Surgery to Correct Duane’s Syndrome and Brown’s Syndrome
Monte A. Del Monte
Steven M. Archer
DUANE’S SYNDROME
INDICATIONS
Duane’s syndrome is a condition of aberrant innervation that results in co-contraction of the medial and lateral rectus muscles in the affected eye. This aberrant innervation produces several manifestations, any one of which may be severe enough to warrant surgery in a given patient. These manifestations include a face turn with strabismus in primary position, an upshoot or downshoot during adduction, retraction during adduction, and enophthalmos. None of these findings is an absolute indication for surgery; the need for surgery depends on the severity of the manifestations and the degree to which the patient feels functionally compromised by the face turn or disfigured by the enophthalmos or bizarre eye movements.
An unacceptable face turn is by far the most common indication for surgical treatment. The face turn is a secondary manifestation of strabismus in primary position and develops to permit fusion. If it is sufficiently large, the face turn may be a functional handicap in addition to being disfiguring. Patients who have Duane’s syndrome with exotropia in primary position usually have a face turn away from the affected eye. More commonly, an esodeviation in primary position leads to a face turn toward the side of the affected eye. This face turn usually is more pronounced with distant fixation. The face turn and measured deviation with near fixation may be less, but this is not a contraindication for surgery to correct the distant fixation deviation; overcorrection at near is uncommon.
An occasional Duane’s syndrome patient may have bilateral involvement or a vertical deviation that precludes fusion with any head posture. In these cases, the strabismus itself rather than the secondary head posture can be the main indication for surgical correction, which should be performed at an earlier age than when fusion is present.
When the affected eye is adducted, an upshoot, downshoot, or retraction can be sufficiently disturbing to the patient or parents to warrant surgical treatment. In severe cases, there is significant enophthalmos and pseudoptosis, even in primary position. A reduction of 50% or more of the width of the palpebral fissure during adduction compared with primary position has been suggested as an indication for surgical treatment of the retraction.1
Increasing the field of single binocular vision is desirable but not a primary goal in the treatment of Duane’s syndrome. Patients with Duane’s syndrome rarely complain of diplopia in the restricted field of gaze. Therefore, procedures designed to improve the field of single binocular vision should not be undertaken in Duane’s syndrome at the expense of compromising other treatment objectives or increasing the risk of secondary complications.
CONTRAINDICATIONS
Many patients with Duane’s syndrome are orthophoric in primary position or have only an insignificant face turn.2,3 In these cases, surgery is not indicated unless another manifestation of Duane’s syndrome, such as an upshoot or downshoot, is causing hardship. The fact that a patient seeks evaluation does not necessarily indicate a desire for surgical correction. Often, it is not the manifestations of the condition themselves that have motivated the consultation, but rather a concern that they indicate some ominous underlying intracranial disease, especially for parents who have suddenly noticed their child’s eye movement abnormality. If discussion with the patient or the child’s parents reveals that fear of life-threatening disease rather than a manifestation of Duane’s syndrome itself is the chief concern, then explanation and reassurance may be all that is needed.
Because fusion usually can be obtained by means of a face turn, most children with Duane’s syndrome have relatively normal binocular function and stereopsis. Therefore, in contradistinction to congenital esotropia–where the goal is to restore ocular alignment at as early an age as possible–the goal in Duane’s syndrome should be to avoid disrupting normal binocular development. Thus, young age is a relative contraindication for surgery. Early treatment may be warranted if the face turn is very large, but usually it is preferable to delay surgery until 4 to 5 years of age. The visual system is relatively mature at this age and less susceptible to damage from a temporary disruption of binocularity, as can occur postoperatively if there is an unfavorable response to surgery. Also, older children can cooperate more adequately for the detailed examination necessary to appreciate the many subtle variations of Duane’s syndrome for which the surgical plan may need to be adjusted.
