Surgical Anatomy of the Nose: A Foundation for Rhinoplasty
David W. Kim
Ted Mau
GENERAL PRINCIPLES
Success in rhinoplasty depends on the surgeon’s ability to create favorable functional and cosmetic changes to the nose. The operation is difficult for a number of reasons: noses are complex, three-dimensional, highly variable structures; most maneuvers attempt to alter a framework that has inherent resistance to manipulation; and the changes that are created are often subtle and subject to relentless postoperative forces of scar contracture. To overcome these challenges, the surgeon must have the ability to analyze a nose and match its variations to underlying structural correlates. Techniques may then be chosen to alter these structures into an optimal form while maintaining support and function. Finally, the maneuvers must be executed with meticulous precision. In rhinoplasty, these steps of diagnosis, selection of technique, and execution are possible only with a clear understanding of the complex anatomy.
This chapter describes sequentially the anatomy of the different regions and components of the nose. Infinite variations of these regions exist and may be the result of differences in ethnicity, gender, age, trauma, congenital deformity, or prior surgery. The unique structural characteristics of each nose underlie each individual’s external appearance and may motivate that person to seek surgery. Whether or not these variations should be classified as variant anatomy is a semantic question, but because of this huge diversity, it is problematic to designate a “normal” archetypal anatomy toward which rhinoplasty surgery should aspire.
Each section in this chapter begins with general anatomic concepts, detailing the orientations and relations that are most commonly encountered. Subsequently, “variations” from normal anatomy are discussed, particularly as they pertain to rhinoplasty. A separate section focuses on the structural architecture of the nose, emphasizing how the various individual anatomic elements integrate into a stable unit. Although the chapter emphasizes anatomy predominantly, discussions on rhinoplasty philosophy, analysis, technique, and complications are included where germane.
SURFACE ANATOMY
Discussion of the surface anatomy of the nose begins within the larger contextual framework of the face. In general, the nose occupies the central horizontal third of the face, from the glabella to the subnasale, and central vertical fifth, between the medial canthi. Variations of nasal dimension and position may cause the nose to extend outside of these confines. These divergences may draw attention to the nose and may therefore be a patient’s motivation to undergo rhinoplasty. Directional references and topographic landmarks are illustrated in Figures 179.1, 179.2, 179.3, 179.4, 179.5.
Subunits
The external topography of the nose is divided into six subunits. These consist of the nasal dorsum, sidewalls, tip, columella, ala/sill, and soft triangles (Fig. 179.6). These areas are defined by the shadows and highlights cast by incident light. Human visual processing depends on these light-dark contrasts to form a perception of the nose. The subunits do not necessarily have sharply defined boundaries and do not mirror exactly the underlying anatomic structures. Nonetheless, it is crucial for the nasal surgeon to identify them in preoperative assessment, particularly in external nasal reconstruction. During reconstruction, effort should be made to place scars within subunit borders whenever possible, as the human eye is more apt to discern a scar that traverses across a subunit than one that outlines it. This may require a surgeon to resect and replace an entire subunit (or subunits) involved, rather
than replace only the primary defect, even if this requires removal of areas of healthy tissue. Tissue of a similar thickness, color, and consistency should be used to reconstruct these defects.
than replace only the primary defect, even if this requires removal of areas of healthy tissue. Tissue of a similar thickness, color, and consistency should be used to reconstruct these defects.
