Chapter 33 Surgical Anatomy and Monitoring of the Recurrent Laryngeal Nerve
 Please go to expertconsult.com to view related videos Recurrent Laryngeal Nerve Monitoring and Continuous Vagal Monitoring.
Please go to expertconsult.com to view related videos Recurrent Laryngeal Nerve Monitoring and Continuous Vagal Monitoring.
 This chapter contains additional online-only content, available on expertconsult.com.
This chapter contains additional online-only content, available on expertconsult.com.
Introduction
Galen, in the second century, discovered and named the recurrent laryngeal nerve (RLN). He found that vagal sectioning in a pig resulted in aphonia. Until this time, speech was thought to be controlled by the heart.1 In the seventh century, Paulus Aegineta suggested that the RLN could be avoided during surgical treatment of the thyroid. Vesalius, in the sixteenth century, provided anatomic drawings of the RLN and superior laryngeal nerve (SLN) distribution.2 In 1872, Kocher performed his first thyroidectomy. Kocher’s meticulous technique reduced operative mortality and was adopted by Halstead. At about this time Billroth abandoned the procedure as a result of hemorrhage and postoperative sepsis. Wolfler noted a 29.5% RLN paralysis rate in 44 patients operated by Billroth over 5 years.3 In 1909, Kocher was awarded the Nobel Prize for his work in physiology, pathology, and surgery of the thyroid gland. Safe thyroid surgery, introduced by Halsted in the United States after a period of study with Kocher, was the foundation on which the clinics of Crile, Lahey, and the Mayo brothers were built (see Chapter 1, History of Thyroid and Parathyroid Surgery). This chapter reviews the surgical anatomy of the RLN, related surgical and management maneuvers, and monitoring techniques for the RLN. The SLN is discussed only where its inclusion seems appropriate in relation to its brethren RLN as it relates to thyroidectomy, so the reader is referred to Chapter 32, Surgical Anatomy of the Superior Laryngeal Nerve.
Reported Incidence of RLN Paralysis
Knowledge of the anatomy, surgical maneuvers, and monitoring techniques for the RLN is important given the frequency and significance of RLN paralysis at thyroidectomy. The reported incidence of RLN paralysis is reviewed in depth in Chapter 15, Pre- and Postoperative Laryngeal Exam in Thyroid and Parathyroid Surgery.
Certainly, permanent RLN paralysis rates in expert hands have been reported in the 1% to 2% range.4 However, the rates of RLN paralysis after thyroidectomy in many studies are likely underestimates for several reasons. First, the thyroid units with unfavorable data are less likely to report their findings. Second, most injuries are not detectable intraoperatively by surgeons. Lo, for example, found that surgeons had recognized intraoperative injury in only 1% of cases when, in fact, that surgical injury had occurred in nearly 7% of patients.5
An additional important reason for RLN paralysis underestimation is that, in studies looking at this issue, not all patients undergo postoperative laryngeal examination. Typically, only patients who are significantly and persistently symptomatic have their larynxes inspected. Several workers have shown the lack of reliability of clinical symptoms in vocal cord paralysis (see Chapter 15, Pre- and Postoperative Laryngeal Exam in Thyroid and Parathyroid Surgery).6–8 Variability in symptoms results from variation in degree of injury, cord position, contralateral cord compensation, and the evolution over time in position of the paralyzed cord. With symptomatic assessment of vocal cord function, a human tendency exists to “identify success and ignore failure.”5 The Scandinavian Quality Register has found that the rate of RLN paralysis doubles when all patients are routinely examined with postoperative laryngeal exam.9 All patients need to have preoperative and postoperative laryngeal examination if we are to appreciate the true rate at which RLN injury occurs.
Although the rate of RLN paralysis with thyroidectomy in expert hands may be low, Djohan recently wrote that “the estimated incidence of RLN injury in standard thyroidectomy is from 2% to 13%.”10 Steurer recently found that if patients operated on for thyroid cancer are examined within 1 week of surgery, 15% are found to have paralysis.8 Foster, in reviewing 24,108 thyroidectomies, described a rate of 2.5% for tracheotomy.11 Recently a large systematic review of the literature reviewing 25,000 patients found a postoperative rate of 9.8%.12
Bilateral thyroidectomy is unique in head and neck surgery in that both left and right cranial nerves are subject to risk in one surgical procedure. The RLNs innervate the airway introitus. Bilateral cord paralysis occurs frequently enough in patients undergoing bilateral thyroid surgery that indications for tracheotomy in patients undergoing bilateral thyroidectomy have been developed.13 Some workers have recommended prophylactic tracheotomy for patients requiring extensive resection.11
Several workers have shown that rates of RLN paralysis during thyroid surgery are greater in cases associated with (1) lack of RLN identification during surgery, (2) bilateral surgery, (3) surgery for cancer, (4) surgery associated with significant lymph node resection, (5) surgery for Graves’ disease or thyroiditis, (6) revision surgery, (7) surgery associated with substernal goiter, (8) surgery associated with longer operating room times or greater blood loss, and (9) patients brought back to surgery because of bleeding. Also, surgeon experience has been related to RLN paralysis rates with rates of < 1% being associated with surgeons performing greater than 45 nerve dissections per year.4,5,14–17 A large German multicenter study yielded the following risk factors, in descending order of their importance (odds ratio), for permanent paresis of RLN: carcinoma recurrence (6.66), goiter recurrence (4.67), carcinoma first operation (2.04) (comparison in each case with benign nodular goiter), hemithyroidectomy (versus subtotal resection, 1.76), no nerve identification versus nerve identification (1.41), hospital experience (1.34), and surgeon experience (1.23)17
Laryngeal Exam in All Patients Preoperatively and Postoperatively
Surgical management of the recurrent laryngeal nerve and recurrent laryngeal nerve monitoring is necessarily wedded with knowledge of glottic function preoperatively and postoperatively (see Chapter 15, Pre- and Postoperative Laryngeal Exam in Thyroid and Parathyroid Surgery).