While Duane’s syndrome patients rarely complain of diplopia preoperatively, they often do not adapt easily to a postsurgical reduction of their field of single binocular vision to the contralateral side. Procedures should be planned to avoid producing significant new incomitance (exotropia in right gaze for a typical esotropic left Duane’s syndrome patient), particularly in adults, who are more likely than children to be distressed by changes in the pattern of incomitance.
PROCEDURES
Because the manifestations of Duane’s syndrome show great variability, no single surgical plan can be recommended. Rather, the choice of procedure or combination of procedures must be tailored to address the specific manifestations that are symptomatic in each patient.
Ipsilateral Medial Rectus Muscle Recession for Esotropic Duane’s Syndrome
Recession of the ipsilateral medial rectus muscle is the mainstay of surgical treatment for Duane’s syndrome.1,4 This improves the face turn and the esotropia by relieving restriction and weakening the antagonist of the lateral rectus muscle. There also can be a modest improvement in abduction, but sometimes at the expense of reduced adduction. Medial rectus recession alone also may improve enophthalmos and vertical overshoots in adduction, in part by limiting adduction of the eye. However, additional measures usually are needed to deal adequately with these problems if they are severe.
It seems that indications for medial rectus muscle recession in sixth nerve palsy also should apply to Duane’s syndrome; however, there are some important differences. In sixth nerve palsy, the absence of abduction suggests that medial rectus muscle recession is ineffective and a transposition procedure to provide some abduction force is necessary for any long-term improvement. Although preoperative abduction ability is a good prognostic sign in Duane’s syndrome, medial rectus muscle recession still can be effective even in cases in which there appears to be no abduction at all. There are two reasons for this. First, medial rectus muscle restriction is frequently an important factor in Duane’s syndrome; some abduction ability is unmasked when the restriction is relieved. When marked restriction is present, medial rectus muscle recession must be at least part of the surgical plan. Second, aberrant innervation of the lateral rectus muscle in Duane’s syndrome often provides some tonic abducting force to counterbalance the weakened medial rectus muscle in primary position, even when there is no active contraction of the lateral rectus muscle on attempted abduction. Of course, absent any component of normal lateral rectus muscle innervation, a transposition is still needed to provide abduction much beyond midline; however, it should be remembered that the primary goal in sixth nerve palsy and Duane’s syndrome are different. Good abduction with a large field of single binocular vision is needed for relief of diplopia in acquired sixth nerve palsy, but abduction to just beyond midline is often sufficient to eliminate the face turn in Duane’s syndrome.
To effectively reduce or eliminate the face turn, a large recession–in the range of 8 to 10 mm as measured from the original insertion–often is needed. Standard recession techniques or a “hang-back” technique may be used, which can make the procedure easier to perform when a large recession is needed. Large recessions can cripple adduction and are contraindicated when there is strong co-contraction or restriction of the lateral rectus muscle, as indicated by exotropia in the contralateral field of gaze. When significant mechanical restriction owing to contracture or fibrosis of the medial rectus muscle is present, smaller recessions usually are sufficient.5 A large recession easily can cripple a fibrotic muscle, which often has contractile properties that are almost as severely compromised as its elastic properties. For adult patients, adjustable suture recession techniques are helpful for finding the best compromise between adequate relief of the face turn and crippled adduction.