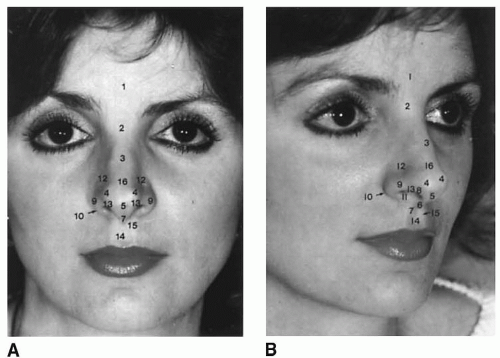 Figure 179.1 Topographic key landmarks and accepted designations for (A) frontal and (B) oblique views of the nose. 1, Glabella; 2, nasion, nasofrontal angle; 3, rhinion (osseocartilaginous junction); 4, tip-defining point; 5, infratip lobule;6, columella; 7, columella-labial junction; 8, facet; 9, alar sidewall;10, alar-facial junction; 11, medial crural footplate; 12, supra-alar crease; 13, alar margin; 14, philtrum; 15, philtral crest; 16, supratip dorsum. (From Tardy ME. Surgical anatomy of the nose. New York: Raven Press, 1990, with permission.) |
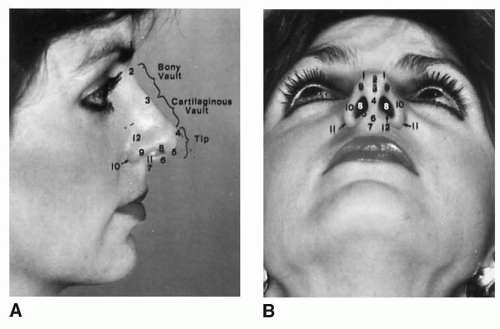 Figure 179.2 A: Topographic key landmarks and accepted designations for lateral view of the nose. 1, Glabella; 2, nasion (nasofrontal junction); 3, rhinion (osseocartilaginous junction); 4, tip-defining point; 5, infratip lobule; 6, columella; 7, columella-labial junction; 8, facet; 9, alar lobule; 10, alar-facial junction; 11, medial crural footplate; 12, supra-alar crease. B: Topographic key landmarks and accepted designations for basal view of the nose. 1, Tip-defining point; 2, interdomal area, alar lobule; 3, infratip lobule; 4, columella; 5, medial crural footplate; 6, columella-labial junction; 7, philtrum; 8, nostril aperture; 9, facet; 10, alar sidewall; 11, alar-facial junction; 12, nostril sill. (From Tardy ME. Surgical anatomy of the nose. New York: Raven Press, 1990, with permission.) |
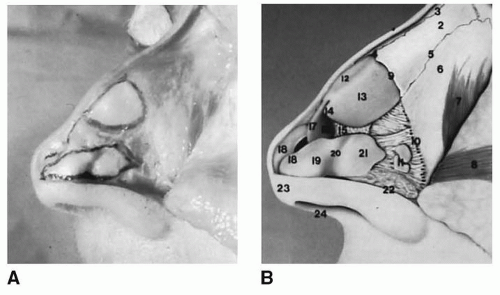 Figure 179.3 Key anatomic landmarks (A) and standard terminology (B) for lateral view of fresh cadaver dissection of nose. 1, Nasofrontal suture line; 2, nasal bone; 3, intranasal suture line; 4, osseocartilaginous junction (rhinion); 5, nasomaxillary suture line; 6, ascending process of maxilla; 7, levator labii superioris muscle; 8, transverse nasalis muscle; 9, cephalic portion of ULC (articulates to undersurface of nasal bone); 10, piriform margin; 11, sesamoid cartilages; 12, cartilaginous dorsum; 13, upper lateral cartilage; 14, caudal free margin of ULC; 15, intercartilaginous ligament; 16, quadrangular cartilage; 17, anterior septal angle; 18, tip-defining point alar cartilage; 19, lateral crus of alar cartilage; 20, concavity (“hinge”) of lateral crus; 21, lateral aspect of lateral crus; 22, alar lobule; 23, infratip lobule; 24, columella. (From Tardy ME. Surgical anatomy of the nose. New York: Raven Press, 1990, with permission.) |
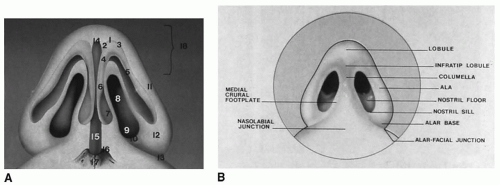 Figure 179.4 Additional anatomic landmarks (A) and standard nasal terminology of base of nose (B). 1, Apex of alar cartilage; 2, medial genu; 3, lateral genu; 4, transitional segment; 5, lateral crus; 6, medial crus; 7, medial crural footplate; 8, nostril aperture; 9, nostril floor; 10, nostril sill; 11, lateral alar sidewall; 12, alar lobule; 13, alar-facial junction; 14, anterior septal angle; 15, caudal septum; 16, maxillary crest; 17, nasal spine; 18, infratip lobule. (From Tardy ME. Surgical anatomy of the nose. New York: Raven Press, 1990, with permission.) |
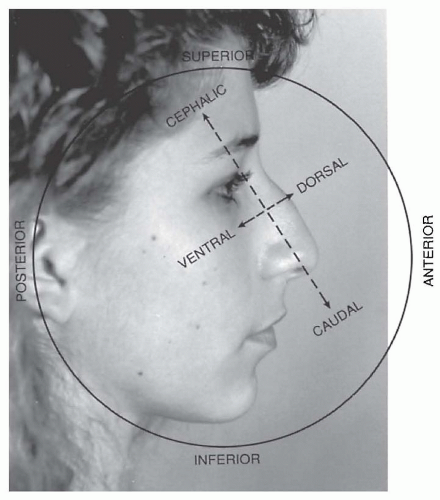 Figure 179.5 Preferred directional references applied to the nose. Note that the axes shift to lie oriented to the nasal dorsal line. |
Topography
A discussion of surgical anatomy must begin with the external topography that surgery aims to alter. A detailed discussion of aesthetic facial analysis is found in Chapter 170. What follows is a limited discussion of nasal analysis and definitions of terms with specific relevance to rhinoplasty anatomy. Correlation of nasal topography to underlying structural anatomy is introduced—details of this anatomy are discussed in greater depth in subsequent sections.