Preoperative laryngeal exam is necessary for the following reasons:
1. Vocal cord paralysis may present preoperatively in the absence of voice complaints.
2. Vocal cord palsy present preoperatively suggests invasive malignancy. Its identification informs preoperative planning and radiographic evaluation.
3. Vocal cord palsy may be present preoperatively even in the setting of benign disease (discussed later).
4. Management of the invaded RLN found at surgery is in part affected by the knowledge of preoperative functional status.
5. Responsibility for postoperative vocal cord palsy can be wrongly attributed if one fails to demonstrate its presence preoperatively.
6. Preoperative laryngeal exam provides a preoperative baseline for postoperative laryngeal assessment.
Postoperative laryngeal exam is necessary for the following reasons:
1. Glottic exam is the only existent accurate postoperative RLN outcome measure. Voice changes may occur without vocal cord paralysis, and vocal cord paralysis may occur without voice changes.
2. Postoperative functional glottic information allows for maximum interpretation of intraoperative electromyography (EMG) data from the neural monitoring.
3. Vocal cord paralysis present postoperatively has significant implications for the safety of swallowing and for the planning of future contralateral surgery. The presence of postoperative unilateral vocal cord paralysis is therefore important whether or not it is associated with symptoms. Vocal cord paralysis has been found to have significant adverse effects to work-related outcome measures in up to 40% of patients affected.18
This chapter assumes that all patients undergoing thyroid and parathyroid surgery have pre- and postoperative laryngeal exams (see Chapter 15, Pre- and Postoperative Laryngeal Exam in Thyroid and Parathyroid Surgery). A discussion of nerve management at surgery does not make sense without this basic information.
Preoperative Vocal Cord Paralysis
The presence of preoperative vocal cord paralysis has been studied in the setting of benign thyroid surgical disease. Overall, the rate of preoperative vocal cord paralysis in patients ultimately found to have benign thyroid disease is approximately 0.7%.53,56 However, Shin et al. reported that 2% of patients out of a total of 198 patients presented with vocal cord paralysis in the setting of benign disease and in the absence of prior neck surgery.19
The proposed mechanism through which benign disease may result in vocal cord paralysis includes distention-stretch, compression, edema, ischemia, perineural fibrosis, calcification, and toxic neuritis.53,59 Some cases of preoperative vocal cord paralysis are likely unrelated to the thyroid and may be related to left atrial enlargement, aortic aneurysm, nonthyroid neoplastic disease of the head and neck, esophagus, lung, or mediastinum or may be idiopathic. Certainly the finding of preoperative paralysis warrants an aggressive radiographic evaluation, typically with axial contrast-enhanced computed tomography (CT) to evaluate the neck base fully.
The prognosis of vocal cord paralysis associated with benign thyroid disease is reasonably good, with reports ranging from 37% to 66% resolution after surgery. Ceroni and others noted that recovery usually occurs within the first 4 to 6 months after surgery, rarely later than 1 year.36,53,59–62 One may question whether some of these cases of motion recovery, which are not confirmed by laryngoscopy, are in fact cases of symptomatic improvement through contralateral vocal cord compensation or a gradual medialization of the affected cord. In my experience in these cases of benign disease with preoperative vocal cord paralysis, if vocal cord EMG cannot be elicited at surgery with ipsilateral vagal stimulation, recovery will not occur postoperatively (see the next section, “Preop Laryngeal Exam and Intraoperative Electrical Stimulability”).
Preoperative vocal cord paralysis is a strong predictor of invasive thyroid disease and mandates additional radiographic evaluation including CT scan or magnetic resonance imaging (MRI) to check for the extent of invasive disease. CT and MRI studies can also identify subtle laryngeal findings that are associated with vocal cord paralysis, including posterior cricoarytenoid muscle atrophy, thyroarytenoid muscle atrophy, anteromedial deviation of the arytenoid cartilage, enlarged pyriform sinus, enlarged laryngeal ventricle, and paramedian cord position20 (Figure 33-1). If a known ipsilateral vocal cord paralysis is present, a mass judged as indeterminate for invasion by the radiologist should be considered invasive until proved otherwise. CT or MRI findings of vocal cord paralysis may not always be present and do require a fine-cut neck and airway CT scan and an experienced head and neck radiologist. Thus, preoperative radiographic evaluation of the larynx does not replace the need for preoperative laryngeal examination.