Surgery on the Contralateral Eye
Recession of the contralateral medial rectus muscle in esotropic Duane’s syndrome can reduce esotropia in primary position by reducing innervation to the ipsilateral medial rectus muscle and recruiting any minimal normal innervation of the ipsilateral lateral rectus muscle that may exist, without any detrimental effect on adduction of the Duane’s syndrome eye. Possible improvement in the field of single binocular vision by matching the duction deficit of the ipsilateral eye provides another rationale for this procedure. A contralateral medial rectus muscle recession needs to be large (often larger than an ipsilateral recession) because it, in effect, is treating the much larger secondary deviation. However, contralateral medial rectus recession by itself, regardless of size, cannot correct a face turn if the ipsilateral eye is unable to abduct at least a little past midline. This should be tested prior to performing contralateral surgery. If the patient cannot abduct the ipsilateral eye well enough to comfortably maintain a straight head posture with the contralateral eye patched, contralateral eye surgery alone cannot correct the face turn. The adequacy of contralateral surgery also can be evaluated, with both eyes open, by testing whether the face turn can be eliminated by holding base-out prism in front of the contralateral eye. Even when not adequate by itself, contralateral medial rectus recession may allow a smaller recession of the ipsilateral medial rectus muscle to be effective. Recession of the contralateral medial rectus muscle is a particularly useful adjunct to ipsilateral medial rectus muscle recession when primary position esotropia exceeds 20 δ or a large recession is contraindicated because of poor adduction or marked retraction.1 Recession of the contralateral medial rectus muscle also may reduce the long-term risk of recurrent face turn owing to development of ipsilateral medial rectus muscle contracture by reducing its tonic innervation. Similar arguments have been made for recession of the contralateral lateral rectus muscle to improve the abnormal head posture and expand the field of single binocular vision in exotropic Duane’s syndrome.6
Unlike other forms of incomitant strabismus, contralateral surgery in Duane’s syndrome can interact with the aberrant innervation in unexpected ways. Particularly in patients with small-angle esotropia, the lateral rectus muscle may have significant tonic aberrant innervation in primary position that aids in holding the eye close to straight. Contralateral medial rectus muscle recession reduces innervation to the ipsilateral medial rectus muscle but also reduces the constructive aberrant innervation to the ipsilateral lateral rectus muscle in primary position.7 The proportion of aberrant and normal innervation to the lateral and medial rectus muscles determines the net change in balance between adducting and abducting forces in a specific patient. Usually, the reduction in aberrant lateral rectus muscle innervation does not quite fully negate the reduction in medial rectus muscle innervation in primary position; however, even a paradoxical worsening of the face turn has been described in some patients.8 Conversely, recessing the contralateral lateral rectus muscle in exotropic Duane’s syndrome increases innervation to the ipsilateral medial rectus muscle and consequently the aberrant innervation to the ipsilateral lateral rectus muscle. Again, the results depend upon how the balance between abducting and adducting forces is changed.
Posterior fixation of the contralateral medial rectus muscle has been advocated as a way of equalizing rotations of the two eyes and improving the field of binocular single vision.6 It can have applications in esotropic and exotropic Duane’s syndrome, whenever there is limitation of abduction in the Duane’s syndrome eye preoperatively or expected after the planned surgery. Unlike recession, posterior fixation does not reduce the constructive primary position aberrant innervation to the ipsilateral lateral rectus muscle; however, it is unlikely to have much effect unless there is at least some component of normal innervation to the ipsilateral lateral rectus muscle.
Recess-Resect Procedure
Resection procedures generally are regarded as contraindicated in Duane’s syndrome because of concern for making the retraction, adduction deficit, enophthalmos, or upshoot and downshoot worse. However, a small recess-resect procedure on the eye with Duane’s syndrome can provide correction of the head posture comparable to that from a single large medial rectus recession, but with less limitation of adduction and better abduction in favorable cases.9,10 To minimize the risk of making the retraction significantly worse, this approach should only be considered in eyes with modest signs of co-contraction and even then resection of the lateral rectus muscle should be limited to less than 4 mm.
Vertical Rectus Muscle Transposition
In esotropic Duane’s syndrome, transposition of the vertical rectus muscles to a position adjacent to the lateral rectus, with or without recession of the ipsilateral medial rectus muscle, has been suggested as a means of correcting the primary position esotropia, improving abduction and enlarging the field of single binocular vision.11,12,13 This procedure may provide better abduction than medial rectus recession alone. However, it is more difficult to perform; may exacerbate retraction, upshoot, or downshoot; and can create new vertical deviations.11 Transposition is best suited for cases in which abduction is severely limited and there is no pre-existing vertical deviation. If there are significant signs of co-contraction, transposition should be done in conjunction with a procedure to weaken or eliminate lateral rectus muscle function (e.g., a large recession or disinsertion with terminal myectomy or fixation to the lateral orbital periosteum).
