21
Temporal Bone Trauma
May Y. Huang and Paul R. Lambert
Temporal bone trauma occurs in 30 to 75% of head injuries.1–7 Compared with the face and skull, the temporal bone is very dense and requires a tremendous amount of force to sustain fracture. The majority of temporal bone injuries are associated with other multiple traumas following motor vehicle accidents. Temporal bone trauma also may be associated with industrial accidents, recreational injuries, falls, assaults, or self-inflicted injuries. Types of temporal bone trauma include blunt trauma without fracture, blunt trauma with fracture, penetrating trauma, compressive injuries, and thermal injuries. Trauma may cause injury to specific parts of the external, middle, or inner ear in addition to other structures within the temporal bone. Frequently, the history of the type of temporal bone injury facilitates evaluation of the spectrum of potential sequelae.
 Anatomic Considerations
Anatomic Considerations
The temporal bone is a wedge-shaped bone in the lateral skull base that is bordered by the middle fossa tegmen superiorly, the posterior fossa tegmen posteriorly, the temporomandibular joint anteriorly, the clivus and foramen magnum medially, and the infratemporal fossa inferiorly. The temporal bone is divided into four regions: squamous, petrous, mastoid, and tympanic. Its posterosuperior border is called the petrous ridge, which lies along the long axis of the temporal bone at about a 45-degree angle posterior to the midcoronal plane. The squamous portion articulates with the sphenoid bone anteriorly and the parietal bone posteriorly, thus forming the roof of the infratemporal fossa and the medial wall of the temporal fossa. At the base of the skull, the petrous and mastoid portions of the temporal bone lie lateral to the occipital bone at the foramen magnum. The petrous apex is separated from the clivus (the fusion of the occipital and sphenoid bones anterior to the foramen magnum) by the foramen lacerum. At the inferior aspect of the base of the skull medial to the styloid process lie the jugular and carotid foramina.
Vital structures that reside within the anatomic confines of the temporal bone include audiovestibular mechanoreceptors; cranial nerves V, VI, VII, and VIII; the sigmoid sinus; and the jugular bulb. Injury to these vital structures needs to be considered in evaluation of temporal bone trauma.
The seventh and eighth cranial nerves arise from the pons, enter the posterior aspect of the temporal bone at the porus acusticus, and then course laterally in the internal auditory canal toward the vestibule. The cochlea and semicircular canals lie anteroinferiorly and posterosuperiorly, respectively, with respect to the internal auditory canal.
The course of the facial or seventh nerve within the temporal bone can be described in segments: the meatal segment within the internal auditory canal, the labyrinthine segment within the internal auditory canal, the labyrinthine segment and geniculate ganglion, the tympanic segment in the middle ear, and the mastoid segment. From the internal auditory canal the facial nerve passes through the facial hiatus into the labyrinthine segment of the fallopian canal. At the geniculate ganglion it gives off the greater superficial petrosal nerve (preganglionic parasympathetic innervation for lacrimation) and then turns posteroinferiorly (first genu) along the medial wall of the tympanic cavity. It passes superior to the cochleariform process and the oval window. Inferior to the horizontal semicircular canal it turns (second genu) into the mastoid segment. It gives off the stapedial branch and the chorda tympani branch (special visceral afferent innervation for taste and preganglionic parasympathetic innervation for submandibular and sublingual glands) before exiting the temporal bone through the stylomastoid foramen.
The trigeminal of fifth cranial nerve exits the pons and travels anterolaterally from the posterior fossa to the trigeminal ganglion by passing over the petrous apex just deep to the attachment of the tentorium cerebelli. Its branches exit the middle fossa via the superior orbital fissure, foramen rotundum, and foramen ovale.
The abducens or sixth cranial nerve travels forward from the pons through the dura over the clivus, passing through Dorello’s canal at the petrous apex. The internal carotid artery enters the carotid canal at the inferior aspect of the petrous temporal bone (anterior to the jugular fossa), courses superiorly, and then turns anteromedially just medial to the cochlea and the eustachian tube. The internal carotid artery exits the petrous apex just above the foramen lacerum, ascends in the carotid siphon just lateral to the sella turcica, traverses the cavernous sinus, and enters the dura just medial to the anterior clinoid process.
