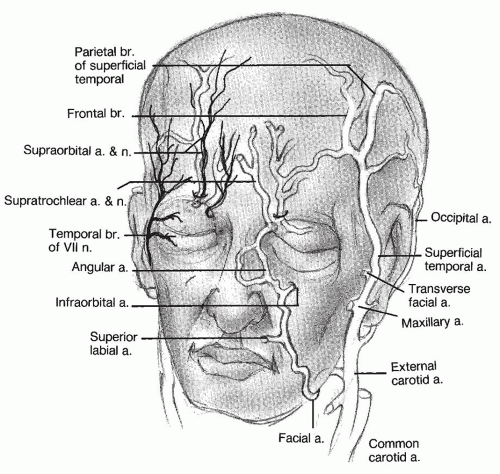 Figure 185.1 Vessels and nerves of the forehead. The major arterial and sensory innervation is through the supraorbital vessels and nerves. They arise about 2.5 cm from the midline. The temporal branch of the facial nerve is the most functionally significant. |
The forehead is an extension of the scalp and thus consists of the same layers, which, from superficial to deep, are the skin, subcutaneous tissues, galea and frontalis muscles, loose supraperiosteal areolar tissue, and pericranium (Fig. 185.2). The galea separates along the superior origin of the frontalis muscle, which divides the galea into superficial and deep layers. The posterior galea is in the same plane as the superior orbital septum. Lateral eyebrow ptosis has been described to be further exacerbated by a ptotic “galeal fat pad,” which is usually fully enveloped by the deep galeal fascia but may be dehiscent in some individuals, accelerating lateral brow ptosis (4). Laterally, the galeal layer is contiguous with the superficial temporal parietal fascia, both of which fuse at the zygomatic arch. The loose subgaleal and subtemporal parietal fascial layers allow for free mobility of the galea, facilitating facial expression.
The frontalis muscle is the primary elevator of the brow and is the most significant contributor to horizontal forehead rhytids. Inferiorly, the frontalis interdigitates with the orbicularis oculi muscle, the skin of the eyebrows, and the root of the nose (Fig. 185.3). The frontalis muscle also blends with the corrugator supercilii and procerus muscles medially. The corrugator supercilius muscle, also known as the “muscle of grief,” is the only muscle of facial expression to arise from bone. After originating from the medial aspect of the supraorbital arch, it passes obliquely, deep to the frontalis and orbicularis muscles, to insert by interdigitation with these muscles throughout the medial half of the eyebrow, causing characteristic vertical and oblique rhytids. The unpaired procerus muscle is pyramid shaped and arises from the fascia over the nasal bone and upper
lateral cartilages of the nose and inserts in the skin between the eyebrows, producing horizontal glabellar rhytids. The orbicularis oculi muscle also serves as a brow depressor. The depressor supercilii muscles are a minor contributor to brow depression.
lateral cartilages of the nose and inserts in the skin between the eyebrows, producing horizontal glabellar rhytids. The orbicularis oculi muscle also serves as a brow depressor. The depressor supercilii muscles are a minor contributor to brow depression.