Preop Laryngeal Exam and Intraoperative Electrical Stimulability
The relationships among laryngeal exam, electrical stimulability, and nerve invasion are interesting. In our series of monitored patients, we have looked at the laryngeal function and monitoring of intraoperative EMG data in several interesting subsets of patients (see Figure 33-2, A and B) (Ditpi Kamani and Greg Randolph, unpublished data, 2011). In 22 patients found ultimately to have nerves invaded by malignancy, the laryngeal exam was normal preoperatively in 45% and was less than normal in 55%. In these 22 patients with nerves invaded with cancer during surgery, recurrent laryngeal nerve was routinely identified above and below the area of invasion and electrically stimulated. In the patients with nerve invasion, 36%, when stimulated, showed no response, whereas 63% showed electrical stimulability despite the intraoperative finding of nerve invasion. If preoperative laryngeal function was normal, the invaded nerve gave an average waveform of 180 μV, whereas if the invaded nerve was associated with preoperative vocal cord paralysis and maintained electrical stimulability, the average waveform was only 63 μV. Thus, invaded nerves are associated approximately 50% of the time with preop clinical nerve paralysis evident, yet they remain electrically stimulable in two thirds of cases (with a low level of EMG response). The resection of such nerves would be expected to worsen voice and dysphagia, so patients should be counseled with this in mind even if they present, as 50% do, with preop nerve paralysis (see Figure 33-2, A).
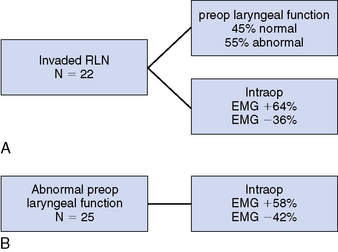
We have also looked at the subgroup of 25 patients who presented with less than normal preoperative laryngeal function and found that intraoperative EMG response was obtainable in 58%. If the reason for laryngeal dysfunction was past surgery and the patient maintained electrical stimulability, the average waveform was only 93 μV. If, on the other, hand preop laryngeal function was less than normal, the nerve retained electrical stimulability, and this was due to invasive cancer, the average waveform was only 63 μV. Of note in patients with preoperative less than normal laryngeal function, the recurrent laryngeal nerve failed to be electrically stimulable in 42% of patients. Goretzki et al. have presented a small series of such patients who retain some electrical stimulability despite preop paralysis.21 Thus, in patients with preop laryngeal paralysis or paresis, nearly 60% maintain electrical stimulability with low-level EMG, which varies depending on the etiology of the paralysis (see Figure 33-2, B).
Visualization of Nerve
The RLN should be visualized in all cases. Lahey, in 1938, helped to introduce the routine dissection and demonstration of the RLN during thyroid surgery. Lahey believed that the identification of the RLN was so important that he routinely divided the inferior thyroid artery laterally to facilitate dissection of the RLN to its laryngeal entry point. Lahey’s paralysis rate with nerve identification fell from 1.6% to 0.3% in more than 3000 nerve dissections over a 3-year period.22 Crile was also an advocate for RLN identification but believed that the RLN was extremely sensitive—more so than other peripheral nerves—to surgical trauma and so proposed the “doctrine of vulnerability.”37 Kocher’s technique of thyroidectomy involved medial mobilization of the thyroid after lateral ligation of the middle thyroid vein. He left a posterior capsule intact to protect the RLN and parathyroid glands.38 Lore has been an advocate for RLN preservation through operative identification, as has Lennquist.39,40 The doctrine of vulnerability has had its proponents, however. Wade believed that any manipulation in the region of the RLN would promote vocal cord paralysis.41 Perzik noted that “the dissection at no time should be directed at identification and uncovering of the RLN.”31 These authors suggested a blind capsule technique for RLN management. We now understand that the RLN tolerates appropriate surgical dissection.42–45 It also has been shown that recurrent laryngeal nerve identification and dissection does not increase the rate of parathyroid devascularization.23
Many studies prove that RLN identification during thyroidectomy is associated with lower rates of postoperative RLN paralysis.23–25 Jatzko reviewed 10 studies of 12,211 thyroid operations; in cases without RLN identification, he found temporary paralysis in 7.9% and permanent paralysis in 5.2%; with RLN identification, 2.7% of cases had temporary paralysis and 1.2% had permanent paralysis.23 A recent study by Chiang also concluded that routine identification by visualization is recommended in thyroid surgery, and a nerve that was documented to be not damaged intraoperatively was most likely to recover postoperatively.26 Hvidegaard described a paralysis rate (without identification) ranging from 3% to 9.4% and a rate ranging from 0.3% to 2% with nerve identification.46 Wagner noted RLN paralysis in 7% of patients without and 3.8% of patients with RLN identification.17 Mountain noted a rate of paralysis three to four times higher without routine RLN exposure.47 Riddell found a 0.6% RLN paralysis rate with nerve identification and a 2% rate without identification.21 Interestingly, Jatzko noted that in cases with initial postoperative paralysis, intraoperative identification of the RLN was associated with better RLN recovery rates (57% recovered if the RLN had been identified versus only 34% if it had not).23 A number of other workers agree that RLN identification is essential during thyroidectomy.48–50
Surgical Anatomy
Vagal Neural Anatomy
The vagus nerve was described in modern form first by Willis in the 1600s.27 The vagus derives its blood supply from a discrete vagal artery that is a branch of the inferior thyroid artery, which is reinforced by branches from the internal carotid, common carotid, aortic arch, bronchial and esophageal arteries.28 The cervical branches of the vagus of concern during thyroid surgery include the SLN, both internal and external branches, and the RLN. The SLN’s internal branch brings general visceral afferents to the lower pharynx, supraglottic larynx, vocal cords, and base of tongue, and special visceral afferents to the epiglottic taste buds. The SLN’s external branch brings branchial efferents to the cricothyroid muscle and inferior constrictor. As is described later, the internal branch of the SLN may also provide motor contributions to the posterior cricoarytenoid muscle and intra-arytenoid muscle, and the external branch of the SLN may provide, at least in some patients, limited motor input to the thyroarytenoid muscle. The RLN contains branchial efferents to the inferior constrictor, cricopharyngeus, all laryngeal intrinsics except the cricothyroid muscle, general visceral afferents from the larynx (vocal cords and below), upper esophagus, and trachea.29 RLN branches also convey sympathetic and parasympathetic branches to the lower pharynx, larynx, trachea, and upper esophagus. Apart from the larynx and pharynx, the vagus provides afferent and parasympathetic innervation to the heart, esophagus, stomach, intestines, liver, spleen, and kidneys.
