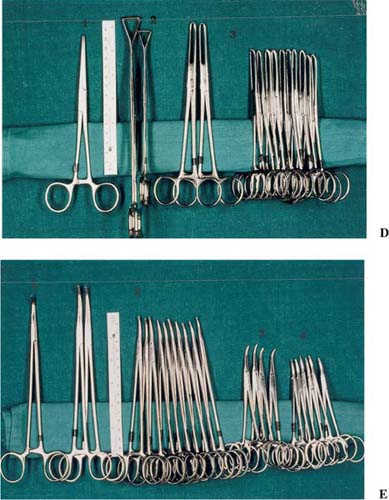
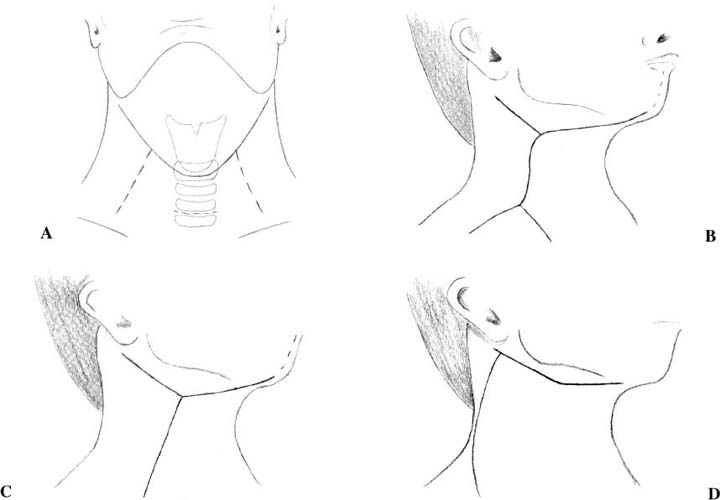
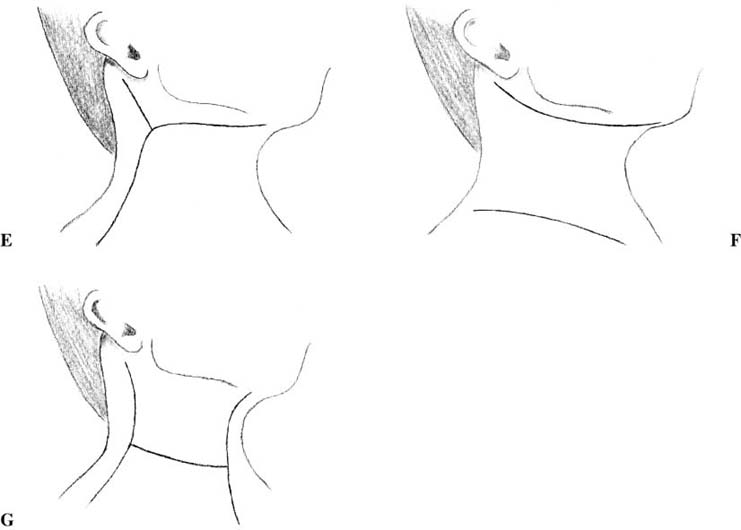
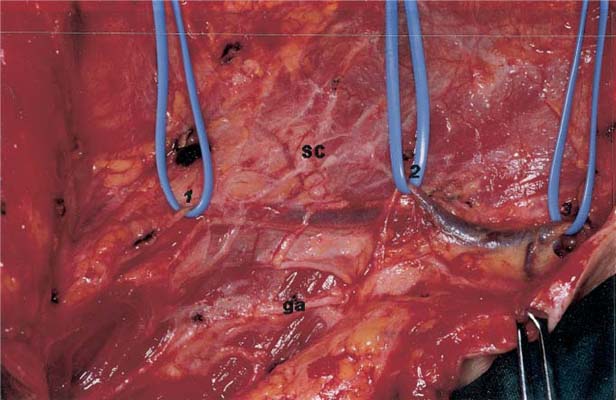
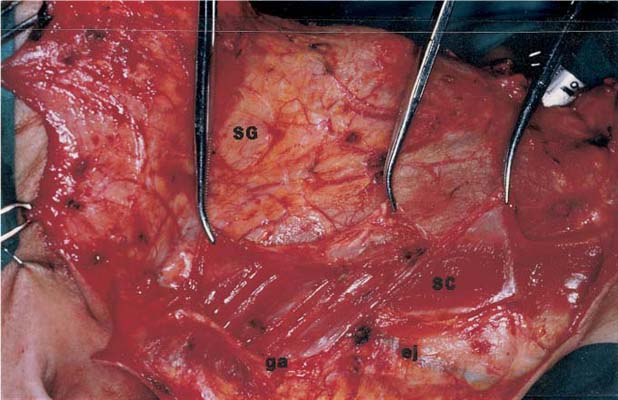
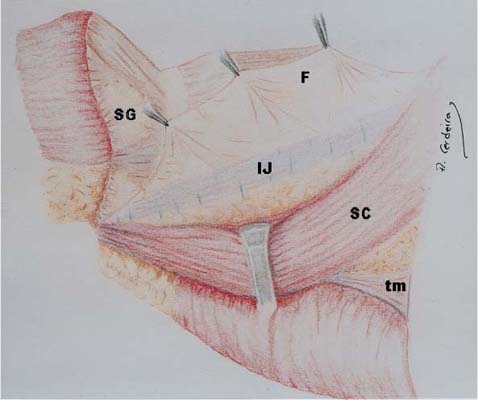
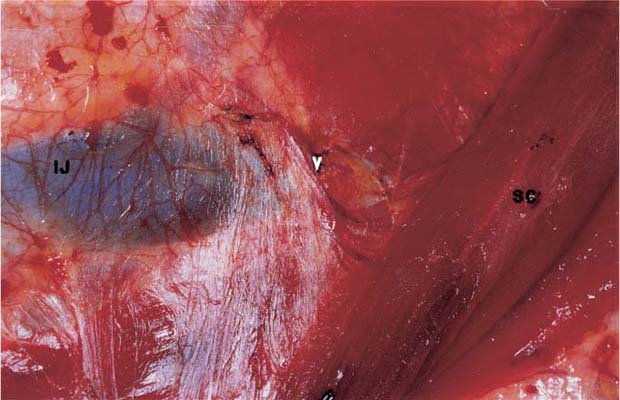
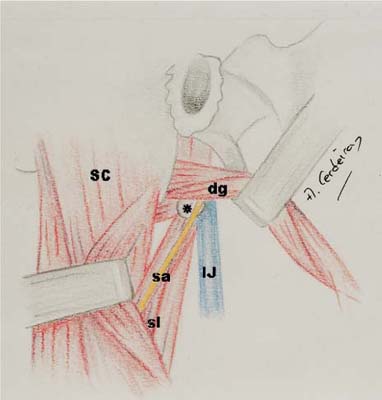
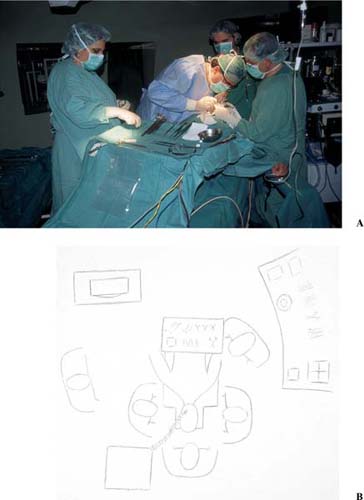
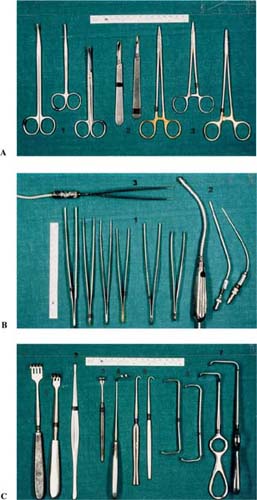
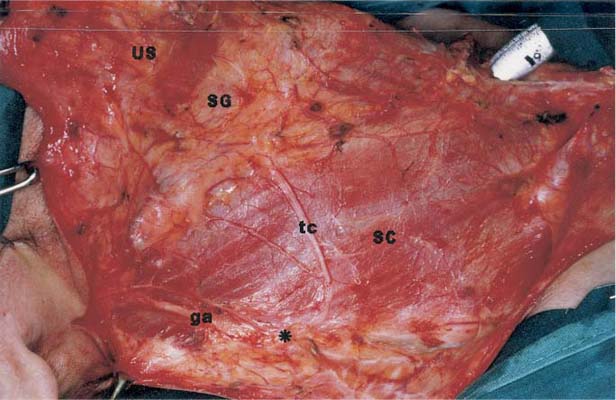
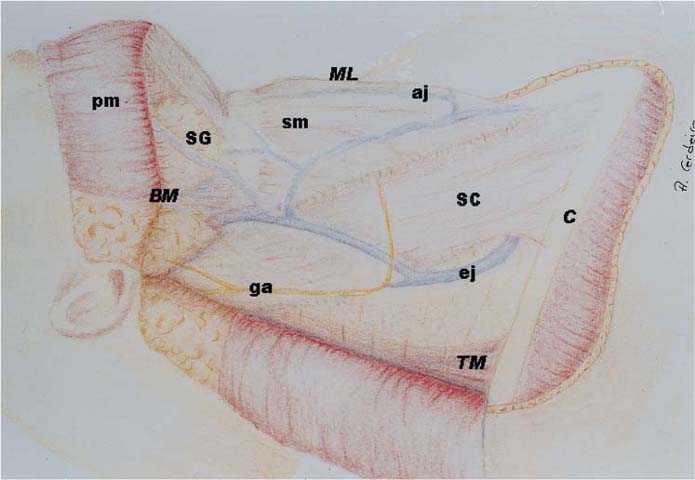
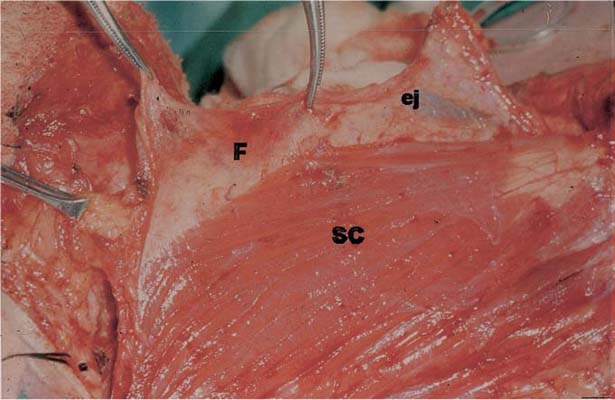
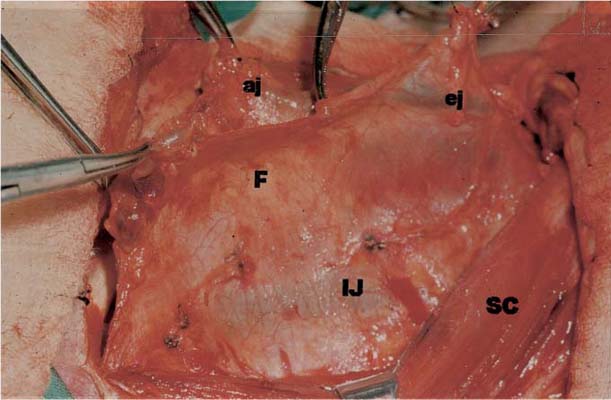
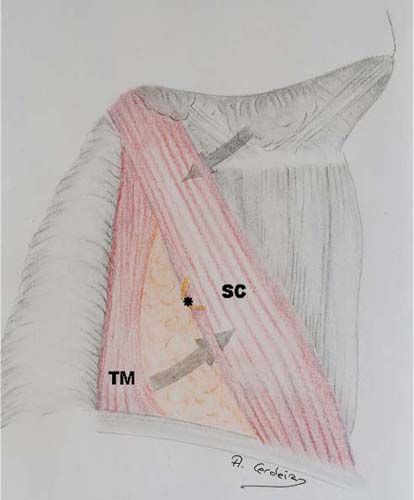
CHAPTER 4 This chapter describes the surgical technique for a complete functional approach to the neck in which all cervical nodal groups are removed. For teaching purposes, the surgical steps are sequentially detailed. However, not every single surgical step of those mentioned must be considered mandatory for every malignant head and neck tumor. As previously emphasized in this book, the preservation of selected nodal groups is a valid option that does not modify the basic principle of the functional approach to the neck (i.e., the removal of lymphatic tissue by means of fascial dissection). Surgeons must be able to decide, according to their own personal experience, which nodal groups should be included in the dissection and which can be preserved, then proceed accordingly, skipping the surgical steps that are not considered necessary. The patient should be prepared as for any major operation. All routine laboratory tests must be performed, including electrocardiogram and chest radiographs. Preoperative evaluation is accomplished by the anesthesiologist prior to surgery. Premedication is used according to the anesthesiologist’s choice. Prophylactic antibiotics are given according to the usual protocol. The patient’s neck and upper chest are shaved and prepared for the operation. The patient is placed supine on the operating table with a pillow or inflatable rubber bag under the shoulders to obtain the proper angle for surgery (Fig. 4-1). This is generally obtained when the occiput rests against the upper end of the table. Elevating the upper half of the operating table to approximately 30 degrees will decrease the amount of bleeding during surgery. The patient’s lower face, ears, neck, shoulders, and upper chest are prepared with surgical solution, and the patient is draped in layers (Fig. 4-2). Four towels are placed and affixed to the skin. Two of the towels are placed horizontally, one from the chin to the mastoid over the body of the mandible and the other across the upper chest from the shoulder to the midline. The remaining two towels are placed vertically, from the mastoid tip to the shoulder, except for unilateral procedures where the second vertical towel is placed in the midline. A sheet is placed over the patient’s chest and legs, and an open sheet covers the entire patient except for the field of operation. The Mayo stand is prepared with the suction