Chapter 66 Surgical Management of Secondary and Tertiary Hyperparathyroidism
Definition
Secondary hyperparathyroidism (SHPT) refers to a derangement in calcium homeostasis leading to a compensatory increase in parathyroid hormone (PTH) secretion.1,2 SHPT requiring parathyroidectomy (PTx) occurs more commonly in progressive chronic kidney disease (CKD)3 and in long-term lithium therapy,4 but it also arises less commonly from disorders of gastrointestinal absorption, deficiency of vitamin D, liver disease, and pseudohypoparathyroidism. The term tertiary hyperparathyroidism (THPT) has been used to define SHPT accompanied by spontaneous hypercalcemia and clinically persistent SHPT after successful renal transplantation.1,5
Secondary Hyperparathyroidism
Epidemiology
It is well known that CKD induces SHPT and SHPT is one of the serious complications that influence mortality and quality of life (QOL) in patients with CKD.6–9 Multivariate analysis showed that younger age, female gender, white race, absence of diabetes, long duration of hemodialysis, use of intravenous vitamin D, previous renal transplantation, and several other comorbid conditions are factors indicating the need for of PTx.10,11 The Japanese Society for Dialysis Therapy (JSDT) reported that in Japan the frequency of PTx was about 10% in patients who had had hemodialysis for more than 10 years and was about 30% among those being hemodialyzed for more than 20 years.12
The Dialysis Outcome and Practice Pattern Study (DOPPS) evaluated the situation and quality of hemodialysis therapy from 1996 to 2001. Baseline prevalence of PTx (%) and the incidence of PTx at follow-up for100 patients/year in each country were as follows: France, 14.3%, 1.8; Germany, 6%, 1; Italy, 5%, 0.9; Japan, 4.1%, 0.6; Spain, 5.7%, 1.5; the United Kingdom, 9.2%, 1.5; and the United States, 4%, 0.5, respectively.13
Kestenbaum et al. and Foley et al. analyzed the PTx rate in the United States.14,15 The first group of authors reported that the rate had decreased in the United States between 1995 and 1999 (by approximately 30%) independently of changes in the general patient’s characteristics. The later authors reported that more recently the rate increased between 1998 and 2002 (from 9.8% to 12%).
The PTx rate may be influenced by new trends of medical therapy—that is, with vitamin D receptor (VDR) activators and calcimimetics. Cinacalcet hydrochloride (HCL) (cinacalcet) has recently become available all over the world and will have impact on the treatment of SHPT.16 Cunningham et al. reported that cinacalcet reduced the requirement of PTx in 90% of patients as compared with a placebo group.17 However, the costs and the cost utility of medical therapy including cinacalcet may to some extent limit the use of this new therapy and thereby influence the rate of PTx in different countries.
Pathogenesis, Histopathology, and Pathophysiology
A summary of pathogenetic factors leading to SHPT in CKD is presented in Figure 66-1. These factors are hypocalcemia, hyperphosphatemia, and deficiency of active vitamin D.18 It has been confirmed that renal impairment induces hyperphosphatemia and phosphate retention, which directly acts on parathyroid cells and stimulates PTH secretion, synthesis, and the proliferation of parathyroid cells.19 Recently a novel phosphaturia hormone fibroblast growth factor (FGF23) has been identified. FGF23 is secreted from osteocytes, and the serum level of FGF23 is progressively elevated to compensate for persistent phosphate retention, which results in reduced renal production of 1,25-dihydroxyvitamin D and thereby stimulates secretion of PTH, suggesting its critical role in the pathogenesis of altered mineral homeostasis in CKD.20,21 Furthermore, it has recently been shown that FGF23 directly acts on parathyroid cells and mediates the secretion of PTH in the presence of Klotho as a cofactor.22,23
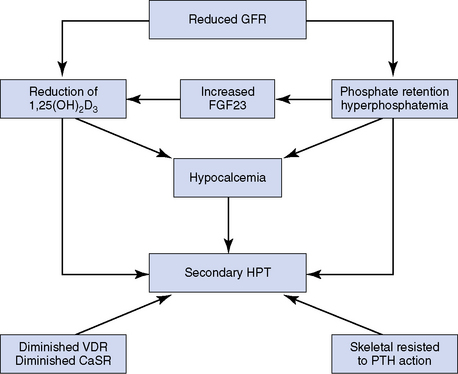
It has been confirmed that there is a diminished expression of VDR and calcium sensing receptor (CaSR) in parathyroid cells in patients with CKD,24,25 and these patients have skeletal resistance against PTH because of diminished expression of the PTH/parathyroid hormone-related protein (PTHrP) receptor in osteoblasts, overexpression of osteoprotegerin, accumulation of 7-84 PTH fragments, as well as accumulation of several uremic toxins.26 These factors interact to form a complex pattern that leads to progressive SHPT in the setting of CKD.
