29 Temporal Bone Trauma
The evaluation and management of a temporal bone fracture will often occur in the setting of multiple additional injuries. Penetrating or blunt trauma can involve any of the structures within the temporal bone, including the glenoid fossa, external auditory canal (EAC), tympanic membrane (TM), ossicles, cochlea, semicircular canals, facial nerve, cochleovestibular nerve, cranial nerves IX to XII, the carotid artery and/or jugular vein.
A detailed examination is warranted in the setting of a temporal bone fracture as these injuries are often associated with epidural, subdural, and parenchymal hematomas. Injury to the internal carotid artery (ICA) can produce life-threatening hemorrhage and/or ischemic brain injury.1,2 Permanent sequelae include hearing loss, balance disturbance, facial nerve paralysis, increased intracranial pressure, and signs and symptoms associated with a postconcussive syndrome.
Epidemiology
Multisystem trauma is still a prevalent problem despite technological advances in motor vehicle safety and legislative safety measures. Head trauma is especially common, and in cases where a skull fracture is identified the incidence of skull base trauma increases significantly. The incidence of temporal bone fractures is up to 4% in the setting of a head injury.3 Temporal bone fractures are identified in up to 22% of patients who sustain skull fractures.2
Motor vehicle accidents are the most common cause of temporal bone trauma followed by assault. Recreational vehicles (i.e., all terrain vehicles) and large flat screen television monitors are another emerging source of head and temporal bone trauma. A higher incidence of temporal bone trauma has been noted in males secondary to increased high risk behaviors (assault, recreational vehicles, driving under the influence).2 Bilateral temporal bone trauma is occasionally encountered and must be kept in mind during the patient assessment and when surgical intervention is necessary.
Fracture Classification
Classic System
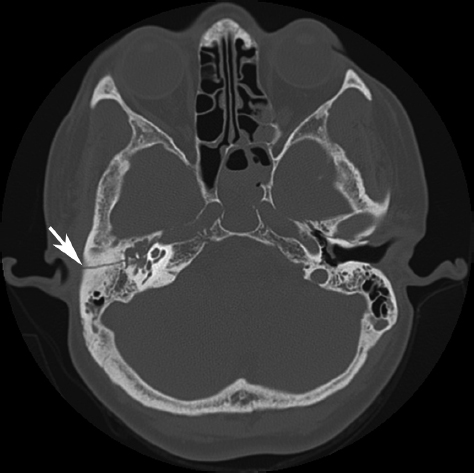
Fractures of the temporal bone have historically been classified based on the fracture orientation with respect to the petrous ridge. A longitudinal or oblique fracture courses parallel or tangential to the petrous ridge and is the most frequent fracture pattern encountered (70 to 90%) (Fig. 29.1). These fractures typically involve the squamous and tympanic portion of the temporal bone and often present with bloody otorrhea and conductive hearing loss. Transverse fractures, which are perpendicular to the petrous ridge, occur in up to 30% of patients (Fig. 29.2).2,4 These fractures typically involve the mastoid and petrous portions of the temporal bone and often present with hemotympanum, sensorineural hearing loss, and vertigo. The incidence of facial paralysis is substantially higher in transverse fractures as compared with longitudinal fractures. A mixed fracture, which has elements of both transverse and longitudinal fractures, is occasionally encountered. Recent studies suggest that the classic method for describing temporal bone fractures does not accurately predict neurotologic complications, nor does it help with selecting an otologic surgical approach when necessary.4–6
Otic Capsule System