tubing and cautery cords secured in place (Fig. 4-3). Two assistants are usually present: one in front of the surgeon and the second at the patient’s head. The scrub nurse stands on the right side of the patient facing the head of the table (Figs. 4-4A, 4-4B). The anesthetist sits at the patient’s head with the machine to the opposite side of the surgery. Few general instruments are needed for the operation (Fig. 4-5). Figure 4-1 Patient prepared for surgery with a pillow under the shoulders to obtain adequate neck extension. Figure 4-2 The patient is covered with drapes and a “Y” incision is outlined on the right side of the neck. Figure 4-3 Mayo stand located over the patient’s chest with the scrub nurse standing at the right side of the surgeon. General endotracheal anesthesia is always used. Muscular relaxation is not a priority but the surgeon must be aware of the patient’s condition to know the degree of contraction that can be expected when approaching the main nerves in the neck. A bloodless field will decrease the operating time and help the identification of neck structures. We do not routinely use infiltration of local anesthetics. Figure 4-4 (A) Picture showing the surgical team for a right-side functional neck dissection. (B) Operating room setup for the operation. Figure 4-5 General instruments used in functional and selective neck dissection. (A) 1, scissors; 2, knives (#10, #15); 3, needle holders. (B) 1, atraumatic and toothed tissue forceps; 2, suction tips; 3, monopolar forceps. (C) 1, Volkmann retractors; 2, Howarth raspatory; 3, Desmarres vascular retractor; 4, Deschamps ligature needle; 5, skin hooks; 6, Farabeuf retractors; 7, Langenbeck retractors. (D) 1, straight Péan’s forceps; 2, large and small Duval forceps; 3, large and small Allis forceps. (E) 1, right-angle forceps; 2, large and small curved Péan’s forceps; 3, Dandy hemostatic forceps; 4, mosquito forceps. The exact location and type of skin incision will depend on the site of the primary tumor and whether a unilateral or bilateral neck dissection is planned. The following are the main goals to be achieved by the skin incision: • Allow adequate exposure of the surgical field. • Assure adequate vascularization of the skin flaps. • Protect the carotid artery if the sternocleidomastoid muscle has to be sacrificed. • Include scars from previous procedures (e.g., surgery, biopsy, etc.). • Consider the location of the primary tumor. • Facilitate the use of reconstructive techniques. • Contemplate the potential need of postoperative radiotherapy. • Produce acceptable cosmetic results. Figure 4-6 Some popular skin incisions for functional and selective neck dissection. (A) Gluck incision for unilateral and bilateral neck dissection. (B) Double-Y incision of Martin. (C) Single-Y incision. (D) Schobinger incision. (E) Conley incision. (F) Mac Fee incision. (G) H incision. A number of skin incisions may be used for neck dissection (Fig. 4-6). A popular incision in our practice is the classic