The middle meningeal artery arises from the maxillary artery in the infratemporal fossa. It enters the temporal bone via the foramen spinosum, runs laterally in the dura over the middle fossa tegmen, and then branches into frontal and parietal branches. It gives rise to the superficial petrosal branch that enters the canal of the greater superficial petrosal nerve.
The sigmoid sinus extends from the transverse sinus to the jugular bulb, coursing from superior to inferior in the dura along the posterolateral aspect of the temporal bone. It receives the greater and lesser petrosal sinuses from the cavernous sinus, as well as the mastoid emissary vein. The jugular bulb lies medial to the vertical segment of the facial nerve and posterior to the ascending portion of the internal carotid artery.
 Classifications of Types of Temporal Bone Trauma
Classifications of Types of Temporal Bone Trauma
Trauma with Fracture
Temporal bone fractures most commonly arise from blunt trauma. They have been traditionally classified as longitudinal or transverse, with respect to the long axis of the temporal bone as viewed from the middle fossa (Fig. 21–1).
Longitudinal fractures are the most common fractures of the temporal bone, constituting approximately 70 to 90% of temporal bone fractures.1–7 This fracture typically results from a direct blow to the temporal or parietal aspects of the head. Symptoms at presentation include conductive hearing loss, bloody otorrhea, and loss of consciousness. Longitudinal fractures are bilateral in 8 to 29% of cases. The facial nerve is injured in approximately 15%. Due to the higher incidence of this type of fracture, however, facial nerve injury is most commonly caused by longitudinal fractures.
The longitudinal fracture line roughly parallels the long axis of the temporal bone in the coronal plane. Classically this fracture extends from the squamous portion of the temporal bone to the anterior portion of the petrous apex in the area of the foramen lacerum and foramen ovale. The fracture thus passes through the posterosuperior aspect of the external auditory canal, the tympanic membrane, and the roof of the middle ear (Figs. 21–2 and 21–3). These fractures commonly disrupt the ossicles or lacerate the skin of the ear canal, but usually spare the otic capsule. Fractures extending through the mastoid rather than the ear canal can result in hemotympanum without laceration of the tympanic membrane.
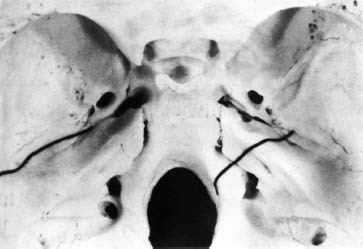
Figure 21–1 Diagram of a longitudinal fracture (left) and a transverse temporal bone fracture (right) as viewed from the middle fossa.
Transverse fractures are far less common, accounting for 20 to 30% of temporal bone fractures. Transverse fractures usually are associated with a blow to the occiput. Symptoms include profound sensorineural hearing loss (SNHL), vertigo, and severe head injury. In approximately 50% of these fractures, a facial paralysis occurs.5,7–9
The transverse fracture extends from the posterior fossa across the petrous pyramid to the foramen spinosum in a more sagittal plane. Transverse fractures extend through the internal auditory canal or the otic capsule. Fractures that arise near the porus acusticus can alternatively end at the oval or round window and produce hemotympanum without laceration of the tympanic membrane (Figs. 21–4 and 21–5).
Few temporal bone fractures are purely longitudinal or transverse. From 50 to 75% of both pediatric and adult temporal bones, fractures could be classified as mixed in their axis of orientation.4,7 In addition, there are not only two axes of orientation but also three planes of orientation by which to describe fractures. Fractures in the oblique plane of orientation are the most common.10–12 As seen from the middle fossa, oblique fractures extend roughly between the coronal and axial planes, across the mastoid cortex, external auditory canal, petrotympanic fissure, and glenoid fossa.

