Systemic Infectious and Inflammatory Diseases
Danielle S. Rudich
Krista M. Ramonas
Alan H. Friedman
VIRAL DISEASES
Herpes Simplex Virus
The herpes simplex virus (HSV) is a common cause of ocular, perioral, and genital infection in humans. The viral particle consists of a core of double-stranded DNA surrounded by a protein capsid and lipid envelope. HSV survives after the initial infection in latent form within sensory nerve ganglia. The virus may reactivate at any time, producing recurrent disease. HSV type 1 accounts for most herpes labialis and ocular herpetic infections whereas HSV type 2 causes genital herpes infections.1
HSV is a global disease and humans are the only known reservoir. HSV keratitis is a serious cause of blindness and is second in incidence only to trachoma in terms of corneal causes of blindness. HSV type 1 is transmitted primarily by oral secretions and HSV type 2 by genital secretions. Primary exposure to HSV type 1 commonly occurs in childhood. The age-adjusted seroprevalence rates in the United States from 1999 to 2004 were estimated to be 57.7% and 17%, for HSV1 and HSV type 2, respectively.2,3
The incubation period for HSV is from 2 to 14 days. Primary infection with HSV type 1 is often asymptomatic but may produce oral, eye, or skin lesions (Fig. 33-1). In children younger than age 5, a painful gingivostomatitis or pharyngitis with fever and cervical adenopathy is the most common presentation. HSV type 2 infections usually involve the glans penis and penile shaft in men, and the vulva, perineum, buttocks, cervix, and vagina in women.1 Fever, malaise, anorexia, and tender inguinal adenopathy may accompany the typical vesicular skin eruption. The ulcerated lesions are painful and may persist for several weeks before healing.
 Figure 33-1. Primary lesion of herpes simplex on the face of a child. |
Congenital HSV infection is recognized at birth by jaundice, hepatosplenomegaly, central nervous system abnormalities, bleeding diatheses, microcephaly, seizure disorders, fever, chorioretinitis, and skin vesicles. It must be differentiated from similar congenital syndromes caused by rubella, toxoplasmosis, and cytomegalovirus. Neonatal infection may be acquired in passing through the infected birth canal or by retrograde spread of the infection into the uterine cavity.
Less common presentations of HSV infection include primary infections of the skin of the fingers (whitlows). These can be seen in medical and dental personnel exposed to oral secretions infected by HSV type 1. In the general community this lesion is caused by HSV type 2 infection. HSV type 1 may also cause a skin infection that mimics herpes zoster, although the dermatomal distribution is not usually maintained and the pain is less severe. On rare occasions, herpes simplex can cause a necrotizing hemorrhagic encephalitis of the temporal lobes marked by rapid deterioration to coma and death.
Reactivation of HSV may be precipitated by fever, trauma, menstruation, emotional stress, or systemic illness. Burning, itching, and tingling tend to precede the appearance of skin vesicles in recurrent episodes of HSV type 1 and type 2. Systemic symptoms tend to be mild or absent, with the exception of recurrent adenopathy. The lesions appear similar to the primary infection and are frequently painful. The most frequent regional recurrences of HSV type 1 are on the vermilion border of the outer lip (herpes labialis) and in the eye (Fig. 33-2). Recurrences of HSV type 2 characteristically produce lesions on the penile shaft and glans in the male and on the labia and perineum in the female. Headache and aseptic meningitis are occasionally associated with a genital recurrence. Further recurrences may be seen at monthly or yearly intervals.
 Figure 33-2. Recurrent herpes simplex virus (HSV) type 2 on the face of a patient with aquired immune deficiency syndrome (AIDS). |
In primary ocular HSV infections, a severe follicular conjunctivitis with regional adenopathy is present. Vesicles may appear on the eyelid skin or lid margin, producing blepharitis (Fig. 33-3). Corneal involvement initially takes the form of a superficial punctate keratitis, which may progress to dendritic or geographic ulceration. Stromal infiltrates and uveitis are less common and relatively mild in primary disease. In uncomplicated cases, lesions usually heal completely in 2 to 3 weeks without scarring. Most cases of ocular HSV are recurrences. Recrudescent ocular herpes may take the form of dendritic or geographic ulcers, recurrent erosions, interstitial or disciform stromal keratitis, and anterior uveitis.4 HSV may also be an agent of retinitis and acute retinal necrosis (Fig. 33-4).
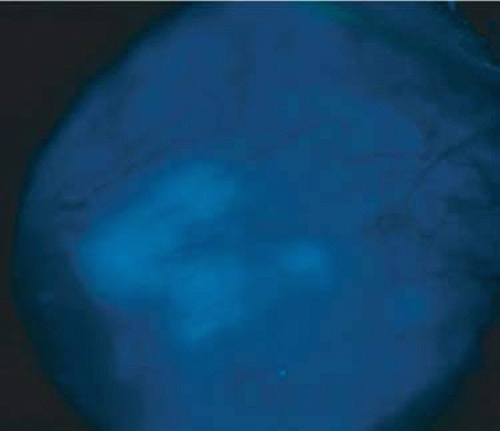 Figure 33-3. Lesions of herpes simplex virus (HSV) type 1 on the surface of the eye after topical fluorescein administration. |
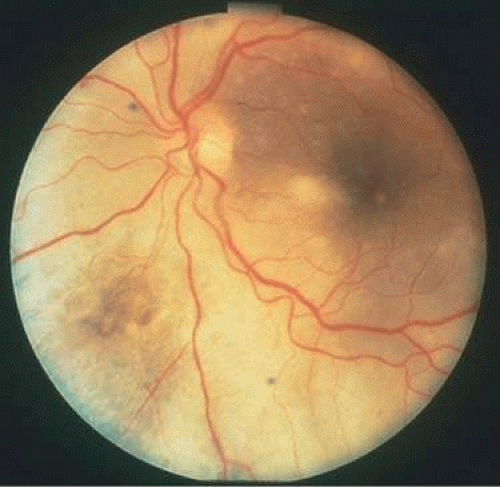 Figure 33-4. Acute retinal necrosis in the fundus. Note the widespread nature of the involvement. |
Clinical diagnosis of HSV infection can be made when the characteristic vesicular lesions are present. The diagnosis can be confirmed by isolation of the virus in tissue culture when necessary. Scraping the base of the lesions and Wright, Giemsa, or Papanicolaou stains will demonstrate the characteristic giant cells or intranuclear inclusions of herpesvirus infection. Polymerase chain reaction (PCR) has recently emerged as a diagnostic test for the presence of HSV 1 keratitis and to identify cases resistant to acyclovir.5
Most infections with HSV are mild or asymptomatic and require no specific treatment; however, antiviral therapy can be life saving in cases of neonatal herpes, disseminated infections, and herpes encephalitis. Famciclovir and valacyclovir are effective in reducing the pain, healing time, and duration of viral shedding in patients with first episode genital herpes and significantly shorten the clinical and virologic course in recurrent episodes. Immunocompromised patients with chronic progressive oral herpes have also demonstrated improved healing times and decreased viral shedding when treated with oral antivirals.6 Intravenous acyclovir is the drug of choice in the treatment of neonatal herpes infections and herpes encephalitis.
The corneal scarring caused by recurrent infection with HSV may be visually disabling and may require corneal transplantation. The Herpetic Eye Disease Study Group (HEDS) examined the short-term and long-term effects of oral acyclovir and topical steroids on epithelial keratitis, stromal keratitis, and iritis. Long-term oral acyclovir was shown to reduce the rate of recurrent HSV epithelial keratitis and stromal keratitis, especially in those who have had multiple prior episodes of stromal keratitis.7,8 Topical steroids are beneficial in preventing progression of stromal inflammation and shortening duration of stromal keratitis. Topical steroids should be given in conjunction with topical Viroptic (King Pharmaceuticals, Bristol, TN) in those with stromal disease or disciform keratitis, but steroids should be avoided in those with epithelial disease. The HEDS trial showed a beneficial trend in the treatment of anterior herpetic uveitis with oral acyclovir, but the trend failed to reach statistical significance.9 Nevertheless, practitioners routinely use oral acyclovir in addition to topical steroids plus a cycloplegic for herpetic-related uveitis. Topical steroids are often difficult to discontinue, and many patients require low-dose therapy for an indefinite amount of time. In recent years, resistance to acyclovir has been recognized as a treatment challenge. A recent study suggests the use of intravenous foscarnet in such cases.10
Varicella and Herpes Zoster
Varicella-zoster virus (VZV) is an enveloped DNA-containing virus that is morphologically indistinguishable from other members of the herpesvirus family. Typically, the primary infection manifests in children between the ages of 2 to 8 years of age, and is commonly known as the chickenpox. It is characterized by a generalized vesicular rash with insignificant systemic manifestations. Herpes zoster is a reactivation of VZV resulting in eruption of vesicles (shingles), which is usually accompanied by pain in the affected nerve distribution.11 Among adults in developed countries, seropositivity for HZV is seen in more than 95% of the population.12
Varicella occurs most commonly in the late winter and early spring. This highly contagious virus is presumably transmitted through direct person-to-person contact or by respiratory droplets. The clinical signs of varicella manifest about 2 weeks after viral exposure. A brief prodromal period of fever, lethargy, malaise, and headache may precede the development of a rash. The viral exanthem commonly starts on the scalp and the trunk as erythematous macules that progress to papules and subsequently vesiculate. Once the lesions crust over, after approximately 1 week, the virus is no longer contagious. Successive crops of new lesions appear so that all stages and sizes of lesions may be present at the same time. The mucosal linings of the mouth and conjunctiva can be involved. In uncomplicated cases, the active course is usually over in 7 to 10 days. The virus subsequently remains in a latent state within the dorsal root ganglion of the sensory nerves.