Gluck incision (Fig. 4-6A), which is basically an apron flap incision, with a vertical posterolateral arm to approach the supraclavicular area. For a bilateral functional neck dissection the incision extends between both mastoid tips, crossing the midline at the level of the cricoid arch. This incision allows good exposure when the neck dissection is to be combined with total or partial laryngectomy. Sometimes the vertical arm can be avoided by prolonging the apron flap in a posteroinferior direction, thus producing a better cosmetic result. When the operation includes a total laryngectomy the tracheostomy is usually incorporated in the incision. On the other hand, for partial laryngectomies and other tumors requiring temporary tracheostomy, a small independent horizontal incision is made at the level of the second tracheal ring for the tracheostomy. The double-Y incision of Martin (Fig. 4-6B) is also popular for functional and selective neck dissection. A chin extension may be used when the removal of the primary tumor requires an intraoral approach. A well-known disadvantage of this incision is the compromise to the blood supply, especially in the two crossings of the incision. Thus, the vertical arm of the incision should be placed posterior to the carotid artery. The cosmetic result is improved by giving the vertical arm a slightly S-shaped curve. The single-Y incision (Fig. 4-6C) avoids one of the crossings of the double-Y incision but makes the dissection of the supraclavicular fossa difficult. The Schobinger flap (Fig. 4-6D) is also designed to protect the carotid artery by means of a large anteriorly based skin flap. However the blood supply to the posterosuperior part of the flap is not good and, occasionally, this area becomes devitalized. The Conley modification (Fig. 4-6E) of the Schobinger flap brings the posterosuperior arm of the incision a little further anteriorly. The vertical arm of the incision is extended more posteriorly, toward the lateral third of the clavicle. The incisions commonly used for radical neck dissection in previously irradiated patients may also be used for functional neck dissection. These include the Mac Fee parallel transverse incision (Fig. 4-6F) and the H incision (Fig. 4-6G). They both allow a good preservation of the blood supply to the skin flaps. The Mac Fee incision has excellent cosmetic results. However, the approach to the neck is not as good as with other incisions. Because a functional approach to the neck is not possible in previously irradiated patients where no fascial spaces remain after radiation, this incision is not commonly used for functional procedures. However, it may be useful for modified radical neck dissection when the extension of nodal disease allows preservation of some neck structures. Many other skin incisions may be used depending on the clinical characteristics of the lesion and the personal preference of the surgeon. After the incision is completed, the skin flaps are elevated deep to the platysma