Cortical areas (including Broca’s area, the motor cortex, and the anterior cingulum) that control laryngeal function project to brainstem nuclei bilaterally, primarily the nucleus ambiguous.30 The nucleus ambiguous then projects to the ipsilateral portion of the larynx.31,32 Gacek’s work in the cat has identified laryngeal motor supply arising in the ipsilateral nucleus ambiguous with adductor function primarily in the dorsal division of the nucleus and abductor neurons primarily in the ventral division. He identified a second source of laryngeal innervation in the retrofacial nucleus, from which neurons extend to the cricothyroid and posterior cricoarytenoid muscles with abductor fibers arising centrally and adductor fibers more peripherally.31,33
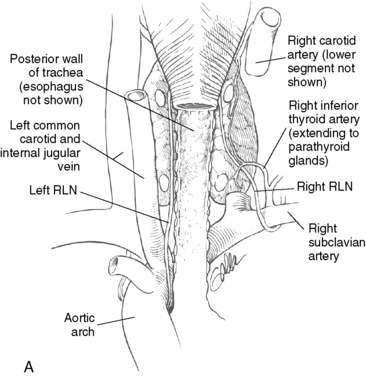
The vagus nerve forms through a gathering of a number of small vagal rootlets together with the bulbar roots of the accessory nerve on the lateral aspect of the medulla and exits the skull through the pars nervosa of the jugular foramen. It descends the neck in the carotid sheath, initially on the medial aspect of the internal jugular, then becomes situated posteriorly between the internal jugular and carotid artery lower in the neck34 (Figure 33-3). The initial branches of the vagus include the meningeal filament extending to the dura, the auricular branch to the posterior external auditory canal (Arnold’s nerve), Jacobson’s nerve to the promontory of the middle ear, and the pharyngeal ramus. The superior ganglion of the vagus nerve lies within the jugular foramen, whereas the inferior or nodose ganglion is just beneath the jugular foramen. The pharyngeal ramus supplies motor fibers to the pharyngeal constrictors and sensory fibers to the underlying pharyngeal mucosa.34 The nodose ganglion contains cell bodies for sensory and parasympathetic fibers and is present just laterally to the superior cervical sympathetic ganglion. Immediately below the nodose ganglion, the SLN is given off.

Dionigi et al. have documented no morbidity or added operative time for vagal dissection and stimulation during neural monitoring. They have shown the vagus is located directly posterior to the carotid and jugular vein in 73% of cases and lies directly posterior to the carotid artery in 15% of patients cases, lies directly posterior to the jugular vein in 8% of cases, and lies anterior to the carotid and jugular vein in the carotid sheath in 4% of cases.35
RLN Neural Anatomy
As the heart and great vessels descend during embryologic life, the RLN is dragged down by the lowest persisting aortic arch (see Chapter 2, Applied Embryology of the Thyroid and Parathyroid Glands). The right vagus runs from the posterior aspect of the jugular vein in the neck base to cross anterior to the first part of the subclavian artery. The RLN branches and courses up and behind the subclavian artery (fourth branchial arch) running medially along the pleura and cranially behind the common carotid artery into the right thoracic inlet in the base of the neck. The left vagus courses from the carotid sheath in the left neck base anterior to the aortic arch (sixth arch, ligamentum arteriosus). The RLN branch curves up under the aortic arch just lateral to the obliterated ductus arteriosus (Figure 33-4).