Herpes zoster infections are seen in patients of all ages and occur at all times of the year. Nearly all cases of herpes zoster have a history of prior exposure and are the result of reactivation of latent virus. The incidence of herpes zoster increases with age and is greater in immunocompromised persons. Pain and paresthesias characteristically precede the skin eruption by several days. The skin lesions morphologically resemble those of varicella; however, they tend to be larger and more bullous. The lesions respect the dermatomal distributions and do not cross the midline. The thoracic distribution nerves are most frequently involved followed by the trigeminal and cervical nerves.
Herpes zoster is most commonly diagnosed in immunocompromised patients, such as those with neoplastic disease, particularly lymphoproliferative disease, or human immunodeficiency virus (HIV). Over the course of a lifetime, approximately 20% to 30% of patients will demonstrate HZV with at least half of all those impacted at least 80 years old.13 Most patients younger than 60 years of age with uncomplicated herpes zoster will have complete resolution of their pain and skin lesions within 4 weeks. Allodynia and itching are potentially debilitating long-terms effects of postherpetic neuralgia and are more common in the elderly population.
Most ophthalmic involvement by varicella is mild.14 Crusting and scarring from skin lesions can lead to long-term complications such as ectropion, entropion, ptosis, trichiasis, distichiasis, and loss of skin pigmentation. Foci of inflammatory cells may appear on the bulbar conjunctiva, limbus, or peripheral cornea either during the acute illness or weeks to months afterward. Pocklike lesions along the eyelids often ulcerate and are associated with conjunctival hyperemia and hemorrhage and a mucopurulent discharge containing primarily neutrophils. Involvement of the cornea can result in superficial scarring with neovascularization. Occasionally, varicella can cause a punctate, dendritic, geographic, or disciform keratitis associated with a mild to moderate iridocyclitis. Unusual ocular complications of varicella include necrosis of the eyelids, interstitial keratitis, corneal melting, cataract, and optic neuritis. Congenital infection may result in microphthalmia, cataract, chorioretinitis, microcephaly, deafness, and cardiac abnormalities.
Of those patients with HZV, approximately 10% to 20% will develop herpes zoster ophthalmicus (HZO), which occurs when HZV erupts along the ophthalmic division of the trigeminal nerve.15 This is often preceded by a prodromal syndrome during which patients may develop eye pain. Approximately 50% of cases of HZO have ocular signs. (Fig. 33-5). Eighty-five percent of patients with cutaneous eruptions on the side of the tip or midportion of the nose (Hutchinson sign) will have ocular involvement. HZO can damage the anterior segment as well as the optic nerve, choroid, and retina. Episcleritis and scleritis with posterior involvement may develop. Cataracts and glaucoma are late complications related to the uveitis and long-term use of topical corticosteroid therapy.
 Figure 33-5. Facial involvement in a case of zoster. Note the characteristic strict segmental distribution of the lesions. |
Corneal complications occur in most patients with herpes zoster ophthalmicus. A punctate epithelial keratopathy with pseudodendrite formation is the earliest and most common lesion that occurs. Stromal infiltrates, disciform reactions, and rarely interstitial keratitis are also observed. Corneal sensation is reduced, and neurotrophic ulceration, corneal melting, or perforation may ensue. The finding of sectoral iris atrophy, unilateral anterior uveitis, and no evidence of prior keratitis are classic for herpetic uveitis. Extraocular muscle involvement with facial paresis has been observed.16
The acute retinal necrosis (ARN) syndrome, documented in both immunocompetent and immunocompromised patients, is most often caused by the herpes zoster virus, although occasionally it may be a result of herpes simplex infection. Floaters, vision loss, and pain are all symptoms of ARN. Areas of peripheral retinal necrosis and aggressive anterior chamber inflammation and vitritis are seen. In immunocompromised patients VZV, or more uncommonly CMV and HSV, may also take the pattern of progressive outer retinal necrosis (PORN) (Fig. 33-6). PORN differs from ARN in that the former is multifocal, localized to the outer retina, and is less often associated with vasculitis and vitritis. It is important to identify PORN as soon as possible given the risk of retinal detachment and the poor prognosis.
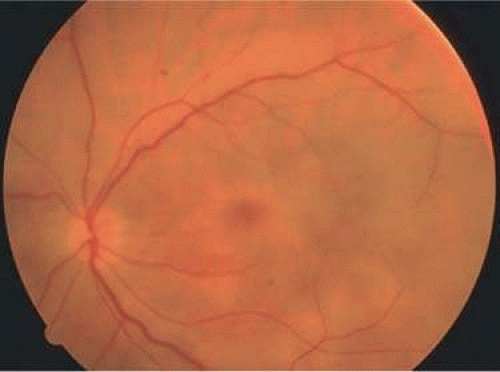 Figure 33-6. Fundus lesions of progressive outer retinal necrosis (PORN). Note the multifocal lesions. |
Laboratory diagnosis of varicella is usually not required as patients often give a history of having the chickenpox previously. Serologic confirmation can be obtained by demonstrating increasing anti-VZV antibody titers. Multinucleated giant cells and eosinophilic intranuclear inclusions can be demonstrated by Papanicolaou or other stains of smears from acute skin lesions.
The clinical diagnosis of herpes zoster is made in the presence of the characteristic vesicular lesions in a dermatomal distribution. Scrapings of the lesions demonstrate giant cells and intracellular inclusions. It is important to note that although most patients with herpes zoster are otherwise healthy, the possibility of an underlying systemic illness should be considered if the patient is young (i.e., younger than 50 years old) or the history suggests other systemic problems.
The treatment of varicella is primarily supportive, consisting of analgesia, antipyretics, antipruritics, and good skin hygiene to prevent secondary infection. The use of aspirin in children is to be avoided in view of the belief that it may predispose to Reye syndrome following varicella. Most eye disease is mild and self-limited and does not require treatment.
Antiviral agents, such as famciclovir and valacyclovir, have been shown to accelerate the resolution of the rash associated with HZV. Patients with HZO must be treated with antivirals. It is believed that treatment with famciclovir, acyclovir, or valacyclovir may speed recovery from postherpetic neuralgia. Valacyclovir and famciclovir are now preferred to acyclovir as first-line therapy for the treatment of zoster. They are well-tolerated drugs with few systemic side effects other than a requirement for reduced dosing in patients with renal failure. Oral corticosteroids also seem to have a beneficial effect in reducing acute pain and speeding cutaneous healing. They have not been shown to have an effect on postherpetic neuralgia.
Topical corticosteroids and cycloplegics are commonly used to treat the inflammation associated with herpes zoster ophthalmicus.14 Tear supplements, bandage contact lenses, surgical correction of lid abnormalities, and tarsorrhaphy may be necessary to promote the healing of epithelial defects. Vision-threatening pathologic processes such as chorioretinitis and optic neuritis should be treated aggressively with intravenous acyclovir and high doses of prednisone.
Treatment of postherpetic neuralgia is often challenging. Pain medications such as opiates are commonly used for analgesia. Routine analgesic drugs are generally ineffective. Cimetidine, colchicine, phenothiazines, and tricyclic antidepressants have been used with some success. Capsaicin cream and lidocaine patches may also be applied for local relief. Gabapentin, a neuroleptic medication, is often prescribed. The pain tends to slowly diminish and disappear over the course of 1 to 2 years but may be prolonged, especially in elderly patients. For those with severe intractable pain, intrathecal injection of methylprednisolone acetate once weekly for 4 weeks has recently been shown to provide relief.17
Vaccination against VZV has greatly reduced the number and severity of cases worldwide. The U.S. Food and Drug Administration (FDA) approved the vaccine for use in patients older than 60 years of age with a history of VZV-seropositivity in 2006.18
Cytomegalovirus Infection
Cytomegalovirus (CMV) is a herpes virus responsible for severe congenital malformations, a mononucleosis syndrome in young adults, and disseminated lesions in the immunosuppressed, especially retinal infection and pneumonia in patients with acquired immunodeficiency syndrome (AIDS). It is the most common reason for vision loss in patients with AIDS. AIDS patients with CD4 counts between 50 and 100 cells per microliter are particularly susceptible to CMV retinitis. If the retinitis is untreated the prognosis is very poor, often resulting in full-thickness retinal necrosis and blindness. Despite treatment, CMV retinitis often recurs in up to 50% of cases.19
In some parts of the world, up to 80% of the population is seropositive for CMV by 6 years of age. Approximately 1% of infections are congenital and 5% perinatal. Anti-CMV immunoglobulin (Ig) G is present in greater frequency in homosexual men, on the order of 80% to 90%. The virus may be transmitted via blood, cervical secretions, semen, and breast milk and as an intrauterine infection. Serologic testing for CMV is not routinely performed because of this frequent exposure in the general population. Immunocompetent individuals rarely manifest symptoms of the virus, which tends to remain in a latent state.
