38 Hearing Rehabilitation with Osseointegrated Implants
The principle of bone-anchored hearing aids is to circumvent the external and/or middle ear to amplify and transmit sound to the inner ear. There are several specific situations in which this becomes relevant, including the anatomic obstacles of aural atresia or a chronically draining ear as well as single-sided deafness. Despite surgical attempts at correcting such problems, there are still limitations that can preclude adequate hearing or fitting for an air conduction hearing aid, and this is the niche the bone-anchored hearing aid fills.
There are currently two U.S. Food and Drug Administration (FDA)-approved devices on the market in the United States: the BAHA by Cochlear Corporation (Mölnlyeke, Sweden) and the Ponto Device by Oticon Medical (Somerset, New Jersey, United States). Both devices are designed to sit postauricularly, not lie within the external auditory canal or pinna, and provide direct bone conduction of sound to the inner ear. The BAHA has been on the market the longest and has a rich body of literature to support its efficacy and role in the armamentarium of sound amplification in specific conditions of hearing loss.
Historical Perspective
The principle of bone conduction hearing dates back to the 17th century when John Bulwar and George Sibscota applied the principles of bone conduction to aid the hearing impaired.1 The Audiphone (Chicago, Illionis, United States), patented in 1879, was a hearing fan that operated by bone conduction and spurred the development of several similar devices.1 Nearly 100 years later, with the advent of osseointegration technology, work specifically on bone-anchored aids yielded the Audiant and BAHA (prior terminology).
Research into the understanding of bone conduction hearing resurged in the 1960s and led to some of the current understanding of the relationship of bone vibrations to cochlear stimulation. A thesis by Stenfelt condenses the principles of bone-conducted sound perception: sound pressure in the ear canal and the occlusion effect, inertia of the middle ear ossicles, inertia of cochlear fluids and fluid pressure transmission, and alteration of the cochlear space.2 The inertia of cochlear fluids is attributed to the vibration of the temporal bone surrounding the cochlea and resulting in a pressure gradient across the basilar membrane, causing a traveling wave.2 A smaller component of it is attributed to the transmission of vibrations to the cranial space, which are then transmitted to the cochlea via a patent cochlear aqueduct or other similar channel (i.e., vestibular aqueduct). As the transverse wave propagates in the skull, it compresses and expands the bone, resulting in deformation in the cochlea and fluid movement within it.2 These principles are important to understanding how the bone-anchored hearing aids work and to what degree.
The conventional bone conduction hearing aid is a transcutaneously applied transducer and amplifier held firmly against the scalp with a headband or spectacle frame. The major complaints of users were the discomfort from the constant pressure, the unsightly appearance, and poor sound quality at high frequencies.3,4 The degree of pressure required to adequately transduce and conduct sound has resulted in reports of headaches, pressure sores, and even head deformity in children. In addition, the soft tissue distorts the sound, demanding use at near maximal settings. These pitfalls and the advent of osseointegration paved the way for bone-anchored hearing aids.
Osseointegration was first discovered by Brånemark in Sweden in the 1950s. He found that osteoblasts would grow in tight apposition to undisturbed titanium screws left in bone with no intervening soft tissue and became firmly anchored.5 In 1965, he first proved its application in humans to fit dental implants.6 This technology then led to multiple different uses, including its application in hearing aids.
Two devices came to the market as bone-anchored hearing aids in the 1980s: the Audiant by Xomed (Jacksonville, Florida, United States) and the BAHA originally made by Entific. The Audiant was introduced by Dr. J. Hough, which was based on the principle of magnetic adherence and ability to vibrate in synchrony. One magnet was anchored within the temporal bone and the external one was placed within a coil. The electromagnetic energy generated by the coil would then be transferred transcutaneously to the magnet anchored within the temporal bone and result in the vibration of the magnet and thus the temporal bone.7 This device is no longer in use in the United States. A new device, the Sophono, based on similar principles has been introduced with the advantage of modifying the strength of the external magnet, but currently there is limited data on the efficacy of the device.