Because of its course around the right subclavian artery, the right RLN enters the neck base at the thoracic inlet more laterally than the left recurrent does36 (see Figure 33-4). The right RLN then ascends the neck, entering the thoracic inlet, emerging from under the common carotid artery, traveling from lateral to medial as it travels superiorly, and ultimately crossing the inferior thyroid artery. It assumes a paratracheal position in the last centimeter of its course as it approaches the lowest edge of the inferior constrictor. Shindo et al. found in their distal course both right and left recurrent laryngeal nerves typically form an angle of between 15 and 30 degrees relative to the trachea but that the right recurrent laryngeal nerve as noted earlier tends to travel in a more oblique course on average through its paratracheal region as compared to the more strictly tracheoesophageal groove course on the left.37 Hisham found that 60% of nerves are located in the tracheoesophageal groove, 5% more lateral to the trachea, and 28% directly posterior to the thyroid lobe.38
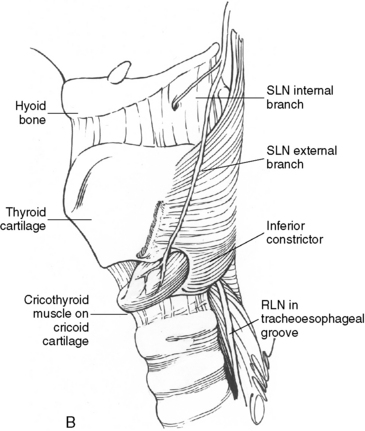
At the lower edge of the cricoid cartilage posterolaterally, the recurrent laryngeal nerve travels under the inferior-most fibers of the inferior constrictor (i.e., the cricopharyngeus muscle), extending deep to the inferior constrictor and up behind the cricothyroid articulation to enter the larynx. In approximately 30% of cases, the RLN actually penetrates the lowest fibers of the inferior constrictor on its way to the larynx39 (see Figure 33-4, B). Incorrect descriptions of this anatomy exist, in which the RLN is said to pass deep to the cricothyroid, rather than the inferior constrictor muscle.40,41 The point at which the RLN disappears under the lowest fibers of the inferior constrictor will, in this chapter, be termed the laryngeal entry point and represents the distal-most exposure of the RLN in the thyroid surgical field. The RLN extends underneath the inferior fibers of the inferior constrictor and up behind the cricothyroid cartilaginous articulation within the larynx. For the last centimeter or so before laryngeal entry, the RLN travels close to the lateral border of the trachea.
The vagus diameter in its cervical course is approximately 4 mm with the epineurium, 3 mm without. The diameter decreases to approximately 2 mm after the RLN takeoff point.42 The RLN diameter averages approximately 2 mm, ranging from 1 to 3 mm.42,43 The length of the vagus from the second cervical vertebra to the separation of the RLN is (based on 30 dissections in 15 adult humans), on average, 11.5 cm on the right and 13.5 cm on the left. The length of the RLN from vagal takeoff to laryngeal entry point is 8.5 cm on the right and 10 cm on the left.42 These different lengths result in discrete different evoked monitoring waveform latencies which allow recognition of the nerve being stimulated providing clear documentation of neural function (discussed below).
Superior Laryngeal Nerve
The SLN arises immediately beneath the nodose ganglion of the upper vagus and descends medial to the carotid sheath. It divides into its internal and external branches about 2 or 3 cm above the superior pole of the thyroid, although this point may vary (see Chapter 32, Surgical Anatomy of the Superior Laryngeal Nerve). The internal branch travels medial to the carotid system, entering the posterior aspect of the thyrohyoid membrane and providing sensation to the ipsilateral supraglottis and base of the tongue. The external branch descends to the region of the superior pole and extends medially along the inferior constrictor fascia to enter the cricothyroid muscle. As the external branch slopes downward on the inferior constrictor musculature, it has a close association with the superior thyroid pedicle.44 Several workers have shown that in approximately 20% of cases the external branch of the SLN is closely associated with the superior thyroid vascular pedicle at the level of the capsule of the superior pole, placing it at risk during ligation of these superior pole vessels.43–45 In approximately 20% of cases, the external branch is actually under the inferior constrictor fascia and may not be directly visualized, yet it can be stimulated electrically.44,45 Depending on the degree of superior pole development, the sternothyroid muscle may “hood” the superior pole region. Isolated sternothyroid division can help with exposure in this region. With external branch injury there is a loss of vocal cord tensing, which is manifested by increased vocal tiredness and a loss of higher registers. Postoperative examinations after unilateral external branch injury are subtle and controversial, but they are generally believed to include a bowed and somewhat lower cord and a larynx rotated to the affected side. Such an injury brought to an end the operatic career of Amelita Galli-Curci, although there is intrigue regarding this point (see the “SLN Monitoring” section presented later in the chapter and also Chapter 32, Surgical Anatomy of the Superior Laryngeal Nerve).
Microanatomy of the RLN
Gacek has shown in the cat that the RLN, 2 cm below the cricoid, is composed of approximately 55% motor fibers and 45% sensory fibers. The percentage of motor fibers rises to 80% more distally at the laryngeal entry point, with sensory fibers having branched from the RLN to adjacent tracheal and esophageal locations.31,33 Nonmyelinated fibers within the RLN represent sympathetic (carotid plexus) and parasympathetic (postganglionic) fibers whose cell bodies are within the nodose and plexiform ganglia.30 Gacek found a higher number of fibers in the right versus the left RLN, a finding confirmed by others.31,33,46
Murtagh described between 2000 and 3000 myelinated fibers in the human RLN.46 The number of motor axons in the distal-most branches of the intralaryngeal portion of the RLN in the dog ranges from 143 to 370.47 Malmgren described three fiber types within the human RLN. The first group comprised 4- to 12-μm fibers staining for acetylcholinesterase; the second group consisted of small fibers from 1 to 5 μm, also staining for acetylcholinesterase; and a third group consisted of small fibers from 4 to 12 μm in size without acetylcholinesterase staining and believed to be sensory and autonomic fibers.48 Malmgren and Gacek noted that the RLN’s epineural covering was notably thicker than for most other human peripheral nerves and that the RLN was organized into between 1 and 11 fascicles.48
Within the vagus, adductor and abductor fibers are not spatially segregated, although all laryngeal motor fibers tend to be in the anterior half of the vagus of the upper neck and the medial half of the vagus in the lower neck.30,31,33,49,50 In the RLN, at the laryngeal entry point, the adductor and abductor fibers lack spacial segregation and are diffusely distributed throughout the entire nerve.31,33,49 The RLN contains two to four times as many adductor fibers as abductor fibers.31,33,51
Visual Identification
The RLN is white and approximately 2 mm wide. Although it generally follows a linear course, it can have a somewhat curved profile and be similar in appearance to the spinal accessory nerve in surgery of the lateral portion of the neck. The normal RLN virtually always has a vessel running on its surface (vasa nervosum), seen as a ventral “red strip.” This may be less apparent if the nerve has been attenuated over time, as in massive goiter or if the nerve is placed on stretch. All that visually appears to be the RLN may not be. Electrical confirmation complements the visual impression and avoids visual false positives. Raffaelli and Henry noted that sympathetic chain branches to the distal RLN branch can be large enough to mimic a nonrecurrent nerve.58 They also describe rare, medially directed branches of the sympathetic system that can mimic the normal RLN. They have found at least one such case, in which the nerve that “perfectly mimicked the RLN, when dissected fully, originated from the sympathetic stellate ganglion, not the vagus.”58 In these cases, the functional information that is available with RLN monitoring adds to the visual information available to the surgeon. Sympathetic nerve branches, when stimulated, should yield no EMG laryngeal activity.