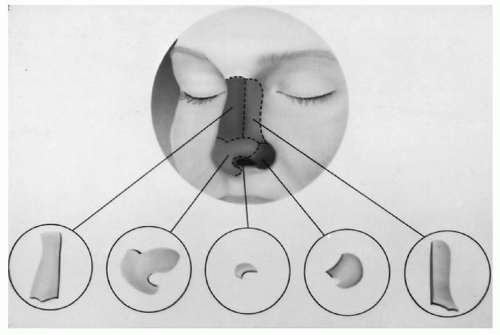 Figure 179.6 Aesthetic topographic subunits of the nasal surface. From left to right: dorsum, tip/columella, soft tissue triangle, alar lobule, and sidewall. The columella may be considered a separate distinct subunit. (From Tardy ME. Surgical anatomy of the nose. New York: Raven Press, 1990, with permission.) |
On frontal view, a gentle, unbroken curve should appear from the lateral brow to the nasal tip on each side of the nose (Fig. 179.1A). These brow-tip aesthetic lines should follow the normal changes of nasal width: wider cephalad at the brow/nasal root transition, narrower in the middle vault, and wider again at the tip. An irregular brow-tip aesthetic line may be correlated to bony and cartilaginous vault irregularities through palpation and close inspection with a light placed above the patient to enhance shadowing. When the upper cartilaginous vault is overly narrow, the curvature of these brow-tip lines is exaggerated.
General tip shape may be determined from the frontal and base views (e.g., bulbous, deviated, wide, amorphous, asymmetrical). The unique features of tip shape are determined by the endless variations of form, dimension, and position of the lower lateral cartilages (LLCs) and surrounding structures. Inference about the thickness of the nasal skin may be made from inspection of the contour of the tip. A tip with sharp features reflects underlying structures transmitting through thin skin. A smooth, bulbous tip is likely covered by thick skin.
The base view also provides information about the shape and size of the columella, alar base, nostrils, and infratip lobule (Figs. 179.2B and 179.4). In most noses, the frontal and base views reveal a triangular shape of the nose in which the nasal base (interface of nose and face) is wider than the tip and dorsal line. The triangularity of the tip depends on the presence of an unbroken line from a narrower nasal tip to a wider nasal base. Poor structural support along this line will manifest as alar pinching or concavity of the alar margins on frontal and base views. When the base is excessively narrow or the tip overly wide, a square or trapezoidal shape instead of triangular
configuration is present (1). The width of the infratip lobule reflects the underlying shape of the intermediate crura of the LLCs. Asymmetry in the columella may be caused by asymmetries of the shape or trajectory of the medial crura, deflection of the caudal edge of the cartilaginous septum, or both. The lateral flaring of the alar lobules is only indirectly determined by the shape and strength of the lateral crura of the LLCs, as the lobules themselves are composed of soft tissue only and are caudal to the lateral crura.
configuration is present (1). The width of the infratip lobule reflects the underlying shape of the intermediate crura of the LLCs. Asymmetry in the columella may be caused by asymmetries of the shape or trajectory of the medial crura, deflection of the caudal edge of the cartilaginous septum, or both. The lateral flaring of the alar lobules is only indirectly determined by the shape and strength of the lateral crura of the LLCs, as the lobules themselves are composed of soft tissue only and are caudal to the lateral crura.