The classic system for characterizing temporal bone fractures has been essentially replaced with a more anatomic classification system with respect to the otic capsule.2 Fractures that do not disrupt the otic capsule (cochlea, semicircular canals, and vestibule) are classified as otic capsule sparing fractures as opposed to otic capsule disrupting fractures (Fig. 29.3). Otic capsule disrupting fractures are far less common 2.5 to 5.8% (Fig. 29.4).2,5 Interestingly this scheme demonstrates that most transverse fractures do not disrupt the otic capsule and that many otic capsule disrupting fractures are in fact longitudinal.5
The importance and relevance of this newer classification scheme is evidenced by the increased incidence of neurotologic complications associated with otic capsule disrupting fractures as opposed to those that spare the otic capsule. Prediction of neurotologic complications was found to be superior using the otic capsule system as opposed to the classic system.6 The incidence of facial paralysis in otic capsule disrupting fractures is up to 50% as opposed to 13% in otic capsule sparing fractures. Patients with an otic capsule disrupting fracture have up to a 10-fold higher risk of a cerebrospinal fluid (CSF) fistula compared with those with otic capsule sparing fractures.6 Sensorineural hearing loss is almost universal in otic capsule disrupting fractures; however, audiometric assessment is still imperative before otologic surgical intervention as cochlear reserve is sometimes present, particularly in fractures that only traverse the semicircular canals.4 Otic capsule sparing fractures more commonly present with conductive or mixed hearing loss.6
Penetrating Trauma
The vast majority of penetrating trauma to the temporal bone is secondary to gunshot wounds (GSW). GSW are typically divided into high versus low velocity. A low-velocity missile travels less than 2000 ft/s. Handguns generally produce low-velocity injuries as do shotguns unless the range is very close. Rifles generally produce high-velocity wounds. High-velocity wounds cause injury not only by crush and laceration, but also by cavitation that is produced by shock waves as the bullet’s kinetic energy is dissipated.7 The cavitation may involve tissues many centimeters distal to the bullet’s trajectory and are frequently subtle. Vascular injury due to stretching of vessels is common and injury to the ICA should be suspected especially in high-velocity wounds.8
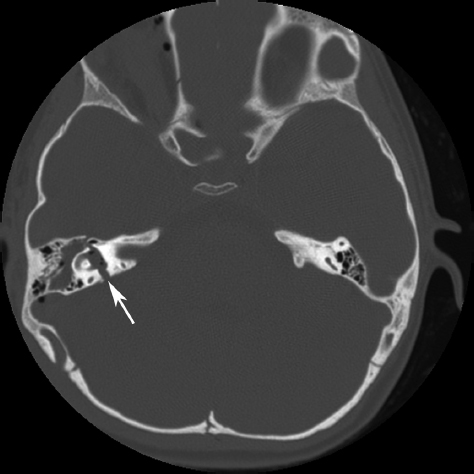
Figure 29.2 Axial bone window temporal bone computed tomography scan demonstrating a transverse fracture at the level of the vestibule (arrow). This fracture is perpendicular to the petrous ridge.
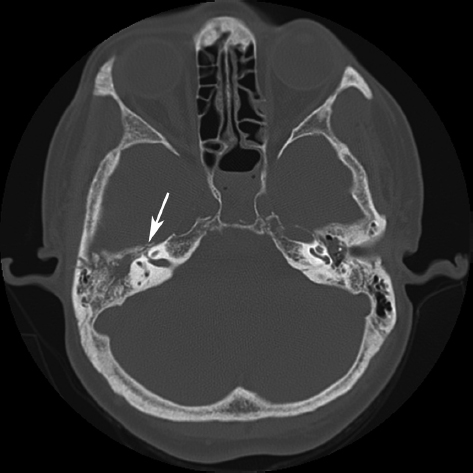
Figure 29.3 Axial bone window temporal bone computed tomography scan showing an otic capsule sparing fracture extending from the cortex to the perigeniculate facial nerve (arrow).
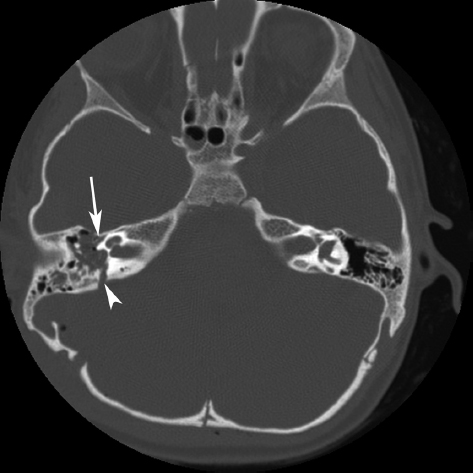
Figure 29.4 Axial bone window temporal bone computed tomography scan showing an otic capsule disrupting fracture extending through the inferior aspect of the vestibule (arrow).
Injury to the facial nerve occurs in approximately 50% of GSWs to the temporal bone but more frequently involve the labyrinthine or tympanic segment as opposed to the perigeniculate facial nerve as is common following blunt trauma.9,10 Laceration of the EAC with subsequent stenosis and cholesteatoma formation is also more common following penetrating trauma.