The characteristic histopathologic findings of SHPT are summarized as asymmetrical glandular enlargement, nodularity, and an increase in oxyphilic and transitional oxyphilic cells27 (see Chapter 70, Surgical Pathology of the Parathyroid Glands). Patterns of parathyroid hyperplasia in SHPT are classified into four categories: diffuse hyperplasia, early nodularity in diffuse hyperplasia, nodular hyperplasia, and single nodular gland.27 When glandular weight exceeds 500 mg, almost all glands contain nodular hyperplasia.28 It has been hypothesized that in CKD patients polyclonal diffuse hyperplasia is transformed into nodular hyperplasia with several nodules in which parathyroid cells proliferate monoclonally with high growth potential27–31 (Figure 66-2). It has been speculated that different genetic hits within initial hyperplastic glands may result in nodularity in SHPT, but the underlying mechanisms are still unclear.32,33
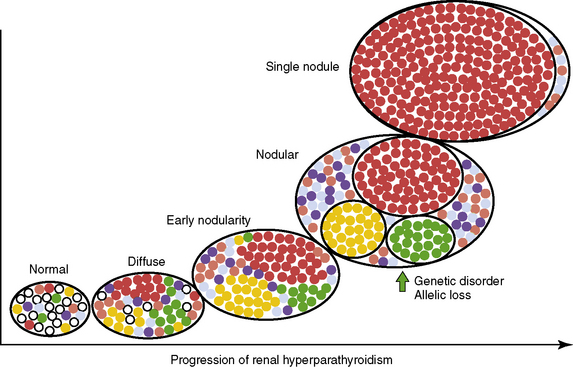
Moreover it has been confirmed that expression of VDR and CaSR in parathyroid cells are diminished in nodules.24,25 From this we infer that cells within nodules have a resistance to calcitriol and hypercalcemia. Therefore, it has been hypothesized that when at least one parathyroid gland progresses to nodular hyperplasia, the SHPT in these patients may be refractory to medical treatments.28,34
Medical Treatment
The majority of patients with SHPT can be managed by medical treatment. At present, many modalities are available for the medical treatment of SHPT (Table 66-1). Kidney Disease Improving Global Outcome (KDIGO), an international workshop, recently proposed clinical practice guidelines for CKD related to mineral and bone disease (CKD-MBD).35 The guidelines recommend lowering the serum phosphorous level to above the normal laboratory range and in hemodialysis patients to keep circulating intact PTH levels between two to nine times higher than the upper normal limit.35
Table 66-1 Available Therapeutic Modalities for Secondary Hyperparathyroidism
To avoid the progression of SHPT, patients should, of course, have known important pathogenetic factors controlled.36 However, in some patients SHPT advances in spite of adequate medical treatment. To control hypocalcemia, dialysate containing high calcium concentration and calcium containing phosphate binders should be employed. To control hyperphosphatemia, removal of phosphorous by adequate hemodialysis, limitation of phosphate intake, and administration of phosphate binders (i.e., calcium carbonate, calcium acetate, sevelamer HCl or lanthanum carbonate) are recommended.37 Other treatment options for lowering PTH include calcitriol, vitamin D analogs, and cinacalcet. However, VDR activators can induce hypercalcemia and hyperphosphatemia, which can prohibit their use is patients with SHPT.