Figure 21–2 Temporal bone fracture.
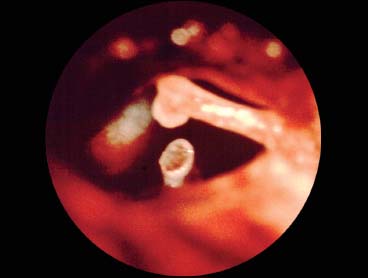
Figure 21–3 Traumatic separation incusstapes.

Figure 21–4 Traumatic hemotympanum.

Figure 21–5 Resolving traumatic hemotympanum.
As in adults, pediatric temporal bone fractures are commonly longitudinal or oblique.13,14 The etiology of pediatric temporal bone fractures includes a higher incidence of falling from heights and automobile-pedestrian accidents. Facial nerve injury and cerebrospinal fluid (CSF) leak may be less common than in adults. The sites of temporal bone injury and their management are similar.
Penetrating Temporal Bone Trauma
The most common type of penetrating trauma affecting the temporal bone is a low-velocity gunshot wound.15 Temporal bone injuries from the typical 0.22-mm to 0.38-mm caliber handgun are most commonly associated with a facial entrance wound rather than one on the side of the head. Mixed or comminuted fractures are most likely; there is no typical pattern of injury. Gunshot wounds of the temporal bone can create a wide variety of specific injuries including trauma to the major vessels, laceration of the dura, and destruction of the middle ear, inner ear, cranial nerves, and central nervous system. The facial nerve is injured in approximately 50% of cases. Usually the associated paralysis is immediate in onset and results from direct nerve injury.
Trauma Without Fracture
Injury to structures of the temporal bone can occur without temporal bone fracture. Such trauma is best enumerated by etiology. Barotrauma, thermal, foreign body, and compressive injuries frequently involve the external and middle ear. Concussive injuries or barotraumas more commonly involve the inner ear.
Blunt head trauma without fracture of the temporal bone may result in SNHL2,16,17 from direct hair cell damage, disruption of inner ear membranes, or fracture of the oval window. A conductive hearing loss can result from ossicular damage or disruption of the tympanic membrane.
Foreign bodies used to remove cerumen, such as hair pins, cotton-tip applicators, pens, pencils, and toothpicks, can traumatize the external auditory canal or the tympanic membrane and result in localized laceration, hematoma, or infection. Injuries from foreign bodies can extend through the tympanic membrane to the middle and inner ear, causing hearing loss with or without vertigo.18,19
Compressive injuries to the ear can result from being slapped or struck on the side of the head or from falling on the water surface during water sports (e.g., waterskiing or diving). These may result in laceration of the tympanic membrane. More significant compressive injuries result from blast injuries. Bomb explosions can cause disruption and implosion of the tympanic membrane as well as high-frequency SNHL due to disruption of the inner ear.20,21
Otitic barotrauma or aerotitis occurs when sudden and severe negative middle ear pressure results in trauma to the ear.22–31 It can be precipitated by concurrent sinonasal inflammation. Symptoms typically include excruciating otalgia during descent flying or ascent from underwater diving. Failure of the eustachian tube to open and adequately equilibrate middle ear pressure with atmospheric pressure causes hyperemia, edema, and ecchymosis of the middle ear mucosa with possible rupture of the tympanic membrane. Perilymph fistulas have also been reported after barotraumas, characterized by fluctuating SNHL and vertigo.32–42
Thermal injuries involve the temporal bone as well. Hot slag injuries sustained during welding can cause a perforation of the tympanic membrane that is difficult to repair (Fig. 21–6) as well as inner ear injury. Also, lightning bolt injuries to the temporal bone can occur from lightning conducted through a telephone to the ear. SNHL, vertigo, tinnitus, and facial paralysis potentially result from devitalized bone and soft tissue.43–47

Figure 21–6 Large traumatic perforation.