On lateral view, several important external landmarks may be identified (Fig. 179.2A). The nasion is the most concave point at the nasofrontal angle and corresponds anatomically to the midline of the nasofrontal suture. This angle is determined by the height of the radix, the most cephalic portion of the nasal dorsum, and the slope of the forehead. An average nasofrontal angle measures 120 degrees in the Caucasian nose. The vertical position of the nasion marks the nasal starting point and is typically between the supratarsal crease and the upper eyelid margin. The rhinion corresponds to the osseous-cartilaginous junction and often marks the location of a dorsal hump. Proceeding caudally, the presence or absence of a supratip breakpoint depends on the dorsal height of the cartilaginous septum and the projection of the domal region of the LLCs. The tip-defining point, or the pronasale, is the most anterior projection of the nose. The overall projection and rotation of the nasal tip may be assessed by using Goode’s method, in which the nasal tip projection (from the alar crease to the tip-defining point) is divided by nasal length (from nasion to tip-defining point). According to Goode, the normal value should be 0.55. The nasolabial angle in men is typically between 90 and 95 degrees and in women, between 95 and 105 degrees. This angle may be affected by variations of the size and shape of the upper lip and premaxillary bone. Therefore, the nasolabial angle does not always reflect the degree of tip rotation. The lateral view of the ideal nostril is oval shaped, with 2 to 4 mm of the columella visible beneath the alar rim.
Variant Anatomy
Because the nose is a three-dimensional structure that is viewed in whole, the topographic dimensions of one area have an optical effect on the appearance of other areas. This is critical during rhinoplasty, as surgical changes to one region or parameter of the nose create the illusion of change to another. Examples as they pertain to external nasal topography follow.
Dorsal Height
The overall height of the nasal dorsum is determined predominantly by the size and development of the highly variable cartilaginous and osseous nasal septum. In general, an increased overall projection of the dorsum on the lateral view corresponds to a narrower appearance on the frontal view. Conversely, a low nasal bridge creates a wider-appearing nose from the front. This is explained by the concept that one looks down the apex of a triangle when observing a nose from the front. In a nose with a high dorsum, the sidewalls are subject to more shadowing, and the apex of the triangle appears narrower. In a nose with a low bridge, the cross-sectional triangular geometry of the nose is flattened, or if surgical hump reduction has occurred, it is truncated into a trapezoid. With less shadowing of the sidewalls, the nose appears wider on frontal view. Local differences in dorsal height create other illusions. In a normal profile, the radix, middorsum, supratip, and nasal tip are linear or nearly colinear. Because our eyes are accustomed to this norm, deviations from these relations create certain optical illusions. For instance, the presence of a mid-dorsal convexity creates an illusion of an underrotated nasal tip, irrespective of absolute tip position. A dorsal concavity, in contrast, creates a perception of increased tip rotation and a shorter nose. Before the surgeon commits to making true alterations of tip position, the effects of dorsal height and its modification must be carefully weighed.
Radix and Nasofrontal Angle
Variations in radix height have an effect on numerous aesthetic nasal parameters such as the nasal starting point, nasofrontal angle, overall dorsal profile, and apparent intercanthal distance. A low radix, as commonly seen in individuals of African or Asian descent, creates an illusion of increased intercanthal distance (see earlier explanation). If associated with tip underprojection, a low radix may create an appearance of a dorsal hump. Correction of this appearance may be accomplished with augmentation of the radix and increasing tip projection instead of reduction of the dorsum to the level of the low radix (Fig. 179.7). Maintaining a higher dorsum offers the advantages of a narrower appearance on front view and avoidance of an open-roof deformity associated with hump reduction. A high radix, in contrast, creates an appearance of decreased intercanthal distance. When excessive height at the radix blunts the nasofrontal angle, the distinction between the nose and forehead may be blurred, creating the illusion of a longer nose. This is particularly true in the presence of a posteriorly sloping forehead. Because of the abundant overlying soft tissue in this area, reduction of osseous height at the radix does not transmit well to overall profile reduction. Conversely, a more acute nasofrontal angle creates an illusion of a shorter nose, independent of the actual vertical position of the nasal starting point.