Blunt Trauma
Substantial force (between 1000 and 2000 psi) is generally required to produce a blunt temporal bone fracture. The majorities of blunt temporal bone fractures occur as a result of either automobile or motorcycle accidents. Motorcycle injuries are disproportionately more common than automobile injuries. Collisions with pedestrians are less common. Falls from height or during recreational activities (biking, skating, skateboarding, and skiing) constitute a second category of relatively common causes for blunt temporal bone trauma. The remaining significant of etiology for blunt trauma is assault.4
Pediatric Temporal Bone Trauma
Fractures of the temporal bone occur in children, although they are relatively uncommon. The etiologies for pediatric temporal bone fractures parallel the etiologies seen in adults: 85% are due to vehicular accidents or falls.11–13 Associated central nervous system (CNS) trauma is common and occurs in approximately 40 to 75%. Lee et al reported that isolated fractures of the squamosa are associated with a higher degree of CNS injury than fractures in other portions of the temporal bone.13
Facial nerve paralysis is less common in children than adults, ranging between 3 and 9%.11–13
Temporary CSF leak is also common but generally resolves spontaneously. The exact incidence is unknown. Bloody drainage from the ear canal often stops before a definitive diagnosis of CSF otorrhea can be made. Separate management protocols for pediatric temporal bone fractures have not been developed and management in children is essentially the same as in adults.
Symptoms
Hearing loss is relatively common, occurring in 40 to 60% of patients with temporal bone fractures. The majority of cases of hearing loss are conductive because of disruption of the TM, blood in the middle ear space, or dislocation of the ossicles. Bloody otorrhea occurs in a significant number of cases. Bleeding can occur not only as a result of TM laceration, but also as a consequence of EAC skin disruption from an underlying fracture. Early on it is often difficult to distinguish bleeding alone from blood mixed with CSF.4
Vertigo is present in the minority of patients but may be difficult to initially assess because of concurrent CNS and associated injuries.4
Facial nerve weakness may occur immediately and be present at presentation or develop later on in the clinical course. It is important to determine as early as possible whether or not facial function is present. The presence of even minimal facial nerve function is important in determining the need for facial nerve decompression.4
Signs
The earliest sign of temporal bone fracture is often loss of consciousness, which occurs in a significant number of patients. Loss of consciousness or altered consciousness is because of associated CNS injuries which are relatively common. Assessment of level of consciousness using Glasgow Coma Scale can be important in determining prognosis. As noted above, it is often impossible to confirm whether the bloody otorrhea is caused by bleeding alone or if there is an associated CSF fistula.
Classic signs of temporal bone fracture are ecchymosis of the periorbital area and retroauricular area over the mastoid cortex (Battle sign). These signs, however, often develop 24 to 48 hours following injury. Hearing loss is frequently present. Conductive hearing loss can be distinguished from sensorineural hearing loss in the awake patient using a tuning fork. The distinction between conductive and sensorineural hearing loss is important: the presence of vertigo or facial nerve paralysis associated with sensorineural hearing loss is a reliable sign of temporal bone fracture. TM perforation is present in only a minority of patients and usually cannot be definitively determined until the EAC is carefully cleaned using aseptic technique. Similarly, when the TM is intact, hemotympanum is present in more than half of individuals with temporal bone fracture but often its presence is detected only after cleaning the EAC. Cleansing of the canal must often be deferred because of the presence of more serious injuries and an uncooperative patient.4
Patient Assessment
Because great force is required to produce a temporal bone injury, temporal bone trauma is frequently associated with other life-threatening injuries. Consequently, initial evaluation must begin with assessing the “ABCs.” Attention must be given to the possible presence of associated injuries, including spine fractures, CNS injury, thoracic injuries, and abdominal injuries. Attention should be focused on the temporal bone only after a full trauma assessment has been completed. The presence of associated injuries is so common that otolaryngology consultation is often sought only after stabilization and management of life-threatening injuries by first line trauma physicians.
If alert and awake, the patient should be queried as to the presence of hearing loss and vertigo. If the patient is dizzy, the physician should determine whether the vertigo is rotational, its severity and whether or not it is associated with visceral autonomic symptoms such as nausea or diaphoresis.
If a complete facial nerve paralysis is present, then the eye must be protected from corneal dehydration and abrasion. An attempt should be made to examine the EAC. It will often be filled with blood and sometimes CSF. Presence of a CSF from the EAC may be obvious. Consequently, care should be taken to minimize contamination during the examination of the EAC. Antiseptics should be utilized and a gloved examination with clean instruments should be undertaken. The presence of blood in the EAC or behind the TM is an excellent predictor of a temporal bone fracture.14
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