The RLN is amendable to surgical dissection without injury. Chiang et al. have shown that RLNs that require extensive dissection of > 5 cm in the setting of goiter had no higher rates of paralysis than nerves requiring less dissection.52
Nonrecurrent RLN
The nonrecurrent RLN occurs in 0.5% to 1% of cases and is associated with a right subclavian artery takeoff from the distal aortic arch.53 The right subclavian in these cases follows a retroesophageal course to the right or, less commonly, between the esophagus and the trachea.53 Henry found that the symptoms of dysphagia secondary to subclavian interaction with the esophagus (dysphagia lusoria) were not consistently present in cases of nonrecurrent RLN. When dysphagia is present, dysphagia lusoria is difficult to separate from dysphagia referable to a pathologic condition of the thyroid. Epstein suggests nonrecurrent RLN is associated with compressive symptoms in 10% of patients typically with dysphasia.54 The retroesophageal subclavian artery is associated with Kommerell’s diverticulum (dilation at its aortic takeoff) in 60% and with other aortic, cardiac, vertebral artery, and thoracic duct abnormalities including right-sided duct location.54 Barium swallow can reliably detect a retroesophageal subclavian artery.53 Watanabe, studying preoperative CT scans in 594 patients, was able to predict preoperatively the occurrence of a nonrecurrent nerve on the right if the right subclavian artery on axial CT scanning was detected on the dorsal side of the membranous wall of the trachea.55 Iacobone has also shown that ultrasound is reliable in detecting this vascular abnormality.56
The nonrecurrent RLN derives from the vagus as a direct medial branch in the neck and extends—depending on its level of takeoff from the vagus and generally with a downward looping course—from behind the carotid artery to the laryngeal entry point but can follow more horizontal or ascending paths.53,57–59 The takeoff of the nonrecurrent RLN from the vagus may occur as high as the thyroid superior pole or as low as the inferior thyroid artery. Avisse has offered a classification scheme that includes type I characterized by a high takeoff from the vagus traveling from the vagus in association with the superior pole vessels, type IIA deriving from the vagus at the level of the laryngotracheal junction traveling along the path of the inferior thyroid artery, and type IIB deriving from the vagus at the level of the laryngotracheal junction then traveling in a downward looping course below the level of the inferior thyroid artery before it extends up to its laryngeal entry point.60 The nonrecurrent nerve may be very closely related to the inferior thyroid artery. It may be bifid or have multiple branches in 18% to 40% of cases53,61 (Figure 33-5). The nonrecurrent nerve is at increased risk for paralysis with one study of 31 nonrecurrent nerves at risk demonstrating a 12.9% paralysis rate.62 The nonrecurrent RLN may be associated, some feel, with a second, smaller right RLN in the normal RLN position. Katz found this in 5 of 11 nonrecurrent RLNs and Karlin found it in 2 of 5 nonrecurrent RLNs.61,63–65 Not all agree that a nonrecurrent nerve may coexist with a small normally positioned right RLN, but the finding of a small narrow right RLN should alert the surgeon to search for a larger nonrecurrent laryngeal nerve trunk.53 Nonrecurrence on the left is possible in the setting of a right aortic arch associated with sinus inversus with a left subclavian artery “lusoria course” and absence of the arterial ligament on the left side.87 Henry described this as occurring in 0.04% of cases.53
Communicating branches between the cervical sympathetic system and RLN have unclear function, perhaps involved in vasomotor laryngeal control.66 These fibers typically originate from the middle cervical sympathetic ganglion and have a diameter slightly less than a normal RLN.58 Large cervical sympathetic RLN anastomotic branches have been found in 1.5% of cases (more frequently than the rate of right RLN nonrecurrence).58 Maranillo’s cadavaric dissections suggest a rate as high as 17% of specimens.67 When present, such large sympathetic RLN anastomotic branches connect to the RLN within 2 cm of the RLN’s laryngeal entry point. Such large sympathetic RLN anastomotic branches may be confused with true RLN nonrecurrent nerves. One should be able to differentiate between these through neural stimulation.