Nasolabial Angle
The nasolabial angle, formed by the upper lip and columella, is widely used as a metric for the degree of rotation of the nasal tip. This region, however, is composed of numerous anatomic components with a high degree of variation and in reality may not accurately reflect the
overall degree of nasal tip rotation. Fullness in this area may be caused by an overdeveloped quadrangular cartilage in the area of the posterior septal angle, a prominent nasal spine and premaxillary bone, or tenting of the soft tissue in a projecting nose. These variations create a more obtuse angle, irrespective of the true rotational position of the nasal tip. However, even if the true rotational position of the tip is not changed, an increased nasolabial angle creates an illusion of increased tip rotation. Conversely, when these structures are less developed or retrusive, a relative deficiency on the nasolabial angle may be present, leading to a perception of counterrotation (Fig. 179.8).
overall degree of nasal tip rotation. Fullness in this area may be caused by an overdeveloped quadrangular cartilage in the area of the posterior septal angle, a prominent nasal spine and premaxillary bone, or tenting of the soft tissue in a projecting nose. These variations create a more obtuse angle, irrespective of the true rotational position of the nasal tip. However, even if the true rotational position of the tip is not changed, an increased nasolabial angle creates an illusion of increased tip rotation. Conversely, when these structures are less developed or retrusive, a relative deficiency on the nasolabial angle may be present, leading to a perception of counterrotation (Fig. 179.8).
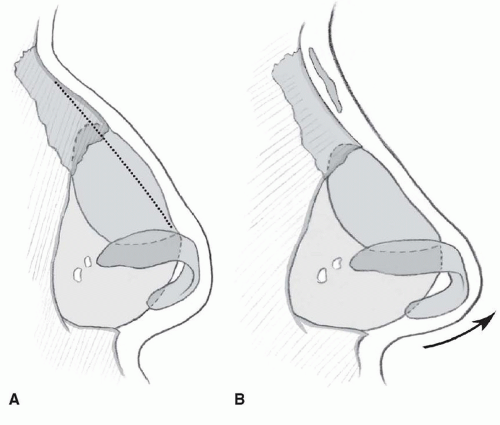 Figure 179.7 A: Profile view of a nose with a true dorsal hump in the region of the rhinion. Correction may involve reduction of the hump. B: Nose with a relative dorsal convexity due to a low radix and an underprojected nasal tip. Correction might involve elevating of the radix with a graft and increasing tip projection. Final external dorsal contour is similar in both examples. |
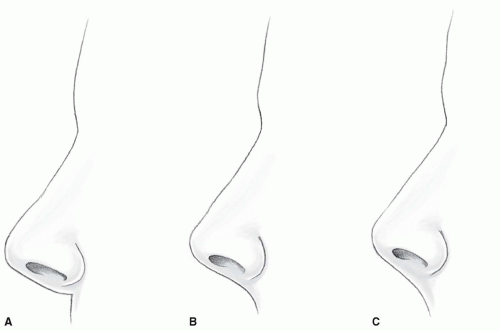 Figure 179.8 Lateral view of three noses with identical tip position. A: Relative deficiency of tissue at the nasolabial area and an acute nasolabial angle creates an illusion of underrotation of the tip. B: Nose with a moderate nasolabial angle. C: Fullness at the nasolabial area with an obtuse nasolabial angle creates an illusion of increased tip rotation. |
Alar-Columellar Relation
With alar retraction or a dependent caudal edge of the cartilaginous septum, excessive columellar height is visible on the lateral view. This hanging columella may create an illusion of a ptotic nasal tip, even when tip position is normal. In contrast, a retracted caudal septum or a low alar margin may lead to a relative lack of columellar show and an associated illusion of increased tip rotation. The size, position, and interrelations of the medial crura, caudal septum, lateral crura, and alar soft tissue determine these variations.
SKIN-SOFT TISSUE ENVELOPE
The nose is constructed of a skeletal framework onto which a skin-soft tissue envelope (SSTE) is draped. Although the framework is the subject of most surgical techniques, the appearance of the nose is determined by the manner in which the SSTE drapes over the modified skeleton. An understanding of the composition of the SSTE and its variant anatomy guides the surgeon in choosing appropriate techniques for successful surgery.
Skin
The skin of the nose varies in thickness depending on its location. The skin is thickest at the nasion and thinnest at the rhinion (2). From the rhinion, the skin becomes progressively thicker as it descends along the dorsum to the tip, where a large number of sebaceous glands reside. The skin becomes thin again at the most caudal aspect of the nose along the alar margin and columella.
