Chapter 43 Technological Innovations in Thyroid and Parathyroid Surgery
Introduction
Since the contemporary era of thyroid and parathyroid surgery began with pioneers like Billroth, Kocher, Mayo, and Halsted, the essential principles of surgery have not drastically changed. A century ago, these surgeons sought to remove diseased glandular tissue while decreasing morbidity and mortality through aseptic technique, adequate hemostasis, and the preservation of laryngeal innervation and parathyroid function.1 Although these rules still apply in the modern area, recent advances in technology have provided the surgeon with new operative approaches and new devices that can assist with anatomic dissection. These techniques have allowed surgeons to use smaller incisions, minimize dissection, avoid drain placement, improve cosmesis, and decrease hospitalizations.
Ultrasonic Energy (Harmonic)
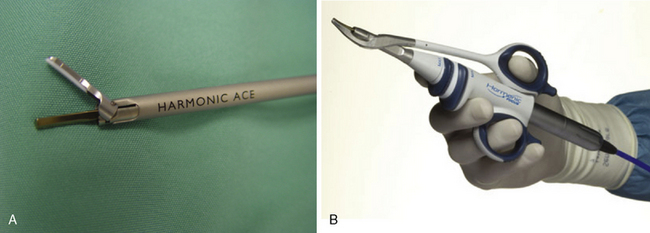
One of the most significant advances in technology, which facilitates conventional surgery but also has allowed departures from traditional thyroid hemostatic approaches for both open and minimally invasive surgery, is the advent of the ultrasonic device (Harmonic ACE; Ethicon Endo-Surgery, Cincinnati, Ohio). The ultrasonic handpiece creates vibrations that occur at 55,500 times per second, which causes simultaneous cutting and vessel coagulation in the tissues contacted. It does so through denaturing cellular proteins, which then form a hemostatic seal.2 This technology is easily applied through small forceps on long extensions, making it an ideal tool for minimally invasive endoscopic and robotic surgery (Figure 43-1). The ultrasonic device has proved to be safe in thyroid surgery, contributing to reduced operating time, inpatient stays, and intraoperative and postoperative bleeding.3 Postoperative discomfort is also improved because there is less thermal injury to surrounding tissues, with no neuromuscular stimulation when compared to standard electrocautery devices.4,5 Hypocalcemia also appears to be reduced because of decreased thermal transmission to the parathyroid glands from the low-temperature ultrasonic energy.6
Bundle Ligation of Superior Pole
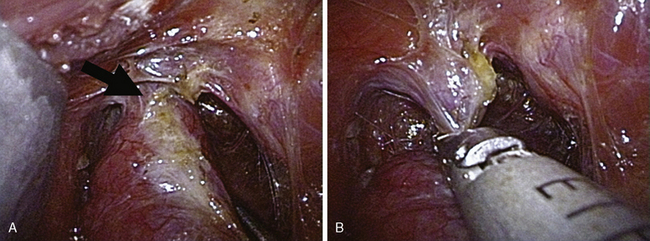
The superior pole vessels (superior thyroid artery and vein) are classically individually isolated prior to their ligation (using suture or clips) and division (with a knife or scissors). Ultrasonic technology can be used to simultaneously ligate and cut these vessels, thereby saving substantial time. An even more efficient maneuver made possible by the ultrasonic device is the single-bundle ligation of the entire upper pedicle without first isolating these vessels (Figure 43-2). This technique is faster, easier, and more efficient than the conventional method of managing the superior vasculature. In addition, it is theoretically safer, through ligation of the lower, terminal caliber branches of the ligated vessel(s), as well as moving this manipulation further from the external branch of the superior laryngeal nerve, which can course at or below the superior thyroid pole frequently.7 The gland can then be delivered through a smaller (≈ 2 cm) incision.