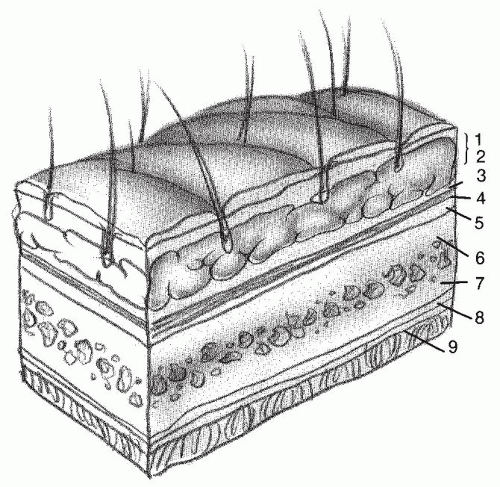 Figure 185.2 Forehead skin. “SCALP” refers to the layers of the forehead skin. 1, Skin; 2, subcutaneous tissue; 3, epicranial aponeurosis (galea and frontalis m.); 4, lax areolar tissue; 5, pericranium; 6, outer table; 7, inner table; 8, dura mater; 9, arachnoid. |
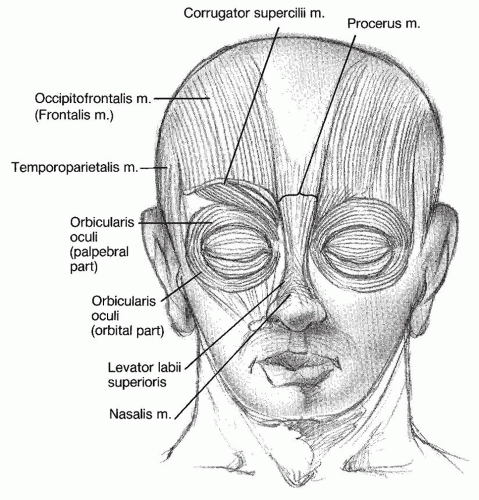 Figure 185.3 Forehead muscles. Forehead muscle activity causes the development of the rhytids associated with aging. The frontalis muscle produces horizontal forehead rhytids, the corrugator supercilius muscle vertical glabellar rhytids, and the procerus muscle horizontal glabellar rhytids. |
In a discussion of anatomic structures that contribute to the upper face aging process, it has been recognized that superficial temporal fascia “instability” plays a role in lateral brow ptosis due to its weak adhesion between the superficial and deep temporal fascial planes, with the sole support of the superficial fascial plane being its attachment to the frontal bone along the rim of the temporal fossa in the “zone of adhesion” and a loose attachment to the superior-lateral orbital rim called the “orbital ligament,” thought to represent a condensation of the superficial temporal fascia (4). It is also postulated that paucity of frontalis insertion laterally, and the stabilizing forces provided by the supraorbital and supratrochlear neurovascular bundles, explain why lateral eyebrow ptosis occurs to a far greater degree than medial or midbrow ptosis.
PHYSIOLOGY OF AGING
In youth, the forehead, temple, and glabella are unfurrowed. The hairline is irregularly irregular, and there is no evidence of male-pattern baldness or thinning hair in women. The transition between the thicker infrabrow skin and upper eyelid skin is of particular importance. In youth, the higher brow position allows for a well-demarcated contour of the lateral supraorbital rim above and an obvious upper eyelid fold.
With aging, the upper third of the face undertakes multiple changes (Fig. 185.4). The corrugator supercilius muscle may be the initiating factor to the aging process of the upper face by producing vertical and oblique glabellar skin lines through its transverse and oblique fibers, respectively (4). It is the interdigitation of the corrugator with the orbicularis, procerus, and depressor supercilii muscles that further causes medial eyebrow depression and glabellar rhytids. As the skin weakens over time and becomes less elastic, these rhytids become permanent. Additionally, loss of subcutaneous tissue and increased skull bone resorption is noted. Descent of the lateral third of the brow (lateral to the deep temporal fusion line) is discussed previously in this chapter. A visual field defect can result in advanced cases of lateral eyebrow ptosis, especially when compounded with upper eyelid ptosis. This “closed eye” appearance is associated with sadness, fatigue, anger, and aging.
With descent of the brows, there is a tendency of the frontalis muscle to increase activity dynamically to counteract the irritant effect of the redundant tissues on the eyelids, thereby initially creating superficial and transient rhytids that become deeper and permanent over time.
Each individual has unique facial expressions and, thus, each develops a unique pattern of upper facial rhytids and eyebrow position. The patient’s skin type, photodamage, tobacco abuse, and many other factors also affect the facial parameters associated with aging.