Understanding skin thickness variation along the dorsum aids the rhinoplasty surgeon in performing dorsal hump reduction. Because the skin is thinnest at the rhinion, a straight external profile requires a small relative convexity to remain in this region. If the dorsum is reduced so that a straight skeletal profile results, a slight concavity at the middorsum is likely to result after skin redraping (3). This may create a cartilaginous pollybeak, in which the supratip dorsum projects above the plane of the dorsum cephalad to it. To avoid this, hump reduction should be carried out incrementally, with verification of the effect of each pass on external contour through the SSTE.
Subcutaneous Tissue
The subcutaneous layer of the nose is made up of the superficial fatty layer, the fibromuscular layer, the deep fatty layer, and the periosteum or perichondrium. The superficial fatty layer is directly connected to the dermis. The fibromuscular layer comprises the nasal subcutaneous muscular aponeurotic system (SMAS) (4). The nasal SMAS is in continuity with the SMAS of the rest of the face and encases and interconnects the mimetic muscles of the nose. The deep fatty layer contains the neurovascular system of the soft tissue envelope. Dissection in the avascular plane between the deep fatty layer and the perichondrium and periosteum is met with little mechanical resistance or bleeding and results in the least postoperative scarring and contraction.
Muscles
The mimetic muscles of the nose reside within the SMAS. They are divided into four groups (5) (Table 179.1). The elevator muscles shorten the nose and dilate the nostrils, the depressor muscles lengthen the nose and dilate the nostrils, the compressor muscles lengthen the nose and narrow the nostrils, and the minor dilator muscles widen the nostrils. In addition to these individual functions, the muscles work synergistically to alter the shape of the nasal tip, alae, and dorsum. For example, simultaneous contraction of the levator labii superioris and the depressor septi nasi may depress the nasal tip, “round up” the supratip area, and lengthen the nose (6). The muscles, particularly the dilator naris (7), also serve to maintain the tone of the nostrils during inspiration, as illustrated in the patient with ipsilateral facial nerve paralysis with unilateral alar collapse (8). Dissection in the sub-SMAS layer of the soft tissue envelope allows the surgeon to avoid the nervous supply to the nasal muscles.
Although most rhinoplasty techniques do not directly address nasal muscles, division of the depressor septi nasi may correct drooping of the nasal tip and shortening of the upper lip during facial animation. The small, paired muscle that originates at the anterior nasal spine and inserts onto the medial crura footplates may be addressed through simple division (6), muscular release and plication (9), or dissection and transposition of the muscle (10). In selected patients, these techniques may reduce gingival show and nasal tip descent during smiling, elevate the nasal tip, and elongate the upper lip in the resting state.
Arterial Supply
The superficial vascular supply to the external nose derives from both the external and internal carotid systems. The
facial artery branches into the angular artery and the superior labial artery. The lateral nasal branch of the angular artery supplies the lateral surface of the caudal nose. Branches of the superior labial artery supply the nasal sill and the base of the columella. The columellar artery, a branch of the superior labial artery, is often encountered in the transcolumellar incision used in the external rhinoplasty approach. The septal branches of the superior labial artery enter the nose on each side of the nasal spine and form the major blood supply to the anterior septum. Large septal mucosal flaps may be pedicled on the nasal spine area with these branches for reconstructive purposes.
facial artery branches into the angular artery and the superior labial artery. The lateral nasal branch of the angular artery supplies the lateral surface of the caudal nose. Branches of the superior labial artery supply the nasal sill and the base of the columella. The columellar artery, a branch of the superior labial artery, is often encountered in the transcolumellar incision used in the external rhinoplasty approach. The septal branches of the superior labial artery enter the nose on each side of the nasal spine and form the major blood supply to the anterior septum. Large septal mucosal flaps may be pedicled on the nasal spine area with these branches for reconstructive purposes.
TABLE 179.1 INVESTING NASAL MUSCULATURE | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
The dorsal nasal artery, an external branch of the ophthalmic artery, anastomoses with the lateral nasal branch of the angular artery, forming an axial arterial network for the dorsal nasal skin. Arterial supply to the nasal tip derives from branches of the anterior ethmoid and angular arteries. The external nasal branch of the anterior ethmoid artery perforates the transverse nasalis muscle of the nasal sidewall and descends toward the nasal tip. The lateral nasal branch of the angular artery sends off branches from the ala anteriorly toward the nasal tip. The vascular plexus to which these arteries contribute resides predominantly in the adipose layer just deep to the SMAS. Remaining in the plane just above the perichondrium and periosteum during dissection minimizes injury to these vessels.