muscle, preserving the superficial layer of the cervical fascia (Fig. 4-7). Preservation of the external lymphatic envelope allows further fulfillment of the basic anatomical principle of the functional approach (i.e., removal of the fascial walls of the lymphatic container along with the lymphatic tissue of the neck). Figure 4-7 The skin flaps have been raised, preserving the superficial layer of the deep cervical fascia (right side). US, upper skin flap; SG, submandibular gland; tc, transverse cervical branch from the superficial cervical plexus; SC, sternocleidomastoid muscle; ga, great auricular nerve;*, Erb’s point. The limits for a complete functional neck dissection are similar to those of the classic radical neck dissection (Fig. 4-8). The surgical field should expose superiorly the inferior border of the mandible and the tail of the parotid gland. Inferiorly, the flap should be raised up to the level of the clavicle and the sternal notch. The midline of the neck will be the anterior border of the surgical field for a unilateral neck dissection. Finally, the posterior border of the sternocleidomastoid muscle in the upper part of the surgical field, and the anterior border of the trapezius muscle in the lower half of the neck, constitute the posterior boundary of the dissection. After the flaps have been raised, the underlying neck structures can be seen shining through the superficial layer of the cervical fascia (Figs. 4-7, 4-8). The flaps must be protected by means of wet surgical sponges. Frequent moistening of the sponges will help to keep the skin flaps in good condition throughout the operation. It should be remembered that this may be a long operation since neck dissection is often performed in conjunction with removal of the primary tumor and, in some instances, reconstructive procedures. Thus, all efforts should be made to preserve the skin in good condition until the end of the procedure. Usually, the first step of the operation is the dissection of the fascia that covers the sternocleidomastoid muscle. The goal of this maneuver is to completely unwrap the muscle from its surrounding fascia. Prior to approaching the fascia of the sternocleidomastoid muscle, the external jugular vein must be ligated and divided. Usually, three sections of the external jugular vein are required in functional and selective neck dissection (Fig. 4-9): (1) at the tail of the parotid gland, where the external jugular vein begins by the union of the retromandibular and posterior auricular veins; (2) at the external surface of the sternocleidomastoid muscle; and (3) at a later step of the operation, within the posterior triangle of the neck when this nodal region is included in the dissection. Figure 4-8 Boundaries of a complete functional neck dissection on the right side of the neck. ML, midline; BM, inferior border of the mandible; C, clavicle; TM, trapezius muscle; ga, great auricular nerve; SC, sternocleidomastoid muscle; sm, strap muscles; pm, platysma muscle; ej, external jugular vein; aj, anterior jugular vein; SG, submandibular gland. Figure 4-9 Points of division of the external jugular vein on a right functional neck dissection. 