Approximately 10% of congenitally infected newborns have permanent sequelae. The full syndrome is manifested as hepatosplenomegaly with hepatitis and cirrhosis, maculopapular rash, purpura, hemolytic anemia, pneumonia, microcephaly, microgyria, encephalitis, chorioretinitis, pathologic bone fractures, and growth retardation. Otherwise asymptomatic children may develop late sensorineural hearing loss or mental retardation.
In normal older children and adults, the most common manifestation is an atypical mononucleosis, comprising fever and lymphocytosis with atypical lymphocytes. Lymphadenopathy and pharyngitis may be present, and rubelliform rashes occur. Heterophil antibodies are negative.
In the immunocompromised, especially organ transplant recipients and patients with AIDS, CMV commonly is responsible for serious clinical syndromes. It causes an interstitial pneumonia, resulting in dyspnea and dry cough, with interstitial infiltrates on the roentgenogram. Subacute encephalitis, enterocolitis, adrenalitis, and adrenal necrosis may be noted.
CMV retinitis was seen in up to 30% of patients with HIV prior to the widespread use of highly active antiretroviral therapy (HAART).20
Perivascular granular white or yellowish infiltrates with hemorrhage are typical. (Fig. 33-7) Minimal vitritis or anterior uveitis may be present. The posterior pole, including optic nerve, or peripheral retina may be involved, leading to rhegmatogenous retinal detachment. Optic neuritis may be retrobulbar. Resolution of retinal lesions reveals local retinal atrophy and pigment dispersion. Iridocyclitis may occur secondary to infection of ciliary processes. CMV retinitis in patients with AIDS is considered a poor prognostic sign in terms of life expectancy. Congenital CMV infection may also cause retinitis, as well as anterior uveitis, cataract, and optic atrophy. New foci of retinochoroiditis can develop in later years of congenital infection, and such infants require periodic re-examination as long as virus is shed in the urine.
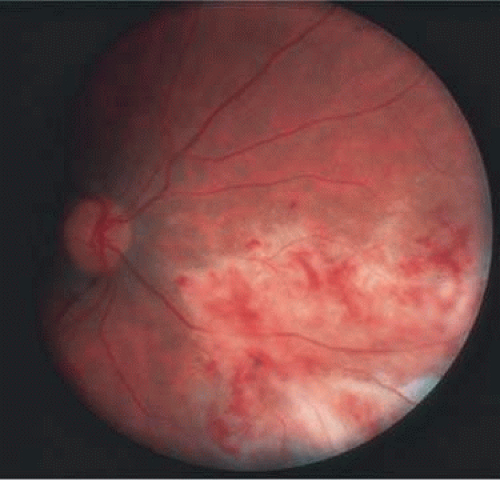 Figure 33-7. Cytomegalovirus retinitis in a patient with aquired immune deficiency syndrome (AIDS). Note the large area of retinal necrosis along with the perivascular distribution of the lesions. |
In the immunocompromised patient, other pathogens must be excluded, even in the presence of positive CMV cultures or serology. Tissue culture methods may take as long as 4 weeks. IgM antibody develops in primary infection and then disappears over 6 to 9 months, but it may reappear with reactivation of infection. The IgM test has unfortunately low specificity and sensitivity in infants and is less helpful than urine culture obtained at birth or in the first weeks of life.
Any cell type may be infected, appearing larger than normal (cytomegalic) and demonstrating eosinophilic intranuclear “owl’s eye” and smaller intracytoplasmic viral inclusion bodies, which are better seen with Giemsa or Papanicolaou stains (Fig. 33-8). Histologic examination of tissue specimens, including bronchoalveolar lavage fluid and urine, may be useful for diagnosis.
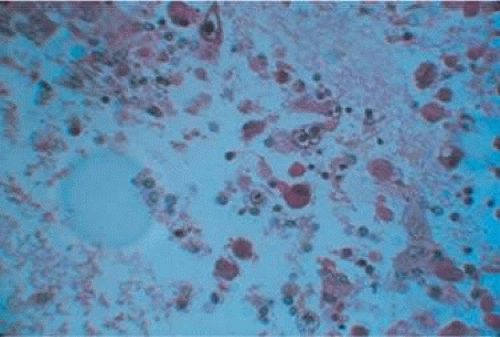 Figure 33-8. Typical lesion of cytomegalovirus (CMV) produces retinal necrosis with large cells possessing owl’s eye inclusions. |
Ganciclovir, or dihydroxypropoxymethyl guanine (DHPG), prevents DNA synthesis in infected cells. It is recommended for consideration in immunocompromised patients with retinitis, pneumonitis, enterocolitis, encephalitis; in infants with severe congenital or acquired disease; and in otherwise healthy patients with acute severe primary cytomegalovirus infection. It is effective in treatment of various CMV lesions, resulting in clinical stabilization or improvement. However, relapse almost always occurs when the drug is discontinued. An exception to this rule has been noted of late in patients who sustain elevated CD4 counts through the aid of HAART.21 The advent of HAART has greatly decreased the incidence of CMV retinitis, by up to 80% in some hospital centers.22 HAART has dramatically increased the life expectancy of patients with HIV, and it has also been shown to improve the outcome of patients with CMV retinitis. Ganciclovir, which halts the synthesis of viral DNA, was the first drug available to treat CMV. It is limited to intravenous use, and neutropenia develops in approximately 20% of patients. The agent that is most commonly used today is valganciclovir (Valcyte; Roche, Basel, Switzerland), an oral formulation that has been shown to slow the progression of CMV retinitis as compared to ganciclovir. It is used for both induction and maintenance therapy. Zidovudine, a reverse transcriptase inhibitor often used in the treatment of HIV, also results in neutropenia and should not be used in association with ganciclovir.23
Intravenous foscarnet, cidofovir, and fomivirsen are other anticytomegaloviral agents that are currently available.24,25 The primary toxicity of foscarnet and cidofovir is renal and requires strict monitoring of blood, urea, and nitrogen (BUN) and creatinine levels during treatment. After high-dose induction therapy, most patients require lifelong maintenance therapy for all anticytomegaloviral agents. In those who cannot tolerate the systemic side effects associated with intravenous therapy, intravitreal injection or intravitreal implantation of ganciclovir is a consideration.26 The ganciclovir implant is inserted into the pars plana and sutured to sclera. The implant can be changed after up to 32 weeks in the eye, as the CMV retinitis often flares once the implant no longer dispenses ganciclovir. Risks associated with the implant include operative complications.
Acquired Immunodeficiency Syndrome
AIDS is a disease caused by HIV, a virus that selectively targets CD4+ T lymphoctyes, leading to the development of secondary infections and tumors. CMV retinitis and other ocular manifestations of HIV-related disease are encountered frequently.
For purposes of reporting and surveillance, the Centers for Disease Control and Prevention (CDC) defines AIDS in terms of specific indicator diseases and laboratory evidence of HIV infection. Patients with AIDS are identified as individuals infected with HIV who have CD4+ T-cell counts less than 200 cells/μL or who have less than 14% CD4+ cells as well as one of the AIDS-defining conditions. These clinical conditions include disease entities such as recurrent pneumonia, invasive cervical cancer, and pulmonary tuberculosis, among other disease states.27
According to the CDC, as of the year 2006 approximately 1.1 million adolescents and adults currently living in the United States have been infected with HIV. New cases of HIV are estimated to be at least 56,000 annually in the United States.28 Worldwide incidence of HIV infection is a much more menacing burden because more than 33.4 million people have been reportedly infected with the virus as of 2008. There is a disproportionate rate of HIV among African Americans in the United States, who make up 12% of the overall population but 46% of HIV prevalence. HIV is more common among men, who outnumber women 2:1 in HIV prevalence in Europe and North America. Homosexual intercourse is still the most common route of infection. However. transmission of the virus is now more common in heterosexual sex, as well as through the sharing of contaminated needles in intravenous drug users. The introduction of antiretroviral therapies led to a decrease in AIDS-related mortality.29
The more widespread use of antiretroviral therapy in addition to public education campaigns has also impacted the rates of maternal to placental transmission of HIV. The United States has seen a drop in the infantile rate of infection from 130 cases in 1995 to 64 cases in 2007. There is currently no evidence for vector-borne transmission or infection via casual household contacts. The health care worker’s risk for infection via needle stick is approximately 3 in 1,000 punctures.30 The virus is very sensitive to heat, lipid solvents, and common antiseptics.
HIV was previously known as human T-cell lymphotropic virus type 3 (HTLV-III) and lymphadenopathy-associated virus (LAV). There are two known types of virus: HIV type 1, which causes AIDS, and HIV type 2, which can also lead to AIDS over a much longer period of time. HIV type 2 has been found in some African cases of AIDS and is believed to be decreasing in prevalence.31 HIV is a retrovirus, meaning it contains a reverse transcriptase enzyme that produces a double-stranded DNA copy (cDNA) from the virus RNA genome (Fig. 33-9).32 HIV infection involves attachment of viral envelope glycoprotein to the CD4 molecule present on T-helper (T4, OKT4, or CD4+) cell surfaces. The virus then fuses with the cell membrane, enters cytoplasm, loses its envelope, and reverse transcription of RNA to DNA occurs. Viral DNA becomes integrated into host cell DNA as latent provirus, in which state it may go unrecognized by the immune system. The proviral DNA can then be transcribed and translated, producing viral proteins and viral genome RNA, which assemble and bud through the host cell plasma membrane as new virions. Antigenic stimulation of lymphocyte activity appears to be important in conversion from latency to progressive infection.