Vagal electric stimulation has been shown to easily diagnose nonrecurrent right RLNs. Typically the nonrecurrent takeoff from the vagus is between the superior thyroid artery and the inferior thyroid artery along the cranial caudal axis. Routine stimulation of the vagus below the inferior thyroid artery is part of standard neural stimulation algorithms during neural monitoring. Successful stimulation at this level confirms neural monitoring setup. If on the right hand side this focus of vagal stimulation is negative, stimulation should be performed at a higher level of the vagus; generally, stimulation at the level cranially at the upper margin of the thyroid cartilage will result in stimulation. If this higher vagal stimulation results in laryngeal EMG activity the surgeon has electrically diagnosed a nonrecurrent right RLN.68
RLN Displacement
was associated with the thyroid gland and was thus at serious risk when the retrosternal mass was mobilized into the neck, a maneuver usually achieved by dislocating the mass with a finger from below and behind. I believe that this hazard must be recognized by all thyroid surgeons and that every strand of tissue stretched over the retrosternal component of the goiter should be presumed to be nerve until anatomically proven otherwise.69
Lahey, in 1938, recommended RLN identification “even in deep intrathoracic goiter extending nearly to the diaphragm.”70 We believe that because of the possibility of nerve fixation and splaying on the undersurface of a goiter, blunt dissection without nerve identification risks stretch injury. Identification of the RLN in such cases is a necessary initial step. The nerve that is fixed to or splayed on the undersurface of the goiter should be dissected off before the gland is delivered. The nerve can be identified through a superior approach (discussed later) and can be dissected retrograde off the goiter before digital delivery of the goiter. The nerve so dissected can appear after goiter resection to be significantly redundant, but it will stimulate normally and function postoperatively despite the intraoperative appearance of laxity. I have noted that goiters associated with retrotracheal extension as identified by preoperative CT scanning may be associated with RLN displacement to the ventral surface of the goiter. This is a disorienting position to come upon and places the nerve at extreme risk, even in experienced hands. Therefore, analysis of preoperative CT scanning in patients with retrotracheal goiter may empower the surgeon to have low suspicion for such ventral RLN displacement (see Chapter 7, Surgery of Cervical and Substernal Goiter).
Tubercle of Zuckerkandl
Aside from thyroid tissue that may actually infuse the ligament of Berry (see the discussion of the ligament of Berry presented later in the chapter), surface nodules and lobulation of the thyroid gland near the ligament may make distal RLN dissection more difficult. A lobule of thyroid tissue, varyingly present, typically just caudal to the ligament of Berry at the posterolateral margin of the thyroid lobe, has been termed the tubercle of Zuckerkandl (TOZ) and was described by Zuckerkandl in 1904 as the “processus posterior glandulae”40,71 and by Madelung in 1867 as the “posterior horn of the thyroid”72 (see Chapter 2, Applied Embryology of the Thyroid and Parathyroid Glands, Figures 2-2 and 2-3, D).
The adult orthotopic thyroid is derived from the fusion of medial and lateral elements (see Chapter 2, Applied Embryology of the Thyroid and Parathyroid Glands). The lateral thyroid anlage derives from the fourth pharyngeal pouch and includes the ultimobranchial body (from the ventral part of the fourth pharyngeal pouch and possibly a portion of the fifth pouch) and parafollicular C cells of neural crest origin. This lateral element fuses with the medial anlage (which derives from the tuberculum impar of the embryonic tongue base) as the thyroid descends before the seventh week of gestation. This point of fusion is closely juxtaposed to several regional important structures: upper parathyroid glands (PIV) (which arise from the adjacent dorsal wing of the fourth pharyngeal pouch), the RLN (the vagus and RLN arise between the fourth and fifth pharyngeal pouches), and the inferior thyroid artery (ITA) (which derives from the fourth aortic arch). When thyroid tissue is present as a posterior lateral projection of the lateral thyroid lobe, it can be termed the tubercle of Zuckerkandl and is felt to represent this point of the lateral anlage’ s fusion with the medial thyroid elements and can have relationships with surrounding structures, especially including the RLN and PIV, which can be of surgical importance.
When present in its typical position, the tubercle is caudal to the ligament of Berry (LOB). The tubercle is said to point to the nerve as the nerve interacts with the LOB and laryngeal entry point. The nerve is typically deep to the tubercle and may be entrapped in a cleft between the tubercle’s deep surface and the adjacent deep surface of the thyroid lobe (see Chapter 2, Applied Embryology of the Thyroid and Parathyroid Glands, Figures 2-2 and 2-3, D). The nerve is said to be in this deep position relative to the TOZ in 93% of cases, but in the remaining 7% of cases the nerve may ride ventral to the tubercle and thus be in an extremely vulnerable position at surgery.72 Hisham also found the RLN coursing anteriorly to the tubercle in 6% of patients and felt this variation was more common in revision patients38 (see Chapter 2, Applied Embryology of the Thyroid and Parathyroid Glands, Figures 2-2 and 2-3, D). When the tubercle is extending dorsally and the nerve is brought ventrally, the TOZ is felt to be the initial manifestation of what would be in the neck, a retrotracheal goiter and in the mediastinum a posterior mediastinal goiter, both of which are associated with such high-risk “ventral” RLNs (see Figure 7-7, B). Even if the nerve is in its more typical position deep to the TOZ, it may be relatively entrapped in the cleft between the TOZ and adjacent thyroid and be stretched as the TOZ is serially dissected and retracted to expose the RLN.