1, tail of the parotid gland; 2, posterior border of the sternocleidomastoid muscle; 3, supraclavicular fossa; SC, sternocleidomastoid muscle; ga, great auricular nerve. The dissection of the sternocleidomastoid muscle begins with a longitudinal incision over the fascia, along the entire length of the muscle. This cut is made with a number 10 knife blade and must be placed near the posterior border of the muscle (Fig. 4-10). This facilitates the dissection of the sternocleidomastoid muscle because the cleavage plane between the fascia and the muscle is much easier to identify in a forward direction. The external jugular vein should be thus transected as close to the posterior border of the sternocleidomastoid muscle as possible. The vein is then included in the specimen and dissected forward with the fascia of the sternocleidomastoid muscle (Fig. 4-11). Using several hemostats, one of the assistants retracts the fascia medially while the surgeon carries the dissection toward the anterior margin of the muscle (Fig. 4-11). Fascial retraction should be done with extreme care because the thin superficial layer of the cervical fascia is the only tissue now included in the specimen. We strongly recommend performing this, as well as most other parts of the operation, using knife dissection. The fascial planes of the neck are mainly avascular and can be easily followed with the scalpel. For knife dissection to be most effective the tissue must be under traction. An important task of the assistants throughout the operation is to apply adequate pressure to the dissected tissue. When the dissection reaches the anterior border of the sternocleidomastoid muscle the hemostats that have been used to retract the fascia may be left lying on the medial part of the surgical field hanging toward the opposite side. This will maintain the required amount of traction while freeing the assistants’ hands. Then the muscle is retracted posteriorly to continue the dissection over its medial face. Retraction is performed initially by one of the assistants, who holds the muscle posteriorly by means of a retractor, while the surgeon continues the dissection over the sternocleidomastoid muscle (Fig. 4-12). When the dissection reaches the deep medial face of the muscle (close to the carotid sheath) the retractor is removed and further separation of the sternocleidomastoid muscle is performed by the surgeon using a hand with a gauze pad. Figure 4-10 Incision of the fascia over the sternocleidomastoid muscle on the right side. Note the posterior placement of the incision with respect to the muscle. SC, sternocleidomastoid muscle; SG, submandibular gland; ej, external jugular vein; ga, great auricular nerve. Figure 4-11 The fascia of the sternocleidomastoid muscle is dissected medially. The external jugular vein is included in the