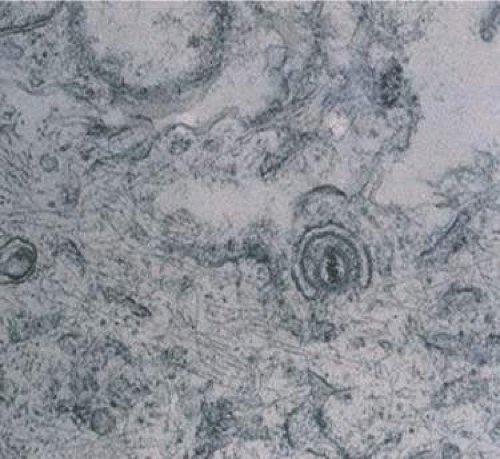 Figure 33-9. An electron micrograph of the human immunodeficiency virus type 1 (HIV-1) in the retina. |
HIV infection results in depletion of T4 cells, which are central to various forms of immune responsiveness. Risk of developing AIDS is inversely related to the absolute T4 cell count. Antigen-responsive T cells become selectively depleted or functionally impaired early in the course of AIDS. There is diminished helper function for B-cell responses, depressed cytotoxic and natural killer cell responsiveness, decreased blast transformation, and decreased lymphokine production. Infected patients’ B-lymphocytes spontaneously produce immunoglobulin, resulting in hypergammaglobulinemia, but are unable to produce specific antibody in response to new infections. Anergy is common. HIV also infects other cells that express the CD4 antigen, such as monocytes and macrophages, but is not cytopathic in these cells. HIV has been identified in brain capillary endothelium, oligodendrocytes, astrocytes, lymph node dendritic cells, Langerhans cells, intestinal mucosa, myocardium, tears, corneal epithelium, aqueous, vitreous, and retina.
Clinical manifestations of HIV are protean. Seropositive persons may be asymptomatic. Various acute HIV infection syndromes have been described. An acute mononucleosis-like syndrome, with fever, malaise, rash, lymphadenopathy, pharyngitis, myalgias, and arthralgias, has been noted after recent HIV exposure. Approximately 20% of patients with HIV initially present with neurologic manifestations; Bell palsy, shingles, aseptic meningitis, encephalitis, or focal lesions may be seen.33 HIV-wasting syndrome is a term encompassing features such as chronic fever, weight loss, and chronic diarrhea.
CDC-defined indicator diseases include HIV encephalopathy, HIV wasting syndrome, CMV disease other than liver, nodes, or spleen, progressive multifocal leukoencephalopathy, recurrent Salmonella septicemia, multiple or recurrent serious bacterial infections in children, extrapulmonary mycobacterial infection, disseminated histoplasmosis, disseminated coccidioidomycosis, chronic isosporiasis, lymphoid interstitial pneumonia or pulmonary lymphoid hyperplasia in children, primary brain lymphoma, and various non–T-cell non-Hodgkin lymphomas. Less specifically associated with HIV infection are manifestations of papillomavirus, molluscum contagiosum, VZV, Epstein-Barr virus, hepatitis B virus, chlamydia, gonorrhea, syphilis, Campylobacter, Pityrosporum, trichophyton, Aspergillus, Acanthamoeba, Entamoeba, Giardia, Strongyloides, basal cell carcinoma, squamous cell carcinoma, idiopathic thrombocytopenic purpura, cerebrovascular infarction, and intracranial hemorrhage.34,35,36,37
Pneumocystis carinii pneumonia once was the most common presentation of AIDS. It is typically of insidious onset, with features including dry cough, dyspnea, and a diffuse bilateral interstitial infiltrate evident on a chest roentgenogram. Typical multifocal fundus lesions have been described. They are yellow-white and have a characteristic pattern on fluorescein angiography (Figs. 33-10A–C). Diagnosis is made by demonstrating the protozoon via sputum induction, bronchioalveolar lavage, and transbronchial or open-lung biopsies. Treatment modalities include trimethoprim-sulfamethoxazole (TMP-SMX).38
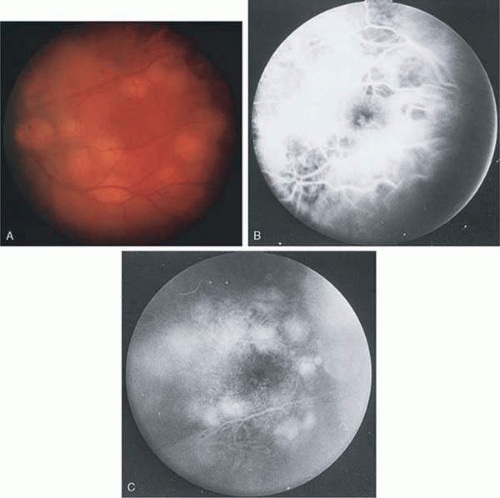 Figure 33-10. A. The retinal involvement of Pneumocystis carinii is manifested by multifocal, yellow-white lesions. B and C. On fluorescein angiography, the lesions fail to delineate in the early phase (B) but stain in the late phase (C). |
Kaposi sarcoma, caused by human herpesvirus 8, is the most common malignancy seen with HIV/AIDS.39 Cutaneous lesions are usually red or violaceous, palpable, and nonblanching papules, nodules, or plaques, often appearing on the hard palate, nose, eyelid, and conjunctiva (Fig. 33-11). Visceral and lymph node involvement is common and often clinically silent. Biopsy specimens show proliferation of small, incompletely formed blood vessels lined by unusually large endothelial-type cells, with extravasated red blood cells and infiltrates of spindle-shaped cells. Treatment of Kaposi sarcoma depends on the severity of the disease and includes surgical excision, radiation, intralesional chemotherapy, and topical alitretinoin. Systemic chemotherapy can be given in more widespread cases. HAART therapy is believed to reduce the tumor size.35,40
 Figure 33-11. The typical lesion of Kaposi sarcoma on the conjunctiva. |
Mycobacterium avium-intracellulare (MAI), M. kansasii, and other atypical mycobacteria are most commonly present as disseminated infections in patients with AIDS, with fever, sweats, chills, malaise, weight loss, and pulmonary and gastrointestinal symptoms. Signs of malabsorption, jaundice, skin lesions, and oral ulcers may be noted. Blood cultures, stool examination, and biopsy of various sites including lymph nodes, liver, gastrointestinal tract, skin, and bone marrow may be useful for diagnosis by smear or culture. Antituberculosis therapy may improve symptoms, but such infections are generally regarded as incurable in those with AIDS. The fundus lesions of MAI consist of discrete yellow-white choroidal foci (Figs. 33-12A and B).41 Extrapulmonary M. tuberculosis is an indicator disease and is covered elsewhere in this chapter.
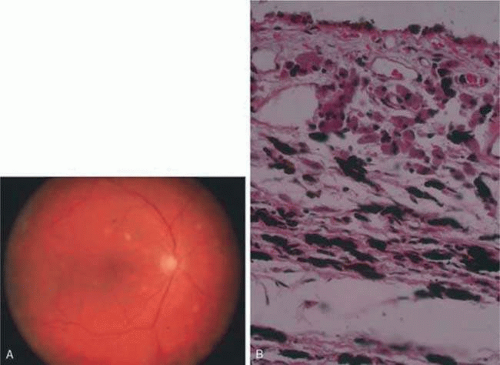 Figure 33-12. A. Mycobacterium avium-intracellulare (MAI) in the fundus produces multiple, discrete yellow intrachoroidal lesions. B. Histopathology of the choroidal infiltrate shows histiocytes laden with acid fast bacilli. |
Cryptosporidium species and Isospora belli are intestinal protozoa causing severe diarrhea in the immunosuppressed. Among patients with AIDS, it is more common in homosexual males and children. Stool specimens and intestinal and other biopsies may yield the organisms for diagnosis. Disease is usually self-limited but may be life threatening in the compromised patient. Therapy is mainly supportive. Spiramycin, α-difluoromethylornithine, and furazolidone have been used to treat cryptosporidiosis, and TMP-SMX for isosporiasis, all with limited success. Giardiasis and amoebic colitis are also seen in patients with AIDS.42
Progressive multifocal leukoencephalopathy is a chronic central demyelinating disease caused by the papovavirus JC (Jacob-Creutzfeldt virus). The disease may begin with subtle encephalopathic signs, later demonstrating various focal deficits. Visual loss is frequently reported. Computed tomography typically shows multiple hypodense nonenhancing lesions in white matter, and cerebrospinal fluid is usually normal or shows elevated protein. Diagnosis is made by brain biopsy. There is no effective therapy.43
Lymphocytic interstitial pneumonitis (LIP) occurs in approximately 30% to 40% of children with AIDS who have pulmonary disease.44 Epstein-Barr virus is speculated to play a role in the development of LIP. LIP is characterized by chronic infiltration of lymphocytes within the lungs, which leads to pulmonary symptoms such as cough and tachypnea. Pulmonary lymphoid hyperplasia (PLH) is a nodular variant of LIP. The LIP/PLH complex is yet another AIDS-related chronic pulmonary disease presenting with diffuse bilateral interstitial infiltrates. Biopsy demonstrates either nodular peribronchiolar lymphoid aggregates or diffuse alveolar and peribronchiolar lymphocytic and plasma cell infiltrates. Exacerbations may indicate superimposed infection. Corticosteroid therapy is recommended for patients with hypoxemia. LIP is an AIDS-defining condition so children with this diagnosis should be started on HAART medications.37,38,45
CMV, herpes simplex and zoster, candidiasis, cryptococcosis, toxoplasmosis, and other AIDS-related infections are described in detail elsewhere in this chapter.