 Mechanisms of Injury
Mechanisms of Injury
Auditory
Conductive hearing loss can arise from injury to the external auditory canal, tympanic membrane, or middle ear. Conductive hearing loss can become evident in the acute setting or on a delayed basis. Acutely, the ear canal often is filled with clotted blood, debris, or hematoma. The tympanic membrane may be lacerated, perforated, or completely disrupted. The middle ear may be filled with blood or cerebrospinal fluid. The ossicular chain may be interrupted (Fig. 21–7). Incudostapedial joint separation is the most common ossicular injury, secondary to longitudinal temporal bone fracture.4,48–55 Dislocation of the incus is the second most common finding, followed by fracture of the stapes superstructure. Fracture of the malleus is the least common. Delayed conductive hearing loss can be due to stenosis of the external auditory canal, or ossicular fixation. Ossicular fixation due to fibrous adhesion or bony ankylosis most commonly involves the head of the malleus and the body of the incus.
Severe head trauma of any type is associated with a high incidence of SNHL.2,56,57 Approximately one third of patients with significant closed head injury experience hearing loss, and up to one half of them also have loss of consciousness. SNHL may result from injury to the inner ear, the eighth nerve, or the central auditory system. The inner ear and internal auditory canal may be directly involved, as in a transverse fracture. As many as one third of longitudinal fractures produce high-frequency SNHL, thought to arise from cochlear concussion.58–65 Degeneration of the hair cells in the basal turn of the cochlea may be due either to production of a pressure wave being transmitted through bone to the cochlea or to sudden acceleration-deceleration of the head with sudden movement of the stapes footplate. Disruption of the basilar membrane or tear of the oval window membrane with perilymph fistula may occur with excessive stapes footplate excursion. Traction on the eighth cranial nerve and brainstem contusion are more central etiologies for SNHL.
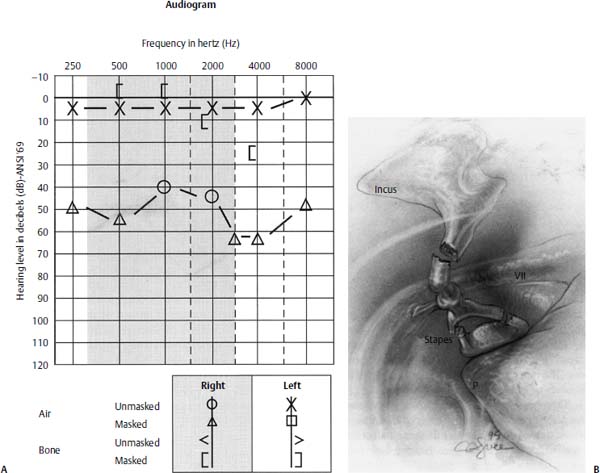
Figure 21–7 (A) Audiogram showing persistent maximal conductive hearing loss many years after a fall. CT scan showed no temporal bone fracture. (B) Diagram of ossicular findings in same patient. Findings during middle ear exploration included fractures of the lenticular process of the incus and both crura of the stapes, as well as incudostapedial joint separation. A stapes prosthesis was successfully placed.