Particularly in adult patients on whom a medial rectus recession is performed concurrently, there is some risk of anterior segment ischemia.14 If medial rectus muscle restriction is absent or mild, transposition with lateral posterior augmentation sutures can reduce the likelihood that associated medial rectus muscle surgery will be needed.15 However, augmented transposition procedures produce more limitation of adduction, increase the risk of a secondary vertical deviation, and anterior segment ischemia can still occur.16 The risk of anterior segment ischemia can be further reduced by performing an augmented partial tendon transposition that spares one ciliary vessel in each vertical rectus muscle.17
Lateral Rectus Muscle Recession for Exotropic Duane’s Syndrome
An exodeviation in primary position with a face turn away from the side of the affected eye is a less common presentation of Duane’s syndrome. In these cases, the face turn usually is treated with recession of the ipsilateral lateral rectus muscle. In patients who have both primary position exotropia and a marked upshoot or downshoot, a lateral rectus recession usually is combined with an additional measure to minimize sideslip of the lateral rectus muscle across the globe–either a Y-splitting procedure or a posterior fixation suture. A large recession of the lateral rectus muscle also provides some improvement in the retraction with adduction. As with medial rectus muscle recessions, recessions of the lateral rectus muscles should be smaller when there is significant restriction.
Bilateral Lateral Rectus Muscle Shift for V-Pattern
Dramatic abduction of both eyes in elevation can occur in what is probably a variant of Duane’s syndrome with aberrant innervation of the lateral rectus muscles by fibers from the superior branch of the oculomotor nerves.18 A similar picture can develop in bilateral cases of more typical Duane’s syndrome after bilateral medial rectus muscle recessions. It is treated by small recession and full tendon width up-shift of the lateral rectus muscles bilaterally.
Ipsilateral Recessions of Both the Medial and Lateral Rectus Muscles
Enophthalmos in Duane’s syndrome is occasionally severe enough to warrant specific remediation. Large recessions of both the medial and lateral rectus muscles can reduce enophthalmos as well as upshoot, downshoot, and retraction in adduction.19 The medial rectus muscle can be recessed 5.5 to 6.5 mm and the lateral rectus muscle can be recessed 7 to 8 mm, with some adjustment for any primary position heterotropia.20
Y-Splitting Procedure
Co-contraction of the medial and lateral rectus muscles on attempted adduction can cause a striking upshoot or downshoot of the eye. This effect is attributed to sideslip of a tight lateral rectus muscle over the globe (mechanical factors) in most cases. The Y-splitting procedure effectively results in a broad lateral rectus muscle insertion that stabilizes its position and prevents it from flipping superiorly or inferiorly over the globe, thus eliminating or greatly reducing the upshoot or downshoot of the affected eye in attempted adduction.21 The Y-splitting procedure may be combined with a moderate recession if there is associated primary position exotropia.
Step 1. The lateral rectus muscle is isolated through either a limbal (Fig. 1) or fornix incision. The muscle is dissected free of intermuscular septum and check ligaments for a distance of approximately 15 mm posterior to its insertion. When a fornix approach is used, the procedure can be performed through a single inferior temporal incision; however, making a second superior temporal fornix incision facilitates reattachment of the superior arm of the muscle.
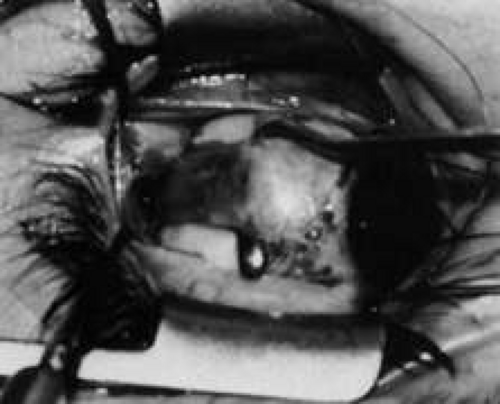
Fig. 1. The lateral rectus muscle is isolated through a limbal incision and dissected free of intermuscular septum and check ligaments for a distance of approximately 15 mm posterior to its insertion.