The ophthalmic findings associated with AIDS are reviewed in another chapter of this section. As many as 25% of HIV-positive patients who do not receive treatment will have orbital and adnexal manifestations during the course of their illness. Commonly encountered anterior segment manifestations include keratitis sicca, infectious keratitis, iritis, herpes-zoster ophthalmicus, Kaposi sarcoma of the lid or conjunctiva, molluscum contagiosum, and conjunctival microvasculopathy. Posterior segment manifestations include retinal microvasculopathy, often noted as cotton-wool spots, cytomegalovirus retinitis, VZV retinitis, toxoplasmic retinochoroiditis, infectious choroiditis, and bacterial retinitis.41,42,46,47,48,49 Neuroophthalmic manifestations include papilledema, cranial nerve palsies, and visual field defects.50
Serologic diagnosis of HIV infection uses enzyme-linked immunosorbent assay (ELISA) kits for serum antibody detection. These assays are highly sensitive and may demonstrate false-positive results. Positive tests are therefore confirmed by repeat ELISA, followed by the Western blot test, which relies on the banding pattern of serum antibody to electrophoretically separated viral antigens.
Seroconversion usually occurs within 2 to 3 months, but may take much longer. Assay results will occasionally be read as indeterminate, indicating a reaction pattern that does not meet criteria for positivity, and retesting in several months is advised. Because of placental transfer of antibodies, a seropositive child younger than 15 months old must have other evidence of infection to support a diagnosis, such as clinical disease, positive HIV cultures, or HIV antigen testing. Serologic testing for HIV requires written informed patient consent in some locales, at least in part because of social stigmata associated with AIDS. Testing is now mandatory in the United States for blood donors, federal prisoners, military recruits and active-duty personnel, foreign-service officers, and immigrants to the United States.
In addition to HIV serodiagnosis, absolute T4 lymphocytopenia is the most useful laboratory finding related to HIV infection. A count of less than or equal to 400 cells/mm3 increases the risk of progression to AIDS.
Zidovudine (azidothymidine [AZT]) is a nucleoside analogue that inhibits viral reverse transcriptase. Zidovudine is virostatic, having no effect on latent virus. Taken orally, it has been shown to decrease symptoms, opportunistic infections, mortality rate, and HIV antigen values and to improve immunologic function in infected patients. The ability of HIV to undergo rapid antigenic variation of envelope glycoproteins, its low immunogenicity, and our incomplete understanding of what constitutes a protective immune response have contributed to the difficulty in developing an effective vaccine.
Several other antiretroviral agents known by their classification as nucleoside analogues, nonnucleoside analogues, or protease inhibitors have been introduced. Nucleoside analogues inhibit transcription of the HIV virus by blocking the enzyme reverse transcriptase, thereby inhibiting replication of the virus. Nucleoside analogues include Didanosine (ddI), Zalcitabine (ddC), Stavudine (d4T), and Lamivudine (3TC). Combivir, a combination of AZT and 3TC, is a popular choice in initial HIV therapy. Drugs known as nonnucleoside analogues, nevirapine and delavirdine, may be used in combination with nucleoside analogues. Due to high levels of resistance to AZT monotherapy, various combinations usually consisting of three different drugs are typically used. This new armamentarium of medications against the human immunodeficiency virus has dramatically lengthened life expectancy and improved quality of life.47
In 1996, the clinical introduction of the protease inhibitor (PI) class of antiretrovirals promised a dramatic breakthrough in the ability to demonstrate a significant impact on the amount of detectable virus in both blood plasma and lymphoid tissue (LT), the principal site of HIV replication and storage. It has now become standard practice to initiate HAART (highly active antiretroviral therapy) with combinations of PIs and other antiretrovirals to more completely and durably suppress viral replication. Some practitioners wait to introduce the protease inhibitors into the cocktail of medications until later stages of immunosuppression. The most commonly used protease inhibitors are saquinavir, indinavir, and ritonavir.
In addition to creating new antiretroviral medications, efforts are now focused on the development of a vaccination against HIV. Although some vaccinations have entered clinical trials, none are currently available to the public.51
Epstein-Barr Virus
Epstein-Barr virus (EBV) is a ubiquitous DNA virus that belongs to the human herpesvirus family. In early childhood the infection is usually subclinical; however, in adolescence and early adulthood it is the principal cause of infectious mononucleosis.
By adulthood more than 90% of the population demonstrates antibody to the virus. EBV is often transmitted by intimate contact with asymptomatic carriers. Live virus has been found to persist in the oropharynx for up to 18 months after clinical recovery from the initial infection. Infectious mononucleosis has also occurred after blood transfusions and open heart surgery.
EBV infection is characterized by the classic triad of fever, sore throat, and lymphadenopathy. Cervical adenopathy is present in 80% to 90% of patients. Splenomegaly occurs in 50% of patients. Other signs include hepatomegaly, jaundice, palatal petechiae, and rash. A wide spectrum of complications have been observed with EBV infection. These include anemia, thrombocytopenia, hepatitis, pericarditis, myocarditis, meningitis, encephalitis, optic neuritis, Guillain-Barré syndrome, and rarely, splenic rupture. Most patients recover spontaneously over a 2- to 3-week period, although rare fatalities have been reported.
Conjunctivitis is the most commonly reported of all ocular manifestations. Other manifestations include Sjögren syndrome, conjunctival lymphocytic infiltrates,52 dacryoadenitis,53 keratitis, oculoglandular syndrome, uveitis, choroiditis, retinitis, acute retinal necrosis,54 acute posterior multifocal placoid pigment epitheliopathy (APMPPE), papillitis, and ophthalmoplegia. Even in cases of retinal involvement, EBV rarely if ever leads to permanent loss of vision. Resolution of the posterior segment inflammation usually leads to return of normal acuity.55,56
EBV infection may be related to neoplasia in several settings. This includes Hodgkin lymphoma, posttransplant lymphoma, Burkitt lymphoma in patients of African descent, and nasopharyngeal carcinoma in Asians.57
Diagnosis of EBV may be made clinically and with serologic demonstration of heterophil antibodies. Serum antibody titers to EBV capsid antigen can also be specifically tested. Treatment of EBV is largely supportive. Corticosteroids may be useful in the treatment of severe thrombocytopenia or hemolytic anemia but are usually of limited value. Antiviral therapy such as acyclovir or interferon-α may be considered for slowly resolving EBV retinitis because both have been shown to inhibit EBV replication in vitro.
Mumps
The mumps virus is an encapsulated RNA virus in the paramyxovirus family that causes acute parotitis in children and young adults. The virus is transmitted in saliva and respiratory secretions. Most cases of mumps occur in the winter and early spring. The primary clinical features are fever and nonsuppurative salivary gland inflammation. Orchitis is present in 20% to 30% of postpubescent males. Meningitis, meningoencephalitis, pancreatitis, oophoritis, myocarditis, and sensorineural hearing loss are less common complications of mumps infection.58
A nonspecific conjunctivitis is a relatively common finding in patients with mumps infection and is occasionally hemorrhagic. Dacryoadenitis, episcleritis, scleritis, keratitis, optic neuritis, and more recently reported acute posterior multifocal placoid pigment epitheliopathy59 and neuroretinitis60 may be seen after mumps.
The diagnosis of mumps can usually be made based on clinical findings. The virus can be cultured from saliva or spinal fluid, and seroconversion can be documented by various assays. Efforts at preventing infection are primarily to avoid the complications of orchitis and encephalitis. Vaccination with live attenuated virus successfully produces immunity in approximately 90% of subjects. Since the licensing of the vaccine in 1967, there has been a more than 99% decline in the annual incidence of mumps in the United States.58 Prior to institution of the vaccine, epidemics of mumps occurred every 2 to 5 years. Mumps is now so rare that only 751 cases were reported to the CDC in 1996. Treatment of mumps is symptomatic and supportive with analgesics and antipyretics. Topical steroids have been shown to be effective in the treatment of corneal endotheliitis.61
Measles
Measles is a highly contagious viral exanthem caused by an encapsulated single-stranded RNA virus in the paramyxovirus family. The illness is characterized by a prodromal period of malaise, with conjunctival and respiratory irritation followed by a maculopapular rash. Measles has a worldwide distribution. Its incidence has diminished in developed countries as a result of vaccination programs. However, measles still remains a serious cause of childhood illness, blindness, and mortality in developing countries. The World Health Organization estimates that 30 million children contract measles each year.