Cinacalcet acts on CaSR in parathyroid cells through an allosteric action and increases the sensitivity of extracellular ionized calcium. It stimulates cell-signaling pathways to mobilize intercellular calcium and decreases PTH secretion without hypercalcemia or hyperphosphatemia.16,38
Based on the clinical evidence, the Kidney Foundation of the United States proposed the Kidney Disease Outcomes Quality Initiative (K/DOQI) clinical practice guidelines for bone metabolism and disease. The guidelines recommend that in hemodialysis patients, the serum calcium level should be 8.4 to 9.5 mg/dL, the serum phosphorus level should be 3.5 to 5.5 mg/dL, the calcium phosphorous product should be less than 55 mg2/dL,2 and the intact PTH level should be controlled within 150 and 300 pg/mL, mainly to avoid ectopic calcification and cardiovascular complications.39
Clinical Symptoms
Table 66-2 shows the clinical symptoms of SHPT. Laboratory examination usually reveals a remarkably high serum PTH level, hyperphosphatemia, and high bone metabolic markers (total alkaline phosphatase [Al-P], bone specific Al-P, and osteocalcin, among others). The serum calcium level is usually low without medical treatment but is easily influenced by medical treatment.
Table 66-2 Clinical Symptoms of Secondary Hyperparathyroidism
Neuromuscular psychiatric symptoms are often more severe in SHPT than in primary hyperparathyroidism (primary HPT). Patients frequently complain of muscular weakness, irritability, sleeplessness, itching, and cough. Ectopic calcification of vessels and heart valves induce cardiovascular complications and contribute to high mortality.6–9 Calciphylaxis, cutaneous necrosis induced by calcific uremic arteriolopathy, and progressive skin necrosis can occur and constitute a condition of considerable mortality.40,41
Surgical Indications
KDIGO guidelines propose that there are no specific indications for PTx, but it should be considered when severe SHPT is resistant to medical/pharmacologic therapy. Although no studies demonstrate a beneficial effect of this treatment on mortality because of cardiovascular complications, PTx performed by an expert surgeon generally results in a marked, sustained reduction in levels of serum PTH, calcium, and phosphorus.35
Previously, surgical indications in SHPT have mainly been based on clear-cut severe symptoms or evidence of bone disease. Currently with treatment with vitamin D and vitamin D analogs, the clinical findings of SHPT have changed. High serum phosphorous, calcium, and PTH levels may persist without severe symptoms and high bone turnover. It has been clarified that in patients with CKD, high values of phosphorous, calcium, and PTH are associated with increased mortality, mainly because of cardiovascular complications induced by ectopic calcifications.6–9 Importantly, currently as a result when serum phosphorous, calcium, and PTH levels cannot be maintained within target ranges, medical treatment including active vitamin D therapy should not be continued, and PTx should be considered to avoid the progression of ectopic calcifications.42
K/DOQI guidelines from the U.S. Kidney Foundation have proposed that PTx should be recommended in patients with severe SHPT (persistent serum levels of intact PTH > 800 pg/mL), associated with hypercalcemia or hyperphosphatemia, which is refractory to medical therapy.39
A European guideline of clinical algorithms on renal osteodystrophy recommends PTx when a high PTH level (> 50 pmol/L) has not decreased by more than 50% after 2 months of medical therapy, or when there is persistent hypercalcemia and hyperphosphatemia or persistent clinical symptoms with parathyroid gland diameter estimated by parathyroid imaging are over 1 cm.43
The JSDT guidelines recommend surgical treatment at an early stage of SHPT, because progressive SHPT is known to influence mortality. These guidelines propose that parathyroid intervention therapy should be recommended in patients with severe SHPT (Table 66-3).44 The assessment of parathyroid mass with ultrasonography (US) is an important factor to predict the response to medical treatment and for reaching a decision on surgical treatment.45,46 Three dimensions of parathyroid glands can be measured by US, and the volume of glands can be estimated using the formula a × b × c × π/6 (a, b, and c refer to dimensions of the gland). A gland with a volume exceeding 300 to 500 mm,3 or where the largest diameter is more than 1 cm, is likely to have developed nodular hyperplasia.47 This implies autonomy and a lack of responsiveness to medical management.