Sensory Nerve Supply
Sensation to the external nasal skin is supplied by branches of the ophthalmic and maxillary divisions of the trigeminal nerve. Twigs from the supratrochlear and infratrochlear branches of the ophthalmic nerve supply sensation to the skin of the radix, the rhinion, and the cephalic portion of the nasal sidewalls (11). The external nasal branch of the anterior ethmoidal nerve supplies the skin over the dorsum of the caudal nose down to and including the nasal tip. This branch emerges between the caudal edge of the nasal bone and the upper lateral cartilage (ULC) and courses in the SMAS layer. Injury to this nerve during intercartilaginous or cartilage-splitting incisions can result in tip numbness (11). Branches of the infraorbital nerve provide sensation to the side of the lower half of the nose and the lateral vestibule. The nasopalatine nerve, a branch of V2 that enters the nose through the incisive foramen, provides the major sensory supply to the posterior two-thirds of the nasal septal mucosa, maxillary gingiva, and anterior palatal mucosa. This nerve may be injured during surgery involving the maxillary crest or nasal floor and can result in temporary numbness near the incisors (12).
Inner Lining
The nasal vestibule is lined with keratinizing squamous epithelium. The surfaces of the nasal cavities, with the exception of the superior olfactory epithelium, are covered by ciliated stratified or pseudostratified respiratory epithelium (13). Because of its high vascularity, the vestibular epithelium and intranasal mucosa are excellent sources of local flaps for reconstruction of the inning lining in fullthickness nasal defects. In such procedures, a free cartilage graft is often used to rebuild structure for the nose. The rich vascular intranasal lining flap nourishes the cartilage graft from its undersurface. Common inner lining donor sites are the nasal septum or nasal vestibule. These flaps are discussed in more detail in Chapter 165. During routine rhinoplasty, care must be taken to preserve vestibular skin in the internal nasal valve area to avoid web formation and nasal valve stenosis (14).
Variant Anatomy
Thickness of the SSTE varies with ethnicity, age, and gender. Noses with thin, less sebaceous skin assume a shape that closely matches the underlying cartilaginous and osseous structure. In contrast, the underlying nasal architecture does not accurately transmit through the soft tissue envelope in thicker-skinned noses. These concepts are critical in rhinoplasty.
In the thick-skinned individual, modifications of the underlying framework, particularly reductive alterations, may not result in significant changes in external appearance because of poor redraping of the overlying SSTE. In these patients, the surgeon should consider augmenting areas of relative deficiency to create a framework that pushes and stretches the thick SSTE into a desirable shape. In such cases, overall proportion of the nose becomes more important than absolute size. Because a thick SSTE cannot conform onto the underlying structure after reduction, scar tissue may fill the resulting void. An example is the soft tissue/scar pollybeak that results after aggressive supratip hump reduction in a thick-skinned individual. Little to no external lowering of the supratip convexity occurs as the cartilaginous hump is simply replaced by scar beneath a noncompliant SSTE.
In patients with thin skin, even small irregularities of the underlying structure may become evident after surgery as the soft tissue envelope redrapes very closely to the framework below. In these cases, care must be taken to camouflage grafts, edges of bone and cartilage, and any other contour irregularities. Graft must be placed in a precise manner, and any edges that may transmit through the skin should be beveled or crushed to blend seamlessly into surrounding structures. Soft tissue or crushed cartilage onlay grafts may aid in camouflaging irregularities.
SKELETAL FRAMEWORK
The skeletal framework of the nose may be divided into thirds: the upper third consisting of the osseous vault; the middle third consisting of the upper cartilaginous vault; and the lower third consisting of the lower cartilaginous vault. The nasal septum, consisting of a bony and a cartilaginous portion, provides support in all three sections
and divides the nasal cavity into two lateral halves. In this section, these structures are discussed individually, with an emphasis on anatomic forms and their variations. In a later section, the interrelations of these bodies as they pertain to nasal structural mechanics are discussed.
and divides the nasal cavity into two lateral halves. In this section, these structures are discussed individually, with an emphasis on anatomic forms and their variations. In a later section, the interrelations of these bodies as they pertain to nasal structural mechanics are discussed.