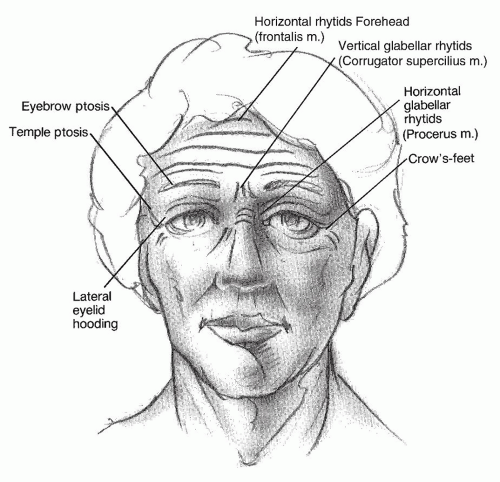 Figure 185.4 Physiology of aging. Ptosis initially occurs at the lateral brow but eventually involves the entire brow and forehead. Rhytids are caused by voluntary and involuntary muscle activity. |
BROW AESTHETICS
The youthful brow, as classically described by Westmore in the 1970’s, is an arch whose apex terminates above the lateral limbus of the iris, with the medial and lateral ends of the brow at the same horizontal level. With evolving concepts of beauty, the ideal brow apex has been described anywhere from the lateral limbus to the lateral canthus (5,6,7). A recent study found that the deep temporal fusion line is the most precise indicator of brow peak position, which makes the most sense intuitively and anatomically. The club-head-shaped medial brow should be in line with a vertical line drawn through the insertion of the ala of the nose. It arches superolaterally above the supraorbital rim to its apex somewhere between the lateral limbus and lateral canthus and tapers into a handle shape to end laterally at an oblique line drawn through the ala of the nose and the lateral canthus. The medial and lateral ends of the eyebrows should lie in the same horizontal plane. In men, the brow is ideally at the level of the supraorbital rim whereas in women the brow should peak above the supraorbital rim. The more lateral the apex of the brow, the more feminized the brow is. Eyebrow hairs are typically thicker in men and may extend in any direction. A lower, thicker brow may still be considered attractive in women, depending on its harmony with their overall facial aesthetics.
ASSESSMENT
Each patient must specify his or her particular concerns if the appropriate procedure is to be chosen for forehead rejuvenation. Oftentimes, a patient will seek correction of lateral eyelid hooding and request blepharoplasty when the ideal procedure may well be one to elevate ptotic brows. During analysis for the patient seeking facial rejuvenation, the surgeon must demonstrate the patient’s own natural brow position in repose as most people with brow ptosis will unconsciously elevate their brows. A previous history of upper blepharoplasty or brow lifting procedures may produce a relative lack of upper eyelid skin for lifting procedures. Additionally, a history of laser-assisted in-situ keratomileusis surgery or dry-eye problems must be considered prior to brow lifting since a transient lagophthalmos following surgery is not uncommon. Patients with alopecia may be at an increased risk for surgical hair follicle shock. Young men with a full head of hair and who are not at risk of developing male-pattern baldness, or older men who have an established pattern of hair loss, may be candidates for coronal forehead lifts and its modifications. Hair transplantation in conjunction with a forehead lift has been described, allowing for expanded use of a pretrichial incision.
Ptosis
It is of paramount importance for the surgeon to differentiate between lateral eyelid hooding that is a result of upper eyelid skin redundancy and that due to ptosis of the eyebrow. Frontalis contraction must be eliminated by complete patient relaxation to eliminate pseudoelevation of the eyebrows. Patients with eyebrow ptosis will be disappointed with a blepharoplasty procedure without addressing the
brows. Younger patients with ptotic brows and upper eyelid hooding without other signs of upper facial aging often see greater improvements with a forehead lift rather than upper eyelid blepharoplasty. Overaggressive resection of brow or eyelid skin may result in further brow ptosis and a short upper lid syndrome. The effects of the forehead lift/browlift may be demonstrated to the patient by gently elevating the forehead in the midline and laterally. The degree of surgical brow elevation required can be assessed by having the patient actively elevate the eyebrows while the surgeon holds a ruler at a predetermined landmark on the brow. This method allows for the ideal amount of brow elevation to be determined. A slightly greater excision of skin should be made to allow for a degree of stretch-back. For example, about 16 mm of skin may be excised if the real amount of aesthetic lift desired is 10 to 12 mm.
brows. Younger patients with ptotic brows and upper eyelid hooding without other signs of upper facial aging often see greater improvements with a forehead lift rather than upper eyelid blepharoplasty. Overaggressive resection of brow or eyelid skin may result in further brow ptosis and a short upper lid syndrome. The effects of the forehead lift/browlift may be demonstrated to the patient by gently elevating the forehead in the midline and laterally. The degree of surgical brow elevation required can be assessed by having the patient actively elevate the eyebrows while the surgeon holds a ruler at a predetermined landmark on the brow. This method allows for the ideal amount of brow elevation to be determined. A slightly greater excision of skin should be made to allow for a degree of stretch-back. For example, about 16 mm of skin may be excised if the real amount of aesthetic lift desired is 10 to 12 mm.