Table 66-3 Surgical Indications for Secondary Hyperparathyroidism Modified by JSDT Guideline
| Essential Components |
| Clinical Findings |
| If patients have one of these factors, parathyroidectomy should be absolutely recommended: 1. Severe osteitis fibrosa, high bone turnover 2. Progressive ectopic calcification 3. Subjective symptoms (bone and joint pain, arthralgia, muscle weakness, irritability, pruritus, depression) 5. Progressive reduction in bone mineral content 6. Anemia resistant to erythropoietin stimulating agent (ESA) |
The induction of cinacalcet has influenced the surgical indications for SHPT (Table 66-4). Unfortunately, it has not been determined at present which particular groups of patients might benefit best from cinacalcet therapy and which are better treated by expeditious PTx.48–50 Moreover, cinacalcet could be of value also as an alternate therapy for SHPT patients judged to be less optimal surgical candidates (Table 66-5).50–52
Table 66-4 Surgical Indications for SHPT in the Era of Cinacalcet
Table 66-5 Indications for Consideration for Cinacalcet Therapy from Surgeon’s Viewpoint
Surgical Procedures
There is a range of surgical options for PTx in patients with SHPT, including (1) subtotal PTx, (2) total PTx with autograft, and (3) total PTx without autograft. Subtotal PTx and total PTx with autograft are widely accepted for SHPT (Table 66-6). Rothmund et al. performed a randomized study comparing subtotal PTx and total PTx with autograft; they found no significant difference with respect to efficacy and recurrence rate between the two operative procedures.53 Thus, the method used for the surgical treatment of SHPT may depend on the surgeon’s preference (1 to 3).54–62 Another important question concerns the role for total PTx without autograft. Might this be a more preferable operative procedure in hemodialysis patients? K/DOQI and JSDT guidelines recommend against total PTx without autograft in patients with CKD stage 5D waiting for kidney transplantation, as control of serum calcium level may be difficult following kidney transplantation.39,44 Some clinical studies have indicated that total PTx without autograft may be an equally safe and successful procedure for SHPT as subtotal PTx or total PTx with autograft. Total PTx without autograft is superior with respect to prevention of recurrence.54,63–65 Even when all parathyroid glands are removed, usually PTH levels are measurable because of remaining nests of parathyroid cells, mainly located in the thymus.63,65
Table 66-6 Operative Procedures for Secondary and Tertiary Hyperparathyroidism
| Accepted Procedures | Our Recommended Procedure | |
|---|---|---|
| SHPT not anticipating RTx | Total PTx with autograft Total PTx without autograft Subtotal PTx | Total PTx with autograft |
| SHPT anticipating RTx | Total PTx with autograft Subtotal PTx | Total PTx with autograft |
| THPT | Subtotal PTx Total PTx with autograft | Total PTx with autograft |
Notes:
• Total PTx with autograft is suitable for patients who are not candidates for renal transplant and require long-term hemodialysis after PTx. Sufficient parathyroid function should be preserved to avoid a dynamic bone disease.
• Total PTx without autograft is acceptable for patients in whom long-term survival is not expected and recurrent HPT should be avoided.
• In patients with SHPT who are anticipating renal transplantation and patients with THPT, sufficient parathyroid function should be preserved to avoid uncontrollable hypocalcemia after kidney transplant; subtotal PTx or total PTx with autograft is acceptable.
• We prefer total PTx with forearm autograft in all three situations, because in Japan, hemodialysis patients can survive long term after PTx and the chance of kidney transplantation is limited. After total PTx with forearm, it is easier to control parathyroid function than after the other two procedures.
SHPT, secondary hyperparathyroidism; THPT, tertiary hyperparathyroidism; RTx, renal transplantation; PTx, parathyroidectomy.