Step 2. A Stevens hook is brought from beneath the muscle to perforate it at its midpoint. Then, the hook is used to split the muscle into equal halves for a distance of 15 mm posterior to its insertion (Fig. 2). Blunt Westcott scissors may be used to complete the ends of the split, particularly at the muscle insertion (Fig. 3).
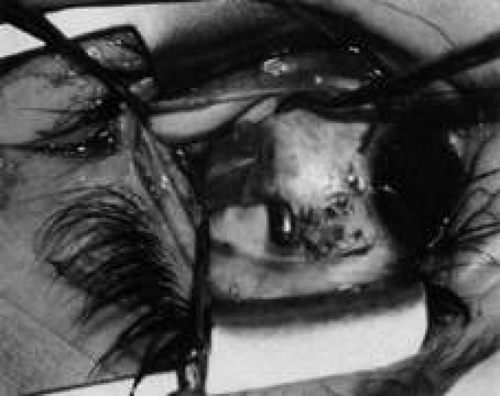
Fig. 2. A Stevens hook is brought from beneath the muscle to perforate it at its midpoint. Then, the hook is used to split the muscle into equal halves for a distance of 15 mm posterior to its insertion.

Fig. 3. Blunt Westcott scissors may be used to complete the ends of the split, particularly at the muscle insertion.
Step 3. Two double-armed 6-0 Vicryl sutures are used to secure each half of the muscle separately (Fig. 4). Both halves of the muscle are disinserted from the sclera (Fig. 5).

Fig. 4. Two double-armed 6-0 Vicryl sutures are used to secure each half of the muscle separately.

Fig. 5. Both halves of the muscle are disinserted from the sclera.
Step 4. The two halves of the muscle are separated into a Y configuration and reattached to the sclera as shown in Figure 6A. The inferior edge of the upper arm of the Y should be attached at the superior border of the original muscle insertion, and the superior edge of the inferior half of the muscle should be attached at the inferior border of the previous muscle insertion. If a recession is combined with the Y-splitting procedure, then these insertion points are relocated the desired amount posterior to the superior and inferior poles of the original insertion (Fig. 6B).
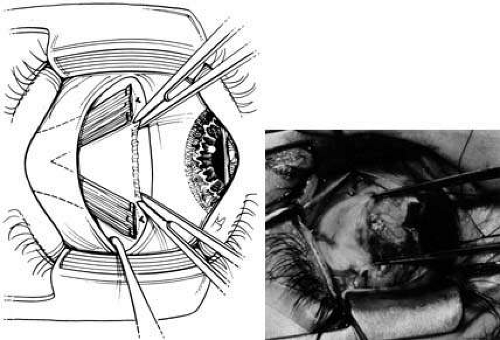
Fig. 6. The two halves of the muscle are separated into a Y configuration and reattached to the sclera. A. The inferior edge of the upper arm of the Y should be attached at the superior border of the original muscle insertion, and the superior edge of the inferior half of the muscle should be attached at the inferior border of the previous muscle insertion. B. If a recession is combined with the Y-splitting procedure, then these insertion points are relocated the desired amount posterior to the superior and inferior poles of the original insertion.
Lateral Rectus Muscle Posterior Fixation Suture
A posterior fixation suture on the lateral rectus muscle can effectively prevent slippage of the muscle belly over the globe. It may be used as an alternative procedure to treat upshoots and downshoots.22 As with the Y-splitting procedure, a posterior fixation suture can be combined with a lateral rectus recession when appropriate.