Rhytids
Static and dynamic rhytids should be assessed preoperatively. Assessment of the forehead, glabella, and temple rhytids, along with the relative degree of activity of the upper facial muscles with mimetic expression, helps to determine the extent of myoplasty required for the involved muscles. Older patients typically have more subcutaneous atrophy and thus rhytids are more pronounced due to the actions of the muscles being transmitted more directly to the skin.
Hairline Patterns
Women who have a medium or low forehead hairline are candidates for the standard coronal or endoscopic forehead lift, since both of these will elevate the height of the hairline. Women with higher hairlines most often benefit from a trichophytic lift, which not only maintains their hairline position but also reduces the vertical height of their high forehead. This eliminates the need to style their hair over their forehead to camouflage a high hairline that would result from a standard coronal lift. Older men without evidence of male-pattern balding may be candidates for a standard coronal or trichophytic lift as well.
Skin Type
Fair- and thin-skinned patients usually heal with more ideal scars than those with darker and thicker or sebaceous skin. In general, women scar better than males. Older patients often have finer scars than do younger patients because of their decreased skin elasticity.
Asymmetries
It is documented that 97% of all patients have facial asymmetries (7). Both passive and dynamic asymmetries of the eyebrows should be documented. The surgeon should not try to alter dynamic eyebrow symmetries. Additionally, the surgeon must take caution in an attempt to correct passive asymmetries as this may alter the patient’s unique facial characteristics. Even when such attempts are made, the coronal forehead lift and its modification are usually unsuccessful in correcting eyebrow asymmetries because of the distance from the incision to the eyebrows. If such correction is desired, a direct eyebrow or midforehead eyebrow lift are likely to be more successful. Patients with hyperdynamic forehead muscle activity may need more aggressive myoplasties to decrease this degree of activity and minimize recurrence of forehead and glabellar rhytids. This may be achieved surgically or with neurotoxin. The clinical assessment and photographic documentation must be performed with the patient’s facial muscles in repose.
Bony Contour
Women with prominent supraorbital rims and excessive forehead bossing may appear masculinized. They may benefit from bone reduction of the supraorbital rim or alloplastic augmentation in association with a coronal forehead lift (8).
PREOPERATIVE COUNSELING
It is imperative to communicate to the patient that brow lifting will have no effect on the eyes other than to improve brow position and lateral hooding. Conversely, upper blepharoplasty will not alter eyebrow position, and if overaggressive skin resection is performed, this may cause further lateral eyebrow ptosis. The lateral infrabrow skin cannot be excised during upper blepharoplasty and, thus, minimal improvement may be achieved in the patient seeking correction of lateral hooding with an upper blepharoplasty rather than with some form of eyebrow lift. Patients should be advised that rejuvenation survey will “turn the clock back” but will not stop the aging process. The patient’s specific concerns in conjunction with full facial assessment must be addressed; this is the only way the correct procedures can be chosen. Patients seeking a face-lift should be advised that it will not alter the appearance of the upper face.
MANAGEMENT
During the consultation with the patient, all options—including surgical and nonsurgical options—should be discussed. Surgery may not always be indicated; other methods may be used to correct a specific defect that is of great concern to the patient or to temporize until the patient is a better candidate for surgery. Other such methods include the following:
Sun avoidance and protection will prevent photodamage to the skin and help prevent squinting and thus decrease vertical glabellar rhytids.
Judicious use of cosmetics may camouflage forehead rhytids.
Retin-A cream may increase the vascularity of the skin and the organization of collagen bundles and may thicken the skin, resulting in a more youthful overall appearance and improvement in fine rhytids. It does not improve deeper furrows. Chemical peels and laser resurfacing will provide a greater effect.
Styling the hair over the forehead will camouflage rhytids, although it usually cannot camouflage brow ptosis.
Injectable fillers may be used selectively for temporary effect in forehead rhytids or furrows and crow’s-feet. Fillers have also been used to simulate a brow lift with some success (9).
Eyeglasses may camouflage both brow ptosis and glabellar rhytids.
Onabotulinumtoxin A (Botox®, Allergan, Inc., Irvine, CA) injections can provide several months of partial muscle paralysis with partial or complete effacement of furrows. Additionally, Botox can be injected into the lateral brows to provide several millimeters of elevation.