Measles is transmitted by direct contact with respiratory secretions. The attack rate exceeds 75% among those in contact with the infection. The prodromal symptoms develop 8 to 12 days after exposure and precede the rash by 2 to 4 days. The erythematous maculopapular rash initially presents on the face and neck but spreads to the rest of the extremities and trunk within a few days. Bright red spots with a bluish white center (Koplik spots) appear on the buccal mucosa 1 to 2 days before the exanthem and are considered pathognomonic of measles.62
Ten to thirty percent of patients with measles develop complications including diarrhea, pneumonia, malnutrition, otitis media, keratoconjunctivitis, and blindness. Although rare, measles encephalitis, thrombocytopenia purpura, and myocarditis lead to significant morbidity and mortality. Subacute sclerosing panencephalitis (SSPE), a rare complication, is believed to be caused by infection of the brain by the measles virus, leading to a slow degeneration of intellect and motor function that culminates in decorticate rigidity and death. The measles virus has been isolated within the retina of patients with SSPE. Optic atrophy, optic neuritis, measles retinopathy, and retinal vascular occlusion have been described with this condition.63
Other ocular findings in measles include a nonspecific conjunctivitis with follicles or papillae and conjunctival hyperemia. An occasional Koplik spot may be seen. In severe cases, punctate erosions of the bulbar conjunctiva are accompanied by a mucopurulent discharge. Subepithelial corneal infiltrates that stain with fluorescein may also appear transiently during the illness.64 Patients with poor nutritional status or vitamin A deficiency may develop corneal ulceration or perforation.
A clinical diagnosis of measles can be made in patients with the characteristic prodrome and morbilliform rash. Laboratory confirmation is obtained by demonstrating seroconversion.
Treatment of patients with measles is supportive. Secondary bacterial infections and dehydration should be treated aggressively. The live attenuated virus vaccine gives a 98% conversion rate under ideal conditions. After immunization, fever and a mild rash may develop; rare cases of encephalitis and uveitis have occurred.65 No therapy is required for the conjunctivitis. Studies have shown that high-dose vitamin A supplements help to prevent the ocular complications of measles, including corneal xerosis, corneal ulceration, and keratoconjunctivitis.
Rubella
Rubella (German measles) is a childhood exanthem caused by an encapsulated RNA virus of the togavirus group. The viral illness may be totally asymptomatic in adults or present with a mild self-limited fever, morbilliform rash, and lymphadenopathy. The most significant aspect of rubella infection is in its effect on the fetus. Prenatal infection may result in miscarriage, stillbirth, or the congenital rubella syndrome.
Since 1969, the year of rubella vaccine licensure, the incidence of rubella infection and congenital rubella have declined 99% in the United States. Most cases occur in the spring, the highest incidence being among children. Patients are most contagious in the week prior to the eruption of the rash and transmit the virus through respiratory droplets. Infants with congenital rubella shed large quantities of virus in their body fluids for months and may retain viable virus in the lens for years after the initial infection.66
Despite immunization programs, 10% to 20% of young adults remain susceptible to rubella infection and limited local outbreaks continue to occur in settings such as schools and military bases where groups of susceptible persons are in close contact.
Typically there are no prodromal symptoms of rubella infection in children; however, adults may experience malaise, fever, and anorexia for several days before the rash erupts. Ocular features generally include conjunctivitis and epithelial keratitis. Lymphadenopathy occurs most commonly in the posterior auricular, posterior cervical, and suboccipital lymph nodes; generalized adenopathy and splenomegaly occasionally are seen. The exanthem of rubella begins on the forehead and face and spreads downward to the trunk and limbs. The lesions are discrete and maculopapular but may coalesce to form a diffuse erythema. Petechial lesions may erupt on the soft palate (Forchheimer spots). In young women, a self-limited arthritis involving the wrists, fingers, and knees may accompany the rash and occasionally persists after the other manifestations of rubella have disappeared.67
Rubella infections that occur early in gestation are associated with the greatest risk of fetal damage; however, infection in the third trimester may still cause damage. Maternal infection in the first 2 months of pregnancy results in a 40% to 60% chance of multiple congenital anomalies or fetal death. Congenital heart disease, cataracts, and deafness are the classic triad of the congenital rubella syndrome; however, there are many other commonly recognized complications of prenatal rubella infection (Fig. 33-13). Encephalitis, microcephaly, mental retardation, intrauterine growth retardation, thrombocytopenic purpura, hepatosplenomegaly, obstructive jaundice, interstitial pneumonitis, myocarditis, and radiolucent bone lesions are all possible sequelae of congenital rubella infection.66 The classic salt-and-pepper retinopathy occurs less commonly (Fig. 33-14) but may be noted to show progression. Other ocular findings include congenital cataracts, microphthalmia, and glaucoma. Ocular disease and hearing loss frequently occur together, and glaucoma is frequently associated with microphthalmos.68 The rubella virus has also been linked to Fuchs heterochromic cyclitis in some studies.69
 Figure 33-13. A patient with the congenital rubella syndrome. Note the hearing aids, left esotropia, left microphthalmos, and cataract. |
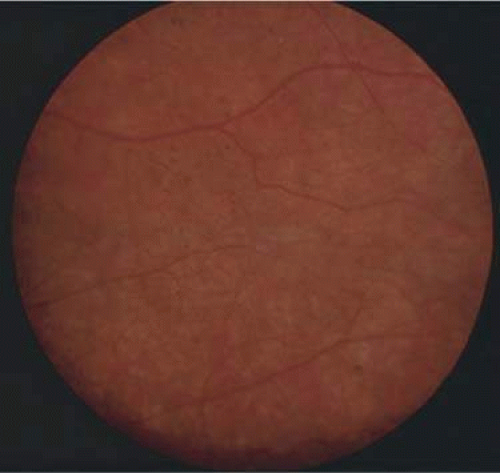 Figure 33-14. The classic salt-and-pepper fundus of congenital rubella. |
The devastating fetal damage caused by maternal rubella infections can be prevented only through rigorous immunization programs. All susceptible women of childbearing age should be vaccinated 3 months before a planned pregnancy or in the postpartum period. As a result of immunization programs, there have been no major outbreaks of rubella in the last 35 years.
Postnatal rubella infection may go undetected because of its mild and nonspecific symptomatology. The diagnosis can be made by culturing virus from the throat or by demonstrating rising antibody titers to rubella-specific IgG. When suggestive birth defects are present, the diagnosis of congenital rubella requires either viral isolation from the throat, urine, or other body secretions or serologic evidence of infection.
BACTERIAL DISEASES
Chlamydia Trachomatis Infection
Chlamydiae are Gram-negative intracellular parasites dependent on host cells for energy-related molecules. Chlamydia trachomatis infection is the most common sexually transmitted disease in industrialized countries and the most common cause of eye infection worldwide. It is also an important cause of infant pneumonia and may be related to Reiter syndrome.
Nongonococcal urethritis (NGU) is the most common manifestation of genital C. trachomatis infection in males, characterized by mucoid or mucopurulent discharge, dysuria, and pruritus. Urethral infection is often mild and may be asymptomatic. Twenty percent of male cases of gonococcal urethritis have simultaneous chlamydial infection. Postgonococcal urethritis due to chlamydia may develop 2 to 3 days after successful treatment of gonorrhea. Chlamydia proctitis is not uncommon in male homosexuals. Epididymitis and Reiter disease may be complications.
Cervicitis is the most common genital manifestation in female patients. Most women are asymptomatic. Mucopurulent discharge occurs in 40%. Chlamydia infections cause one third of cases of acute salpingitis (pelvic inflammatory disease), often with only mild symptoms of abdominal pain and only 5% positive cervical smears. The long-term consequences of pelvic inflammatory disease include ectopic pregnancy, chronic pelvic pain and infertility.70 Four to twenty-one percent of pregnant women may have C. trachomatis infection of the cervical canal, thus exposing the newborn at birth. Inclusion conjunctivitis may occur after an incubation period of 6 to 19 days. Thirty to forty percent of pneumonias in the early months of life are because of Chlamydia, and approximately half of such children also have conjunctivitis.71
Lymphogranuloma venereum is a sexually transmitted infection of C. trachomatis serotypes L1, L2, and L3, which affects lymphatic tissue. The primary lesions of lymphogranuloma venereum are small painless papules, vesicles, or ulcers of the penis, vulvar or anorectal areas, and manifest 3 to 12 days after the initial exposure. Painful massive regional lymphadenopathy becomes suppurative, and draining fistulas develop within weeks of the primary lesion. Chronic lymphedema can lead to elephantiasis if lymphatic vessels are obstructed, rectal stenoses, strictures, and fistulas.72
Trachoma is a chronic infectious keratoconjunctivitis caused by C. trachomatis serotypes A, B, and C. It affects approximately 300 to 500 million persons and has led to blindness is about 5.9 million. The infection is commonly seen in parts of developing Africa, the Middle East, and Asia, but also may be seen in natives of the American Southwest. In the early phase, trachoma causes an acute conjunctivitis. Classic findings include conjunctival follicles and papillae. During this acute phase limbal follicles may form, leading to the development of corneal pannus. Regression of the limbal vessels leads to corneal indentations named Herbert pits. Severe scarring of the cornea and conjunctiva after repeated episodes of inflammation often leads to entropion, trichiasis, and corneal opacifications.73,74 C. trachomatis serotypes D through K are the most common cause of genital infections and infectious neonatal conjunctivitis in the United States. Adult and neonatal inclusion conjunctivitis and trachoma are reviewed elsewhere in these volumes.