Vertical Rectus and Inferior Oblique Muscle Weakening Procedures
Besides the mechanical factors discussed, innervational factors, presumably aberrant co-contraction of the vertical rectus or inferior oblique muscles, may contribute to an upshoot or downshoot in some patients with Duane’s syndrome.23 When there is a significant vertical deviation in primary position, horizontal rectus muscle surgery alone generally does not correct the problem adequately, and recession of the appropriate vertical rectus muscle is needed.1,24 The upshoot in adduction that is often seen in Duane’s syndrome bears some resemblance to inferior oblique overaction, but inferior oblique weakening procedures usually are ineffectual in correcting the problem.21,23,25
EXPECTED RESULTS
Horizontal muscle recession reportedly eliminates the face turn in 79% of cases and significantly reduces the face turn in most of the remaining cases.4,26 In a patient with esotropic Duane’s syndrome, recession of the ipsilateral medial rectus muscle usually provides a modest improvement in abduction; however, this improvement often comes at the expense of reduction of adduction. The field of single binocular vision is shifted to include primary position but remains relatively unchanged in size. Vertical rectus transposition procedures may provide better abduction and a larger field of single binocular vision, but no studies have directly compared the efficacy of transposition with unilateral or bilateral medial rectus recession.
When they are due to mechanical factors, upshoots and downshoots usually can be satisfactorily reduced or eliminated by the Y-splitting procedure, posterior fixation, or large recessions of both ipsilateral horizontal rectus muscles. On the other hand, when the upshoot or downshoot results from innervational factors, an appropriate recession of a vertical rectus muscle eliminates the vertical deviation in primary position, but some vertical deviation usually remains when the eye is adducted. Large recessions of both horizontal rectus muscles usually provide satisfactory correction of enophthalmos in primary position, but generally, some retraction in adduction remains.
COMPLICATIONS AND THEIR MANAGEMENT
Undercorrection of primary position esotropia and the face turn probably is the most common adverse outcome after surgical treatment of Duane’s syndrome, especially when surgeons use amounts of recession typical of their experience in treating concomitant esotropia. Undercorrection may be obvious in the immediate postoperative period, or the face turn may reappear over a period of years after what initially appeared to be a good result. Late recurrence of the face turn usually results from the development of contracture of the ipsilateral medial rectus. Undercorrection can be managed by re-recession of the medial rectus muscle, if the initial recession was relatively small (less than 8 mm),27 or by vertical rectus transposition. Re-recession of the medial rectus is necessary if passive duction testing still indicates restriction.
With the large recessions necessary for treatment of Duane’s syndrome, overcorrection occurs occasionally.28,29,30 Management of this secondary exotropia is often problematic and usually requires both advancement of the recessed medial rectus muscle and recession of the lateral rectus muscle, which is often found to be restricted on passive duction testing.
New vertical deviations may result from vertical rectus muscle transposition procedures. This condition is managed by dissection, which involves considerable scar tissue, and recession of the appropriate transposed vertical rectus muscle in the ipsilateral eye, particularly if vertical passive ductions are positive, or recession of the appropriate vertical rectus muscle in the contralateral eye.
BROWN’S SYNDROME
True Brown’s syndrome is a stable, persistent limitation of eye elevation in adduction. It is caused by a congenitally shortened and therefore tight superior oblique muscle or tendon.31,32,33 In most cases, elevation in abduction is near normal, differentiating Brown’s syndrome from monocular elevation deficiency (double elevator palsy). However, when the affected eye moves from abduction to adduction, there may be a characteristic depression or downshoot. In addition, in severe cases, the limitation may extend to primary position, resulting in a hypotropia of the affected eye in primary gaze. Some patients also may have increased amounts of abduction of the affected eye on attempted elevation in primary position, resulting in a Y pattern exotropia in upgaze.