All patients should be counseled that the goal is improvement, not perfection. Furthermore, although rejuvenation is achieved, aging continues and cannot be stopped or reversed. Patients will appear younger than if they had not had the surgery but in time will redevelop most of the same features that were improved by the surgery. Patients must acknowledge that a specific result, a “perfect” result, or a no-risk procedure cannot be guaranteed. Each procedure will have specific effects, and patients must be aware of what will and will not be achieved with the procedures they choose. Specifically, patients should be counseled about the general and local complications associated with the procedures they are contemplating, outlining the preoperative, postoperative, and surgical protocols in detail. Literature with instructions and advice about the surgery should be given to the patient, because a well-informed patient can choose the procedure that has the highest likelihood of success for him or her. Of primary importance in forehead rejuvenation procedures are the patient’s specific goals, the hairline changes involved, and the acceptability of scar placement.
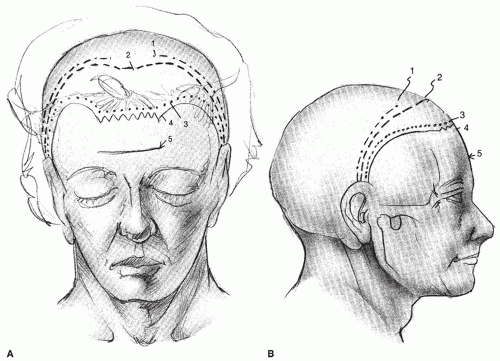 Figure 185.5 The coronal incision is the standard incision. Modifications may be made depending on the patient’s hairline, degree of ptosis, rhytids, skin type, asymmetries, sex, and personal preference. A: Frontal view. B: Lateral view. 1, Bilateral (temporal); 2, coronal (forehead); 3, trichophytic; 4, pretrichial; 5, midforehead. |
SURGICAL PROCEDURE AND TECHNIQUE
Surgical rejuvenation of the upper face can be considered within three categories: the coronal forehead lift and its modifications (Fig. 185.5), the direct brow lift and its modifications (Fig. 185.6), and the endoscopic forehead lift. The indications and surgical technique for each of these follow.
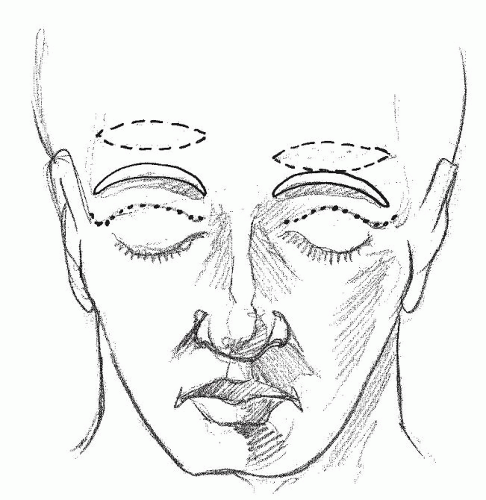 Figure 185.6 The direct brow lift (solid lines) is the standard incision. More recent modifications, such as the indirect brow lift (dashes) and browpexy (dots), can be useful in selected patients. |
Coronal Forehead Lift
The coronal lift and its modifications are arguably the procedures of choice for rejuvenation of the upper face. Numerous recent reviews have validated its efficacy, safety, longevity, and high degree of patient satisfaction (2,10,11,12). The coronal lift is especially useful for patients who have both generalized ptosis and rhytids of the upper face and a normal or low hairline (Fig. 185.7). Relative contraindications include men with male-pattern baldness and women with high hairlines. Due to the distance between the incision and the brow, the coronal lift and its modifications are not useful to correct static or dynamic brow asymmetries. Advantages of the open lifts are the well-hidden incision within and behind the hairline and excellent exposure of the forehead musculature, allowing accurate and extensive myoplasty. Disadvantages include elevation of the frontal hairline, although this is an advantage in patients with a low frontal hairline. Other disadvantages include the temporary, and occasionally permanent, hypesthesia or paresthesia posterior to the incision line, although a recent study by Guillot et al. (13) presents good prospective and retrospective data concluding that this may not be a clinically significant disadvantage in the long term. Wide surgical undermining increases the risk for blood accumulation, and tension on the wound closure may predispose to temporary or permanent hair loss, especially if the wound is not meticulously closed in multiple layers.