fascia (right side). ej, external jugular vein; F, fascia; SC, sternocleidomastoid muscle. Figure 4-12 Lateral retraction of the sternocleidomastoid muscle allows the dissection of the medial surface of the muscle. The dissected fascia is carefully pulled medially (right side). IJ, internal jugular vein shinning through the fascia; SC, sternocleidomastoid muscle; F, dissected fascia; tm, trapezius muscle; SG, submandibular gland. Until this point, the cleavage plane between the muscle and the fascia is avascular. However, when the deep medial face of the muscle is approached, small perforating vessels are found entering the muscle through the fascia (Fig. 4-13). The assistant must now cauterize the vessels while the surgeon continues the dissection over the entire medial surface of the sternocleidomastoid muscle. The surgeon must be extremely careful at the upper half of this region, where the spinal accessory nerve enters the muscle. One or more small vessels usually accompany the spinal accessory nerve, which often divides before entering the muscle. The vessels should be cauterized without injuring the nerve, and all branches of the nerve must be preserved to obtain the best shoulder function. More details concerning the dissection of the spinal accessory nerve are given in a later stage of the operation. After all the small vessels entering the sternocleidomastoid muscle have been cauterized, a new avascular fascial plane is entered and the dissection continues posteriorly along the entire length of the muscle. The internal jugular vein can now be seen through the fascia of the carotid sheath (Fig. 4-14). The muscle is now almost completely separated from its covering fascia except for a small portion at the posterior border. This part of the muscle will be dissected in a later stage of the procedure. Wet surgical sponges are now introduced in the lower half of the sternocleidomastoid muscle, between the muscle and its dissected fascia. They will serve two purposes: (1) maintain the desired moisture of the dissected tissues while the attention shifts to the upper part of the surgical field, and (2) serve as a reference for the dissection of the fascia that still covers the posterior border of the sternocleidomastoid muscle, in a later stage of the operation. The surgeon now moves to the upper part of the surgical field to complete the identification of the spinal accessory nerve. For a better understanding of the following steps of the operation, at this point it may help the reader to take a short pause in the technical details to realize how the surgical approach is made with respect to the sternocleidomastoid muscle when the posterior triangle is included in the resection. Figure 4-13 Small vessels enter the sternocleidomastoid muscle through its medial face (right side). SC, Sternocleidomastoid muscle retracted laterally; IJ, Internal jugular vein shining through the fascia; V, Vascular pedicle entering the sternocleidomastoid muscle. Figure 4-14 The dissection