Electrothermal Bipolar Vessel Sealing System (LigaSure)
The combination of bipolar electrocautery and pressure allows less thermal energy utilization than traditional instrumentation. The LigaSure (Covidien, Boulder, Colorado) seals vessels up to 7 mm in diameter in an average of 2 to 4 seconds.8 Like the ultrasonic device, it may decrease surgical times, hospital stays, and hypocalcemia when compared to conventional thyroidectomy.9–12 A recent study compared the electrothermal bipolar, Harmonic device and traditional thyroid surgery and found surgical time to be equally reduced by use of either the electrothermal bipolar or the Harmonic. No difference was observed between these two modalities and conventional thyroidectomy in terms of nerve injury, bleeding, hypocalcemia, or hospital stay.13 Like the ultrasonic device, this instrument can be used for endoscopic or standard thyroidectomy approaches, so use of the instrument often depends on the surgeon’s preference and availability.
Laryngeal Nerve Monitoring
Although covered in considerable detail in other sections, it is appropriate to address laryngeal nerve monitoring here, particularly because it represents an important technological adjunct in modern thyroid surgery and is a natural complement to minimal access surgery (see Chapters 32, Surgical Anatomy of the Superior Laryngeal Nerve, and 33, Surgical Anatomy and Monitoring of the Recurrent Laryngeal Nerve).14
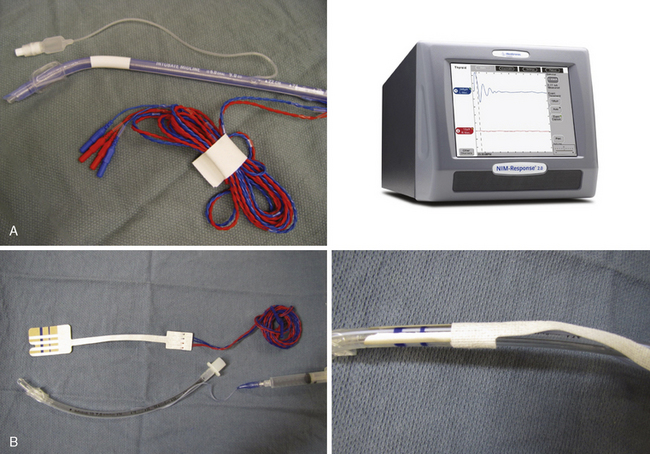
A number of reliable options for monitoring the integrity of the laryngeal nerves have emerged, with the device most commonly represented by an integrated electromyographic endotracheal tube (NIM 2.0, Medtronic Inc., Jacksonville, Florida). A lower-cost alternative is available in the form of surface electrode decals, which are affixed to a standard endotracheal tube (Neurosign and Nerveana), which requires the surgeon to adhere these correctly to the endotracheal tube (Figure 43-3). The principle is similar in each of these systems, in that electrodes detect electromyographic impulses from the thyroarytenoid muscles and relay them to the control unit, which presents them as an audible or visible signal. In some institutions, the monitoring is accomplished by a nonsurgical individual assigned to this task, or even a team of technicians (as is commonly done for multichannel neural monitoring systems as used for neurotologic or neurosurgical interventions).
High-Resolution Endoscopy
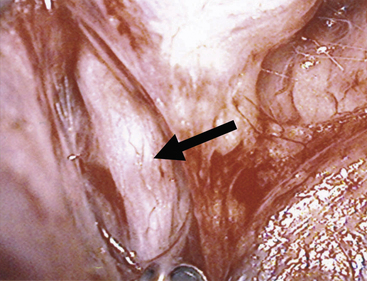
Endoscopes have accelerated the evolution of minimally invasive techniques across many surgical disciplines. The earliest endoscopes were uncomfortable for surgeons to use and obviated surgical teaching, because the surgeon had to look directly through the endoscope. Consequently, others in the operating room were unable to see what the operating surgeon was doing. As video imaging technologies developed, the ability to project magnified images not only allowed greater visualization inside cavities where direct visualization is impossible (Figure 43-4) but simplified the education of surgeons in training. Traditional methods of dissection and vessel ligation using ties and clamps proved difficult and time consuming when performed endoscopically. Concurrent with the widespread use of endoscopes were new technologies for dissecting and obtaining hemostasis. The combination of these technologies spawned the modern era of thyroidectomy, which includes both novel surgical maneuvers and the possibility of minimally invasive techniques.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