Vestibular
Benign paroxysmal positional vertigo is the most common form of disequilibrium after head injury.16,17,63,64 It occurs in nearly half of patients with longitudinal temporal bone fractures and in one fifth of patients who suffer blunt head trauma without fracture. Typically the onset of symptoms immediately follows the injury. This clinical entity is thought to be due to disruption of the utricular macula. Detached otoconia enter the posterior semicircular canal and render the ampulla sensitive to gravity and thus changes in head position.57,65–70
Traumatic perilymph fistulas may result from fracture or subluxation of the stapes, penetrating trauma, and barotrauma.22–42 Transverse fractures may directly involve the vestibule or semicircular canals and cause a leak of inner ear fluids.71 A perilymph fistula (PLF) is a persistent, abnormal communication between the inner ear and middle ear or the mastoid. Trauma is the third most common cause of PLF, after iatrogenic injuries and idiopathic causes,41 although the traumatic event can involve a relatively minor head injury. The defect is found in the oval window or the round window. Symptoms can include tinnitus, disequilibrium with or without vertigo, aural fullness, and SNHL that may be fluctuating. Patients often describe a popping sensation in the affected ear at the time the fistula occurs. Symptoms cannot reliably predict the site of the fistula. The duration of symptoms is variable but can persist for months. Bilateral PLF is not uncommon.38 The mechanisms of PLF formation are described as implosive or explosive. Implosive PLF such as barotrauma results in inward motion of the oval widow or round window. Explosive PLF results from increased intracranial pressure (e.g., the Valsalva maneuver) transmitted to the labyrinth, possibly by way of an abnormally patent cochlear aqueduct or internal auditory canal. Patients with congenital anomalies such as enlarged vestibular aqueduct are predisposed to PLF from minor head trauma.39 Because the symptom complex caused by PLF is varied, the diagnosis of this entity can be difficult. A specific history of barotrauma or straining coincident with the onset of the symptoms provides some confidence in the diagnosis.
Injury to the labyrinth is more frequently caused by concussion of the labyrinth than fracture. Concussive injury produces shock waves through the inner ear fluids that disrupt labyrinthine membranes.58–62 Traction on the eighth nerve also may result in vestibular symptoms. Brainstem contusion or hemorrhage can involve vestibular nuclei, although trauma to the brainstem usually arises in conjunction with diffuse brain injury.57,65–70,72 Isolated brainstem contusion is unusual. Typical presentation includes multiple cranial nerve palsies, elevated intracranial pressure, and focal neurologic signs.
Facial Nerve
In 80 to 90% of longitudinal fractures, the site of facial nerve trauma is located in the perigeniculate region or just distal to it in the tympanic segment5,8,9,73–75 (Fig. 21–8). Impingement from bone spicules is the most common mechanism of early-onset paralysis, followed by neural contusion. Transverse fractures usually injure the facial nerve in the labyrinthine portion, at or proximal to the geniculate ganglion. The geniculate region may be particularly sensitive to shearing forces in blunt head trauma; its bony covering is frequently dehiscent in this area compared with the surrounding labyrinthine and tympanic segments. In addition, the ganglion is tethered by the takeoff of the greater superficial petrosal nerve. Other mechanisms of injury to the intratemporal facial nerve include transection by fracture, hematoma within the nerve sheath, and edema with constriction in the fallopian canal.
Histopathologically, the extent of facial nerve injury can be classified as neuropraxia, axonotmesis, or neurotmesis (see Chapter 9).76 Neuropraxia is defined as cessation of axoplasmic flow without degeneration of the axon. Axonotmesis describes degeneration of axons with maintenance of the endoneurial sheaths. In neurotmesis, the axons and their endoneurium degenerate. A more detailed classification of neural injuries has been presented by Sunderland,77 who described five levels of injury based on the status of the endoneurium, perineurium, and epineurium. During the first 2 to 3 days of a complete paralysis, or before significant Wallerian degeneration has occurred, electrical tests are not reliable in distinguishing between different levels of injury. Once axonal degeneration has occurred, electrical testing can differentiate neuropraxia from the other injury types. Electrical testing cannot distinguish between axonotmesis and neurotmesis, although the rapidity with which electrical excitability is lost can provide some indirect measure.9,75,77–84 Any type of trauma to the facial nerve will cause a spectrum of neural injuries. If most of the nerve fibers are neuropraxic only, recovery will be excellent and occur rapidly. Recovery will also be excellent if the injury does not progress beyond the level of axonotmesis, although it will be delayed compared with the neuropraxic state, as regrowth of the axons to the motor end-plates occurs. Because the endoneurial tubules are lost in neurotmesis, regenerating axons will become misdirected, resulting in synkinesis, or encounter fibrosis, producing a residual weakness.