This lobule of thyroid tissue may have a varying relationship to the RLN and, in general, tends to obscure its distal course and make more difficult its distal dissection. The exact position of the TOZ (when it is present) varies along a cranial caudal axis. Most typically, the TOZ is present at the posterolateral margin of the thyroid midpole region and so is below the ligament of Berry; in this position, the TOZ points to superiorly the RLN as the nerve extends to the ligament of Berry and laryngeal entry point.73 However, the TOZ may occur higher on the thyroid lobe and so may overlie the ligament of Berry region obscuring the region of the nerve-ligament of Berry and nerve entry site. The TOZ may occur even more superiorly from the posterolateral margin of the superior pole, frankly above the RLN entry site.73,74 The TOZ is felt to also have a relatively constant relationship to the ITA—typically dorsal relative to the TOZ—and will typically have the PIV on its lateral or superolateral margin (see Chapter 2, Applied Embryology of the Thyroid and Parathyroid Glands, Figures 2-2 and 2-3, D).72
A TOZ grading scheme has been offered: grade 1 (less than 5 mm), grade 2 (between 5 and 10 mm), and grade 3 (greater than 1 cm).75 Significant TOZ (i.e., grade 3) is felt to be present in 14% to 61% of patients and seems to vary in its prevalence in relation to country of origin and may be more common on the right than on the left (69.6% on the right and 53.2% on the left in one study).72,76,77 Of course, as thyroid tissue the TOZ is subject to any benign or malignant process. This variability in existence of the tubercle from patient to patient has hindered this as being a reliable landmark for nerve identification (see Chapter 2, Applied Embryology of the Thyroid and Parathyroid Glands, Figures 2-2 and 2-3, D).78
Extralaryngeal RLN Branching
Various surgical and cadaver dissection series show the RLN branches before the laryngeal entry point in from 30% to 78% of cases.63,64,79–82 Up to five branches have been described.82 These studies do not usually distinguish between the small branches arising from the RLN and extending to the adjacent trachea (sensory), esophagus (sensory and motor), inferior constrictor (sensory and motor), and sympathetic chain, and the typically larger branches arising as a terminal division of the nerve destined to innervate laryngeal musculature. Of course, branches that contain laryngeal intrinsic motor fibers must together enter the larynx at the laryngeal entry point and not extend more ventrally or posteriorly, which implies their sensory or nonlaryngeal motor nature. Obviously, only the branches extending to the laryngeal entry point will affect laryngeal motor function. In my experience and that of Serpell et al., 50% to 60% of patients have some small branches of the RLN to the trachea, esophagus, or inferior constrictor, but only 20% to 30% have true RLN extralaryngeal branches that enter the larynx and with stimulation resulting in laryngeal EMG activity.83,84 This is in agreement with both the older work of Morrison, who noted true extralaryngeal branches in approximately one third of patients on at least one side,85 as well as the more recent studies of Bergergama and Serpell.84 Endotracheally based monitoring systems identify only thyroarytenoid depolarization, whereas assessment of laryngeal twitch or posterior laryngeal electrodes will inform regarding posterior cricoarytenoid (PCA) depolarization. In my experience, the small RLN branches to the esophagus and inferior constrictor, when stimulated, usually result in local contraction of the associated esophageal or inferior constrictor musculature. Brok found four or five branches of the RLN to the cricopharyngeus in nine of nine patients with careful dissection.29
Any true extralaryngeal RLN branches not recognized during surgery are at risk for injury. The total diameter of the normal RLN in the neck is only approximately 1 to 2 mm, so these branches are often less than 1 mm. Most laryngeal branches of the RLN arise from the distal RLN segment, with 90% of branching occurring above the intersection of the RLN and the inferior thyroid artery.63 Reed found that only 5.4% of 506 dissected nerves branched at the level of the RLN and inferior thyroid artery crossing.100 It is known that the distal-most RLN intralaryngeal branches are always given off by the time the RLN is above the cricothyroid joint.27 Serpell’s group has shown that the most common branch point occurred in the distal 2 cm course of the RLN measured from the bottom of the inferior constrictor and averaged approximately 18 mm with a range of 5 to 34.83,84 True “extralaryngeal RLN branches” (i.e., major branches destined to enter the larynx) can be assumed to be analogous to intralaryngeal branches, except that they are premature, occurring more proximally below the lower edge of the inferior constrictor. The lowest segment of the inferior constrictor is termed the cricopharyngeus.
Thus, extralaryngeal nerve branches, when present, usually exist at the level of the ligament of Berry and are usually not present below the inferior thyroid artery. The lack of branches below the inferior thyroid artery is part of the rationale for the inferior approach to the RLN in the thoracic inlet as described by Lore.86 We have seen that RLN branching occurrence and pattern vary from side to side within the same patient, in agreement with the work of Morrison and Katz.63,85 Katz noted, in a study of 1771 nerves, that if extralaryngeal branches occur on one side, 39% of patients will have branching on the opposite side.64
The most important message regarding patients with extra laryngeal branching, because of this increased anatomic complexity and narrow diameter of the branched RLN, is that they are at increased risk for both transient and permanent vocal cord paralysis. The work of Sancho et al. suggested branched nerves are twice as likely to have transient vocal cord paralysis (VCP) postop (15.8%) than nonbranched nerves (8%).87 The work of Cassella also suggested an increased rate of paralysis from 7 to 12 times that of patients with unbranched RLNs.88
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