According to our experience, subtotal PTx is frequently followed by recurrent hyperparathyroidism (HPT) because of residual parathyroid tissue in the neck. When reexploration of the neck is required, there is a higher risk of injury to the recurrent laryngeal nerves than at the initial operation, and reoperation also implies some risk for parathyromatosis. For patients who require long-term hemodialysis after PTx, the risk for recurrence is not negligible,56,58 as it is easier and safer to remove residual parathyroid tissue from the forearm at recurrence as compared with a neck reexploration. Thus, we feel total PTx with forearm autograft is the preferred option in a patient who has to continue hemodialysis for long periods after PTx.58
Parathyroid intervention therapy including percutaneous ethanol injection (PEIT), direct vitamin D injection therapy, radiofrequency ablation, and high-intensity focused ultrasonography (HIFU) has been tried in limited numbers of patients with both primary HPT and SHPT.66 PEIT can be used to manage SHPT over the long term, provided that only one parathyroid gland is enlarged to more than 500 mm3 estimated by US.67 However, if surgery is required after PEIT, it is often difficult to identify remaining parathyroid tissue and the recurrent laryngeal nerve.68 PEIT should therefore be limited to patients in whom only one gland is substantially enlarged and in patients with a high risk for undergoing standard open PTx under general anesthesia.44
Preoperative Examination and Management
Generally, PTx for SHPT is performed under general anesthesia. Because hemodialysis patients frequently suffer from cardiovascular disease, careful preoperative evaluation is required. Special attention is given to control hyperpotassemia and regulate hydration status, which is required before the operation. PTx can improve cardiac dysfunction in patients with dilated cardiomyopathy. In these patients, the operation may be better performed under local anesthesia because of the high risk of general anesthesia. Initially cinacalcet should be tried, and if surgery is necessary, the operation under local anesthesia should be limited.69
To avoid bleeding from the wound, anticoagulant agents and antithrombotic medicine should be discontinued appropriately. Special attention should be paid to ectopic glands including mediastinal, intrathyroidal, and undescended glands. Careful preoperative imaging is useful to detect these ectopic glands, and we recommend US and a sestamibi scan before initial PTx.44
Surgical Approach
In SHPT, the stimuli affect all parathyroid glands and tissue, and fundamentally all glands, including supernumerary glands, become hyperplastic. Thus, to avoid persistent/recurrent HPT, all parathyroids, including supernumerary glands, should be identified. It has been reported that the frequency of supernumerary glands detected at surgery for SHPT is 15% to 20%.70–72 To remove supernumerary glands, resection of the surrounding fat tissue of original parathyroid glands is essential. In our series, the ratio of rudimentary and split glands was present in 24.8% of cases. It is not so difficult to detect these types of glands during the operation because the glands are usually located in the vicinity of the original ones. The most common location of these supernumerary glands was in thymus.70,72,73 Such supernumerary glands in thymus are frequently detected histopathologically after the operation when parathyroid nests are identified microscopically in thymic tissue. In our series, about 40% of inferior glands were located in the thymic tongue. Then removal of thymic tissue from the neck incision is therefore essential to avoid missing glands.73 The second frequent location of supernumerary glands is the paratracheal and paraesophageal areas, so a careful search of these regions is necessary.70
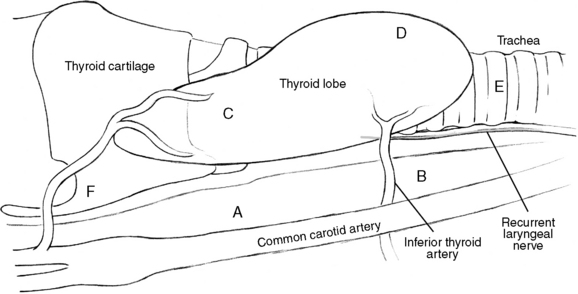
The junction between the recurrent laryngeal nerve and the inferior thyroid artery is a useful landmark for detecting parathyroid glands. The superior glands are frequently located above the junction and dorsal in relation to the recurrent laryngeal nerve (Figure 66-3, area A). If the gland cannot be identified in this region, the ventral area from the recurrent laryngeal nerve (Figure 66-3, area C) should be explored. Superior glands sometimes drop into the paraesophageal area in a retromediastinal direction (Figure 66-3, area B), and the gland can easily be identified by following the inferior thyroid artery. If the superior gland is missed, the ipsilateral upper pole of thyroid lobe should be mobilized as well as the posterior surface of thyroid lobe, the area around superior thyroid artery, and the space anteromedial of the recurrent laryngeal nerves (adjacent to Berry’s ligament). Also the lateral and posterior areas of esophagus and carotid sheaths should be searched.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