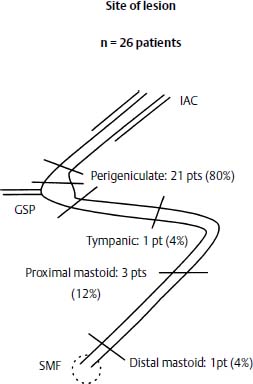
Figure 21–8 Diagram of the middle fossa and mastoid exposure of the intratemporal facial nerve. Arrows indicate the frequency of facial nerve injury at each site in 26 patients following longitudinal temporal bone fracture. IAC, internal auditory canal; GSP, greater superficial petrosal (nerve); SMP, stylomastoid foramen. (Adapted from Lambert PR, Brackmann DE. Facial paralysis in longitudinal temporal bone fracture: a review of 26 cases. Laryngoscope 1984;94:1022–1026. Reprinted with permission.)
Intracranial
Intracranial injuries include trauma to the dura, brain parenchyma, and other neural or vascular structures. Fractures with dural tears or fractures through the otic capsule or internal auditory canal can result in leakage of CSF. Leaks can present as otorrhea, rhinorrhea (via the eustachian tube), or fluid behind an intact tympanic membrane. Multiple cranial nerves can be injured including V, VI, IX, X, XI, and XII. Introduction of air through the fracture into the cranial vault results in pneumocephalus. Mechanisms of brain injury include hemorrhage, contusion, infarct, and edema with increased intracerebral pressure. Herniation of brain through fractures results in encephalocele or meningoencephalocele. Bony fragments also can impinge directly on the brain and cause devitalization of the central nervous system.
Vascular
The location of hematomas can be extradural or subdural. In the region of the temporal bone, hematomas typically arise from injury to the middle meningeal artery. Direct vascular injury can be arterial or venous. Mechanisms of direct injury to the internal carotid arterial system include transaction, laceration, thrombosis, aneurysm, and pseudoaneurysm formation. Fracture or penetrating injury in the mastoid area can lacerate or thrombose the sigmoid dural venous sinus. Associated venous injury includes avulsion of the superior or inferior petrosal sinuses, injury to the jugular bulb, or injury to the cavernous sinus.
 Evaluation
Evaluation
Overall stabilization of the multiple-trauma patient precedes evaluation of specific temporal bone injuries. The history of the traumatic events and any loss of consciousness should be ascertained. Initial assessment is performed with emergency department personnel and includes level of consciousness, adequacy of the upper and lower airway, hemodynamic stability, and central neurologic deficits. The otolaryngologist may need to perform intubation, tracheotomy, or cricothyroidotomy emergently. Life-threatening injuries, such as shock, hemorrhage, expanding hematoma, tension pneumothorax, or cardiac arrhythmia, are the physician’s first priority. In addition, the cervical spine must not be manipulated until instability has been ruled out by lateral neck plain films, preferably in flexion and extension. A pertinent medical history should be elicited from the patient or family members.
Examination of the head and neck can proceed once the patient has been stabilized. This examination must be performed deftly and thoroughly because many people may converge on the patient in the emergency room. Development of a methodical examination prevents the omission or repetition of part of the examination. It is suggested that one proceed from cranial to caudal, including the temporal bones. Examination of cranial nerves can be included with each region. Starting with the scalp and upper third of the face, rule out open skull or sinus fractures. Examine the reactivity and symmetry of the pupils and visual acuity. Check for restriction of extraocular motion, proptosis, enophthalmos, diplopia, and traumatic telecanthus. In the midface, rule out a nasal fracture, septal hematoma, CSF rhinorrhea, hypesthesia, asymmetry, malocclusion, and trismus. When evaluating the lower third and mandible, examine intraorally for fractures, edema, missing teeth, and hypesthesia. For each third of the face, take note of fractures (point tenderness, crepitus, and bony step-off), laceration, and facial motion. Examine lower cranial nerve function if possible, including the larynx and hypopharynx. Palpate the neck for trauma to the airway, hematoma, crepitus, and midline shift.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