The BAHA was originally developed by Tjellström et al and became commercially available in 1987 where in he connected an external oscillator percutaneously to an osseointegrated screw in the temporal bone.8 It was not until 1997 that it was FDA approved for use in the United States. Till date, there are three different models of the BAHA that accommodate different user needs: BAHA 3, BAHA 3 Power, and Cordelle II. Another recent device is the Ponto Device, introduced in the market in 2009. The differences and marketed advantages of the Ponto Device are the angled screw allowing for a more contoured fit and improved hearing in noise. Data on the newer devices are still pending, but continued research to perfect the system is promising. This discussion focuses on the BAHA device, as it has the most substantial body of evidence.
Principles of BAHA
The BAHA is composed of three components: the titanium implant, the abutment, and the processor (Fig. 38.1). The surgical procedure is now more commonly a one-step procedure, though it may still be done in two stages in children, whereby the implant and abutment are placed and after an adequate amount of time is allowed for osseointegration (6 to 12 weeks for adults and 12 to 24 weeks for children) the sound processor can be attached. The indications for BAHA can be divided into otologic criteria (Table 38.1) and audiologic criteria. The audiologic criteria include a conductive hearing loss, mixed hearing loss, or single-sided deafness. The specific devices have different capacities for sound amplification and therefore different bone conduction threshold criteria; however, in all cases a minimum speech discrimination of 60% is required. The BAHA 3 is ideal for patients with a bone conduction threshold (at 0.5, 1, 2, and 3 kHz) of 45 dB or less, the BAHA 3 Power has a slightly lower threshold of 55 dB, and the Cordelle II works for patients with a bone conduction threshold of 65 dB or less (Fig. 38.2). In patients with single-sided deafness, the profoundly impaired side, usually with thresholds greater than 90 dB, is implanted, provided the better hearing ear has pure tone air threshold losses of no more than 20 dB at 0.5, 1, 2, and 3 kHz. Otologic indications include chronic draining ears, aural atresia with an intact cochlea, conductive hearing loss because of ossicular disease that cannot be surgically corrected, dermatitis or hypersensitivity to the ear molds, or tumor of the external auditory canal or middle ear space.
Currently, the FDA approves the BAHA in children who are 5 years or older. Relative contraindications that must be considered by the clinician include local skin disease or mental or psychological impediment to appropriate care and hygiene of the device and site. The preoperative assessment is important in identifying appropriate candidates and also in managing expectations and preparing the patient for maintenance. During the preoperative assessment, a full history and head and neck examination should be performed. Radiologic imaging studies are not a prerequisite but may be useful in cases of congenital abnormalities. The patient can also have a test trial with a BAHA testband. It is worth mentioning to the patient that the output of the testband is weaker than the actual implant.
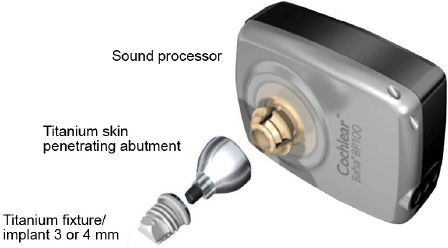
Figure 38.1 BAHA components—sound processor, abutment, and titanium implant.
Printed with permission from: Cochlear Americas, Somerset, New Jersey, United States.
Technique
The original technique described a two-stage procedure performed under general anesthesia where the implant was first placed and left to allow osseointegration to take place and then the overlying soft tissue was thinned and the abutment was placed. In adults it is now commonly done with local anesthesia in one stage where the implant and abutment are placed simultaneously. In young children it is generally still done as a two-stage procedure to allow for adequate osseointegration; however, multiple surgeons have made attempts to improve on the procedure and reduce the exposures to general anesthesia.9
First, the skin incision is planned and the skin and soft tissue is elevated. The fixture is placed 55 mm posterior and slightly superior to the posterior edge of the meatus to prevent the processor from touching the pinna. The flap is then outlined with a marking pen, and local anesthesia is infiltrated.
Table 38.1 Indications and Contraindications for the BAHA
Indications | Contraindications |
Chronic draining ear Congenital or acquired malformation of the external auditory canal (atresia and tumor) Chronic otitis media Chronic otitis externa Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|