Gram stain does not detect chlamydia. Tissue culture techniques are most sensitive. These cultures require special transport medium and refrigeration of the specimen and 48 to 72 hours of incubation with the cell culture prior to specific immunofluorescence staining for diagnosis. The McCoy cell culture using fluorescent antibody test for staining has become the gold standard.71 Direct Giemsa stained smears have a relatively low yield, with sensitivity varying from 50% to 90%, demonstrating dark blue or purple intracytoplasmic inclusions in a field of polymorphonuclear leukocytes, lymphocytes, and other cell types (Fig. 33-15). The microimmunofluorescent antibody stain for smears has approximately 90% sensitivity and 100% specificity compared to cultures. Serum antichlamydial IgM may aid diagnosis in neonatal pneumonia, and high titers of antichlamydial IgG may be found in complications of genital infection such as acute salpingitis. In addition to the McCoy cell culture, polymerase chain reaction may also aid in detection of C. trachomatis DNA.
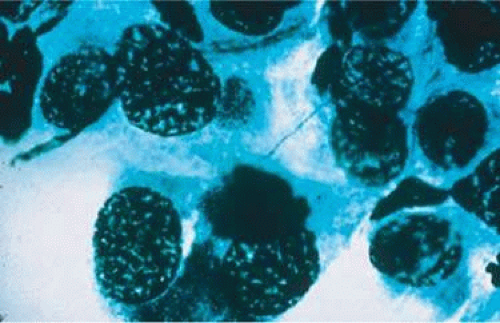 Figure 33-15. A positive Giemsa stain in a case of chlamydial conjunctivitis. |
Therapy for genital chlamydia infection is administration of tetracycline, doxycycline, or erythromycin for 2 to 3 weeks. Asymptomatic sexual contacts should be treated as they are likely to harbor genital chlamydial infections. Treatment failures are rare.
Tuberculosis
Mycobacterium tuberculosis is a bacterium that causes infection through inhalation of aerosolized droplets filled with the organism. An asymptomatic pulmonary granuloma may develop and reactivate at any point, particularly when accompanied by diseases such as HIV, chronic renal failure, and diabetes mellitus.
Ocular involvement, seen in 1% of cases of TB, most commonly occurs after reactivation in the lung or alimentary tract and is thus referred to as secondary TB (Fig. 33-16). Primary ocular involvement of TB is rare and is almost always limited to the cornea and conjunctiva. Conjunctival TB has been reported as a chronic unilateral conjunctivitis with a conjunctival mass or ulceration associated with regional lymphadenopathy. Although also rarely seen, conjunctival phlyctenulosis has been found to be associated with tuberculoprotein hypersensitivity. Biopsy and culture proven scleral TB was reported in the literature in 1976 and 1989. Other ocular manifestations of TB include anterior uveitis, either granulomatous or nongranulomatous, choroiditis, vitritis, and choroidal tubercles/tuberculoma.75 TB been linked to Eales disease, a retinal vasculitis characterized by vitreous hemorrhages and retinal neovascularization, seen in young men.76
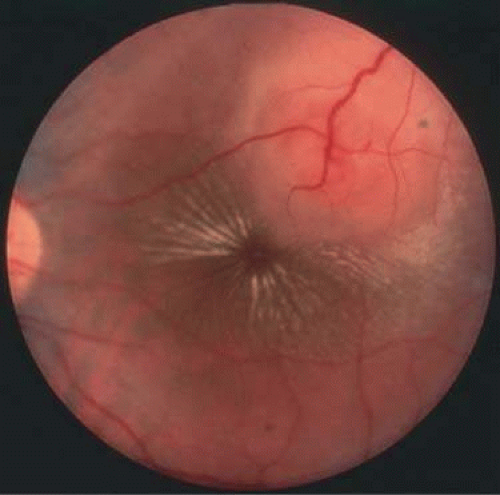 Figure 33-16. A choroidal tubercle in a patient with miliary tuberculosis. |
The gold standard for diagnosis of intraocular tuberculosis is demonstration of acid-fast bacilli in fluid or tissue sample either by direct smear and culture, polymerase chain reaction (PCR), or ELISA (Fig. 33-17). Tuberculin skin testing is useful but is less specific and must be interpreted based on the size of induration in correlation with socioeconomic status, immune status, and contact history of the patient. The test consists of an intradermal injection of purified protein derivative (PPD) from tubercle bacilli. Two recently developed tests, T-SPOT TB and QuantiFERON-TB Gold are more specific than tuberculin skin testing. The tests measure levels of interferon γ produced after exposure to tuberculosis antigens.
 Figure 33-17. Acid-fast bacilli are present in the biopsy of a lesion. |
Classic histopathology consists of caseating granulomatous inflammation in a zonal distribution. The noncaseating tubercle may be present but is less specific (Fig. 33-18). The organism is acid-fast, meaning that it does not decolorize with acid alcohol after staining with basic fuchsin, appearing as bright red, long thin rods. A definitive laboratory diagnosis of intraocular tuberculosis may be made via anterior chamber tap, vitreous or chorioretinal biopsy depending on the site of inflammation. The PCR may be helpful in making the diagnosis.
 Figure 33-18. Histopathologic examination of an enucleated eye demonstrates a caseating focus in the choroid. |
Treatment of tuberculosis consists of rifampin, ethambutol, and isoniazid for 2 months followed by rifampin and isoniazid for 4 months. Pyridoxamine may be added to the regimen to prevent isonicotinic acid hydrazide (INH)-induced peripheral neuropathy. Monitoring the response to treatment should be done with sputum cultures. By the end of the third month of treatment most patients are culture-negative. Those who remain culture-positive at the end of 6 months should be considered treatment failures. In a uveitic patient with a positive PPD, a 2-week therapeutic trial of INH may aid in the diagnosis. If ocular inflammation decreases, a full course of anti-TB treatment is used.77,78
Prevention of tuberculosis is through rapid diagnosis, bacille Calmette-Guérin (BCG), vaccination, and preventative chemotherapy. BCG vaccine is not used in the United States but is recommended in countries where the prevalence of TB is high. The vaccine is from a strain of live attenuated bovine tubercle bacilli used to induce an immune response to M. tuberculosis. The vaccine varies greatly in efficacy from 0% to 80%. Patients who have received the BCG vaccine will have a false-positive PPD skin test reactivity.
Lyme Disease
Borrelia burgdorferi is a tick-borne spirochete that produces Lyme disease. Lyme disease was originally named in 1977 when arthritis was observed in a group of children in Lyme, Connecticut. B. burgdorferi is now considered endemic in more than 15 states in the United States, as well as in Europe and Asia. In 1999, 16,273 cases of Lyme disease were reported to the CDC, more than 90% from the states in the northeastern and mid-Atlantic region of the United States. Although B. afzelii and B. garinii also produce Lyme disease, only B. burgdorferi has been found in the United States.79
The vector for the transmission of the bacterium B. burgdorferi to humans is the black-legged Ixodes tick. Ixodes scapularis are most often found in the northeastern United States, and I. pacificus is more commonly found in the western United States. The Ixodes tick is very small, said to be the size of a pinhead, and the tick bite therefore often goes unnoticed. In the early stages of the disease, several days to weeks after the bite, a slowly expansile area of erythema with an area of central clearing known as the bull’s-eye rash or erythema migrans appears. The size of the lesion varies from 5 to 15 cm. Nonspecific symptoms of malaise, fever, myalgias, and arthralgia accompany the rash in the initial stages of infection. While often difficult to diagnose because of the subtlety of findings, this stage is most susceptible to treatment with antibiotic therapy. Stage two occurs as spirochetes spread from the site of initial infection via cutaneous, lymphatic, or blood-borne routes. Signs of early disseminated infection include development of multiple smaller annular skin lesions and involvement of the cardiac, central nervous, and musculoskeletal systems. Cardiac involvement is rare, involving less than 8% of untreated cases, and includes atrioventricular block, pericarditis, and cardiomegaly. Neurologic involvement, also known as neuroborreliosis, is seen in 15% of cases and may cause meningitis with neck stiffness and headaches, cranial neuropathy with facial nerve palsy, forgetfulness, and sleep disturbances. The late disseminated stage is characterized by intermittent arthritis and neurologic symptoms, such as encephalopathy and polyneuropathy. Some patients continue to have arthritis several months after treatment for Lyme disease. A subset of patients experience posttreatment chronic Lyme disease, a diagnosis given to patients with unexplained symptoms lasting at least 6 months after treatment for Lyme disease. Fatigue, arthralgias, memory disturbances, and myalgias are all characteristics of this disorder and no effective treatment has been found to date.80
Lyme disease can involve nearly all structures of the eye. The most common early manifestation is conjunctivitis, occurring in approximately 11% of patients; however, most ocular manifestations of Lyme disease are associated with late stages of the disease. Follicular conjunctivitis, episcleritis, trigeminal neuralgia, and retinal vasculitis have been reported in an observational case series of 10 patients with Lyme borreliosis.81 Other findings include anterior uveitis, multifocal choroiditis, optic disc edema, and intermediate uveitis (Fig. 33-19).82
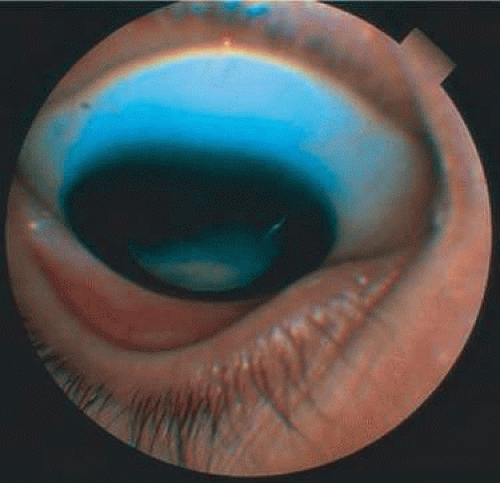 Figure 33-19. Intermediate uveitis in a case of Lyme borreliosis. |
The diagnosis of Lyme disease is made by clinical presentation and serology. It is, however, appropriate to treat based on clinical findings and a history of a known exposure. CDC recommendations for serologic testing include an ELISA followed by a Western blot. Antibodies are often present for years after exposure to infection, regardless of treatment of the disease. Therefore, seropositivity must not be mistaken for active disease. Treatment recommendations for Lyme disease include a 2- to 3-week course of doxycycline, with substitution with amoxicillin for children and pregnant women.83 Patients with evidence of neurologic abnormalities should undergo a more intensive 2- to 4-week course of intravenous ceftriaxone.