 Figure 185.7 A: Sixty-four-year-old female with a short forehead, brow ptosis, and prominent horizontal forehead rhytids. Note the hyperdynamic elevation of the brows commonly observed in patients with brow ptosis. B: One year following coronal forehead lift, upper and lower blepharoplasty, and deep plane face- and neck lift. Note that the brows are now in an improved position without dynamic movement. Note the slight increase in the length of the forehead. C: Four years following the above-mentioned procedures—note the longevity of the open forehead lift. |
Technique
The procedure is done under either local intravenous sedation or general anesthesia. General anesthesia is preferable, especially if multiple other procedures are being
performed (14,15). A curvilinear incision about 4 to 6 cm posterior to the anterior hairline is marked, and a thin strip of hair is removed along the incision line. Local infiltration of anesthesia of lidocaine 1% with epinephrine 1:100,000 and bupivacaine 0.5% with epinephrine 1:200,000 mixed in equal parts is used initially to effect a regional block at the supratrochlear and supraorbital nerves. Following this, a ring block is completed by following the supraorbital margins, the zygomas, and the scalp at the incision site. Infiltration is completed in the subgaleal plane beneath the entire area of the flap to be elevated. At least 7 minutes must be allowed for adequate vasoconstriction.
performed (14,15). A curvilinear incision about 4 to 6 cm posterior to the anterior hairline is marked, and a thin strip of hair is removed along the incision line. Local infiltration of anesthesia of lidocaine 1% with epinephrine 1:100,000 and bupivacaine 0.5% with epinephrine 1:200,000 mixed in equal parts is used initially to effect a regional block at the supratrochlear and supraorbital nerves. Following this, a ring block is completed by following the supraorbital margins, the zygomas, and the scalp at the incision site. Infiltration is completed in the subgaleal plane beneath the entire area of the flap to be elevated. At least 7 minutes must be allowed for adequate vasoconstriction.
The coronal incision is beveled parallel to the shafts of the hair follicles, usually obliquely anterior at the midline and becoming more horizontal or even obliquely posterior in the temple region (Fig. 185.8). The flap is elevated with broad scalpel sweeps with a no. 10 blade in the subgaleal plane, abetting this action with firm upward traction on the flap. The pericranium is kept intact and moistened with saline gauze. Prominent vessels may be seen coursing superiorly from the supraorbital vessels about 2 to 3 cm superior to their origin. Scalpel dissection is carried inferiorly to about 1 cm above the supraorbital rims. Dissection laterally must be carried down to the zygoma; this is most safely done with the blade handle and gentle blunt dissection just above the temporalis fascia.
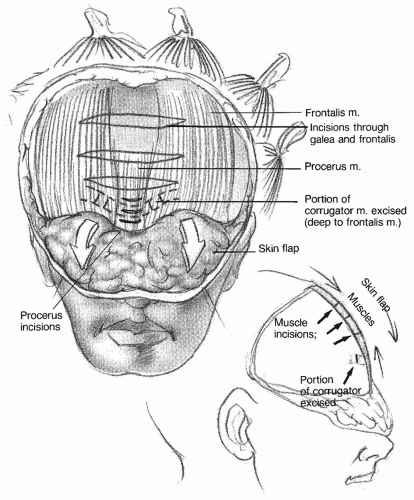 Figure 185.8 The coronal incision is beveled parallel to the shafts of the hair follicles. The flap is elevated over the supraorbital margins and to the zygoma. A portion of the corrugator supercilius is excised, and the procerus and frontalis are incised. |
Myoplasty is performed through blunt interfibrillar scissors dissection to identify and free the corrugator muscles from the supratrochlear and supraorbital nerves and vessels, which are multiple and course around the muscle. The flap is dissected over the supraorbital rims, releasing the arcus marginalis, but not so far as to expose orbital fat. In this way the brow is freed so that it may be elevated above the supraorbital rims. The muscle is cauterized with bipolar cautery at two points about 1 cm apart, and the central portion excised. Any bleeding is meticulously controlled with bipolar cautery, taking care not to injure any nerves. The procerus in the midline is identified and incised horizontally using unipolar cautery. The frontalis muscle is identified in the flap, and the unipolar cautery is used to incise the muscle and galea immediately deep to the prominent transverse forehead creases. Cauterization is maintained medial to the pupils to prevent injury to the temporal branch of the facial nerve and also to preserve some natural forehead movement through the action of




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