of the medial face of the sternocleidomastoid muscle has been completed (right side). iJ, internal jugular vein; ej, external jugular vein; aj, anterior jugular vein; SC, sternocleidomastoid muscle; F, dissected fascia. Including the posterior triangle of the neck in the field of dissection requires a combined approach, both posterior and anterior to the sternocleidomastoid muscle (Fig. 4-15). In the upper half of the neck the dissection is performed anterior to the sternocleidomastoid muscle, whereas in the lower half of the neck the supraclavicular fossa is approached posterior to the sternocleidomastoid muscle. To better understand this, imagine the surgical field divided horizontally in two halves by a line passing through Erb’s point, the place where the superficial branches of the cervical plexus appear at the posterior border of the sternocleidomastoid muscle. This creates an upper and a lower part of the neck. The upper half of this division includes the submental and submandibular nodes (area I), the upper part of the posterior triangle of the neck (upper part of area V), and part of the lymphatic chain of the internal jugular vein (area II and part of area III). The dissection of the upper half of this division is performed anterior to the sternocleidomastoid muscle. For this purpose, the muscle must be retracted posteriorly throughout the dissection. The lower half of this imaginary division includes the supraclavicular fossa (lower part of area V), the lower part of the lymphatic chain of the internal jugular vein (area IV and part of area III), and the paratracheal lymph nodes (area VI). These regions will be approached both posterior and anterior to the sternocleidomastoid muscle. The supraclavicular fossa will be dissected from behind the muscle, and the remaining lymph structures of the lower half of the neck will be approached anterior to the sternocleidomastoid muscle. For the surgical specimen to be removed en bloc, the tissue removed from the supraclavicular fossa will be passed beneath the sternocleidomastoid muscle to meet the remaining part of the specimen. This maneuver, which has always been difficult to understand, is detailed in the following text. Figure 4-15 Schematic view of the approach to the neck for a complete functional neck dissection. Above Erb’s point the operation is performed anterior to the sternocleidomastoid muscle. The lower part of the posterior triangle (supraclavicular fossa) is approached posterior to the sternocleidomastoid muscle. SC, sternocleidomastoid muscle; TM, trapezius muscle;*, Erb’s point. Figure 4-16 Anatomical landmarks for the identification of the spinal accessory nerve on its course between the internal jugular vein and the sternocleidomastoid muscle (right side).*
Surgical Technique
PREOPERATIVE PREPARATION AND OPERATING ROOM SETUP



INCISION AND FLAPS
DISSECTION OF THE STERNOCLEIDOMASTOID MUSCLE
MANAGEMENT OF THE STERNOCLEIDOMASTOID MUSCLE
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