Septum
The nasal septum is a sagittal midline structure that divides the nose into two cavities and provides structural support to the osseous and cartilaginous vaults (15). The septum is divided into a cephalic-posterior osseous septum, composed of the perpendicular plate of the ethmoid and the vomer, and a caudal-anterior cartilaginous septum, consisting of the quadrangular cartilage.
The perpendicular plate of the ethmoid forms the dorsal aspect of the osseous septum. Its superior attachment consists of the frontal bone and its nasal spine anteriorly and the cribriform plate posteriorly. Anterosuperiorly, it articulates with the inward projection of the nasal bones in the midline. Anteroinferiorly, it borders the quadrangular cartilage, and posteroinferiorly, it borders the vomer. The thickness of the perpendicular plate of the ethmoid varies considerably, and it is rarely pneumatized. Because it is attached to the cribriform plate, aggressive lateral force high on the osseous septum may lead to fracture of the skull base and resultant cerebrospinal fluid leak or olfactory bulb injury.
The vomer, one of the bones that make up the skull, is shaped like the keel of a boat. In a midsagittal view of the skull, its superior edge forms a line connecting the sphenoid sinus to the anterior nasal spine. Superiorly, the vomer articulates with the perpendicular plate of the ethmoid. Inferiorly, it attaches to the midline nasal crest of the palatine bone posteriorly and the maxilla anteriorly. Anterior to its articulation with the vomer, the maxillary crest forms a groove into which the quadrangular cartilage sits. The posterior free edge of the vomer forms the posterior border of the choanae.
The quadrangular cartilage comprises the cartilaginous septum. This structure rests within a groove in the nasal spine and maxillary crest inferior to it. This ventral surface is typically thickened in comparison to the remainder of the structure. Dorsally, the quadrangular cartilage forms the contour of the nasal bridge externally. The ULCs articulate with the cephalic aspect of the quadrangular cartilage, forming the dorsum of the central third of the nose. The most caudal portion of the cartilage extends anterior to the nasal spine and is the least rigid portion (Fig. 179.9). Three angles may be identified at the caudal edge of the septum (Fig. 179.10). The anterior septal angle is usually the most anterior projection of the septum and forms the transition between the dorsal and caudal components of the supportive cartilaginous septal L-strut. The domal regions of the LLCs are in intimate proximity and typically project beyond the anterior septal angle, creating the external topography of the nasal tip. Because of this relation, deviations of the anterior septal angle may cause distortions of nasal tip position. The posterior septal angle is located at the quadrangular cartilage articulation with the anterior nasal spine. The intermediate septal angle lies between the anterior and posterior septal angles.
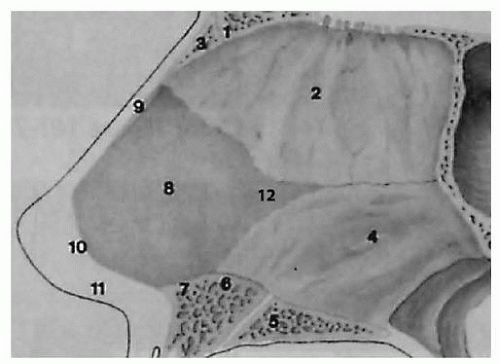 Figure 179.9 Anatomy of the typical nasal septum. 1, Nasal process and frontal bone; 2, perpendicular plate of ethmoid bone; 3, nasal bone; 4, vomer bone; 5, palatine bone; 6, maxillary crest; 7, nasal spine; 8, quadrangular cartilage; 9, upper lateral cartilage; 10, caudal margin quadrangular cartilage; 11, membranous septum; 12, posterior projection of “tongue” of quadrangular cartilage (variable length). (From Tardy ME. Surgical anatomy of the nose. New York: Raven Press, 1990, with permission.) |
The membranous septum is the soft tissue continuation of the cartilaginous septum. Consisting of a central layer of subcutaneous areolar tissue between vestibular skin on each side, the membranous septum bridges the caudal edge of the cartilaginous septum to the medial crura and columella. Contained within it are the ligamentous attachments of the medial crura to the caudal septum. Because of a lack of cartilage, it is mobile and displaces easily with manipulation of the columella.
The septum is lined with an inner layer of perichondrium or periosteum covered by an outer layer of mucosa.




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