Syphilis
Syphilis is a sexually transmitted disease caused by the bacterium Treponema pallidum. A primary skin lesion known as a chancre is followed 3 weeks to 6 months later by hematogenous dissemination of the organism, a stage known as secondary syphilis. Secondary disease manifestations are broad and nonspecific ranging from a maculopapular rash and generalized mucocutaneous lesions to malaise, fever, and painless lymphadenopathy. Less commonly, gastrointestinal, hepatic, and renal disease have been reported. Secondary syphilis generally resolves within months but may recur, often within the same year. Late sequelae involving the central nervous system and the aorta are referred to as the tertiary stage of syphilis. Approximately 30% of untreated patients develop tertiary syphilis, but less than 1% develop clinical signs of neurosyphilis. Neurosyphilis can result in a cerebral vasculitis producing symptoms of transient ischemia or infarction, general paresis, or chronic encephalitis producing progressive dementia and tabes dorsalis. Tabes dorsalis is a progressive spinal cord lesion involving the posterior columns and dorsal nerve roots resulting in the classic broad-based foot slapping gait. The average interval from infection to central nervous system involvement is 5 to 10 years for meningovascular disease, 20 years for general paresis, and 25 to 30 years for tabes dorsalis. Progression to neurosyphilis may be accelerated in patients with AIDS.84
The clinical manifestations of congenital syphilis are as broad as those of acquired syphilis. The first sign is often rhinitis, followed by mucocutaneous lesions resembling secondary syphilitic disease in adults. Inflammatory skeletal lesions are common, as are lymphadenopathy, hepatosplenomegaly, jaundice, anemia, thrombocytopenia, and leukocytosis. Neonatal death may occur from pulmonary hemorrhage, secondary bacterial infections, or severe hepatitis. Stigmata include widely spaced peg-shaped teeth (Hutchinson teeth), frontal facial bossing, saddle nose, maxillary hypoplasia, saber shins, and linear scarring around body orifices known as rhagades.
Ocular involvement may occur in all three stages of syphilis. Conjunctival chancre formation may occur in primary syphilis. Nonspecific conjunctivitis, episcleritis, and scleritis may occur in secondary syphilis. Syphilitic interstitial keratitis is usually associated with congenital infection but may also be acquired. Iritis, dilated iris capillaries, iris nodules, and chorioretinitis including the classic salt-and-pepper pigmentary degeneration of the fundus are seen in congenital disease (Fig. 33-20).85 Yellowish and gray placoid lesions in the fundus of HIV patients are seen in acute syphilitic posterior placoid chorioretinitis. These lesions appear as leopard-spot–like changes on fluorescein angiogram, which distinguishes them from the lesions of serpiginous choroiditis and posterior multifocal placoid pigment epitheliopathy.86 Neuroophthalmic findings such as cranial nerve palsies are seen early in the disease course, whereas optic neuropathy is seen in secondary syphilis. The Argyll Robertson pupil, seen late in the course of the disease, is characterized by irregular, unequal, and miotic pupils.87
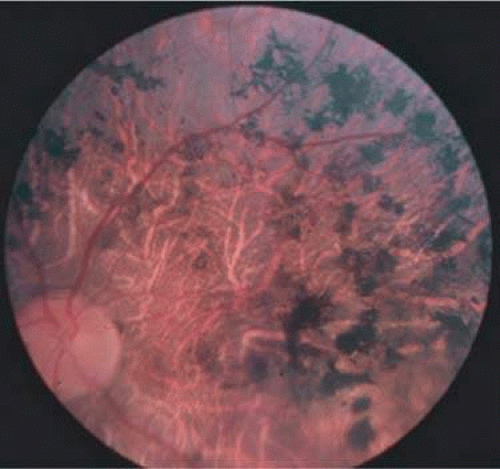 Figure 33-20. Fundus pigmentary changes in a case of secondary syphilis. |
The introduction of penicillin drastically reduced the incidence of syphilis. From 1990 to 2000 the rates of primary and secondary syphilis decreased by nearly 90%. An increase in rates among men has recently been noted. Reported cases of syphilis were 2.5 per 100,000 population in 2003.87
Diagnosis of syphilis is difficult at times and often requires a high level of suspicion because of the varied manifestations of the disease. Syphilis can be diagnosed by examination of material from infectious sores by dark field microscopy (Fig. 33-21). The organism may be demonstrated with silver stains or direct fluorescent antibody microscopy. Pathology specimens show mononuclear infiltration particularly around blood vessels. The easier and more commonly used route of testing is serologic. Serologic tests can be categorized as either treponemal or nontreponemal. Venereal Disease Research Laboratory (VDRL) and rapid plasma regain (RPR) are nontreponemal tests that detect antibodies to cardiolipin cholesterol antigen. These tests are best suited for general screening, but a positive result must be confirmed with a treponemal test such as fluorescent treponemal antibody absorption test (FTA-ABS).88
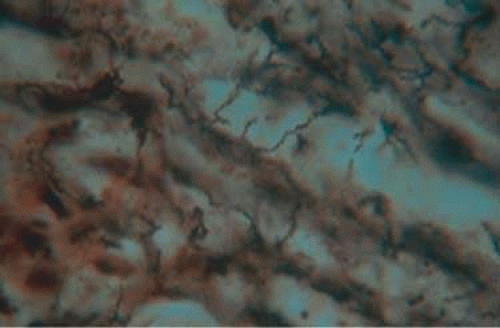 Figure 33-21. Histopathologic examination of silver-stained conjunctival lesion revealed spirochetes. |
Penicillin G is the drug of choice for syphilis. Primary, secondary syphilis, and early latent syphilis may be treated with a one-time intramuscular injection. Recommended treatment for latent syphilis, late latent syphilis, and tertiary syphilis is penicillin G, 2.4 million units intramuscularly weekly for 3 weeks. Neurosyphilis requires treatment with 18 to 24 million units of intravenous aqueous crystalline penicillin every 4 hours for 10 to 14 days or intramuscular procaine penicillin with oral probenecid. The CDC advises HIV testing for all patients with neurosyphilis and evaluation of the cerebrospinal fluid (CSF) every 6 months.86 Oral doxycycline or tetracycline has been recommended for those with a documented penicillin allergy.88 Steroids, either periocular, topical, or systemic, may be used as an adjunctive agent in the treatment of ocular syphilis.87
Leptospirosis
Leptospirosis is a disease common to tropical climates that is caused by the spirochete Leptospira interrogans. Rodents and wild animals are considered reservoirs of this disease. Animals are infected via water or soil that is contaminated with the spirochete. Humans acquire the disease through skin or mucosal contact with infected urine or animal tissue. The spirochetes enter the bloodstream, leading to an acute febrile reaction, headache, severe myalgia, and fatigue. Leptospira organisms are present in the blood and cerebrospinal fluid during this period, which lasts 4 to 7 days. Defervescence and a decrease in symptoms occur over the next few days. A second (immune) phase follows, typically 3 to 6 months after inoculation, with return of fever and symptoms. Ocular involvement occurs during the second, or immune, phase of the disease. Conjunctival injection and subconjunctival hemorrhages may be present. Unilateral or bilateral uveitis, occasionally with hypopyon, has been reported with leptospirosis. Uveitis recurs in some patients, whereas some patients experience a single episode. Anterior, intermediate, and panuveitis have been documented. The prognosis for this uveitis is generally good. Common complications include cataract formation and glaucoma induced by treatment with steroids.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