True Brown’s syndrome must be distinguished from other simulating conditions, such as inferior oblique palsy, monocular elevation deficiency (double elevator palsy), paratrochlear trauma or inflammation with resulting scarring and fibrosis, congenital periocular fibrous bands, orbital floor fracture with entrapment of orbital contents, inferior rectus fibrosis syndrome, mass effect from a glaucoma Seton implant,34,35 and inferotemporal or posterior superonasal orbital fibrosis secondary to the fat adherence syndrome that is associated with rupture of Tenon’s capsule and prolapse of fat during inferior oblique surgery. Exclusion of these simulating conditions (pseudo-Brown’s syndrome) is important because most require a different management approach. The diagnosis of true Brown’s syndrome requires: (a) the presence of typical clinical features described in the preceding; (b) the presence of mechanical restriction to elevation of the eye in adduction as demonstrated by forced duction testing either before or during surgery; and (c) complete resolution of all restriction after transection of the superior oblique tendon. Any patient with suspected Brown’s syndrome who does not meet all three criteria should be evaluated thoroughly for alternative etiologies.
INDICATIONS
In true Brown’s syndrome, surgical therapy is indicated for patients with abnormal head posture, a hyperdeviation in primary position, or diplopia. Most patients with Brown’s syndrome have fusional ability; so abnormal head posture is the most common indication for surgery. The patient may have a chin-up posture to eliminate hypodeviation in primary position or a face turn away from the affected eye, which cannot adduct without depressing. The chronic head posturing can result in musculoskeletal problems, difficulty with balance (especially in young children), and cosmetic disfigurement. Diplopia is an uncommon complaint in children who generally suppress the non-fixating eye when a deviation is present, but it can be a problem in previously well-compensated adults who later decompensate when driving or when they become tired. Occasionally, adults with Brown’s syndrome complain of vague ocular discomfort characterized as a pulling sensation or a sensation of ocular fatigue. However, by themselves, these symptoms rarely are severe enough to indicate a need for surgery. In addition, surgical correction sometimes should be considered for occupational reasons in patients whose occupations (e.g., librarian, airline pilot, painter, or professional basketball player) have significant upgaze requirements.
Although immediate surgery is not necessary, children with mild to moderate involvement without compensatory head posturing or vertical strabismus in primary position need close observation and careful follow-up for later development of the preceding surgical indications. Particular attention should be given to documentation of the visual acuity in each eye, the fusional and binocular status, and the presence of even mild or intermittent degrees of head posturing. Evidence of loss of binocularity, development of amblyopia, or loss of head posture suggests decompensation with the development of suppression and a need for immediate surgical correction.
CONTRAINDICATIONS
Many patients with Brown’s syndrome have none of the preceding indications and do not require surgery. They may have only minimal symptoms or symptoms that are present only in extreme upgaze without head posture, or they may report only unusual disconjugate eye movements in upgaze. Children spend much of their time in upgaze looking at taller adults, which accentuates even mild to moderate head posturing or disconjugate eye movements. The marked secondary over-elevation of the unaffected eye during upgaze may be the feature most readily observed by parents, leading them to suspect an abnormality of the contralateral normal eye. As a small child grows, the need for upgaze decreases, and this sign becomes less noticeable.
True Brown’s syndrome is congenital; therefore, patients with unusual features such as acute or acquired onset, the presence of pain or active inflammation around the trochlea, or signs of any of the simulating conditions listed in the preceding, require further evaluation before surgery is considered. Some forms of acquired Brown’s syndrome, such as those with associated pain, other signs of inflammation, or intermittency, respond to local corticosteroid injection. Other forms may be an early manifestation of orbital tumors or localized subperiosteal abscesses, and radiologic or sonographic imaging is needed for proper diagnosis and treatment. In patients with acute traumatic Brown’s syndrome, which may occur after blunt orbital trauma or in canine tooth syndrome, surgery should be deferred for at least 4 to 6 months to determine whether spontaneous recovery occurs.
PROCEDURES
Superior Oblique Forced Duction Testing
When any surgical procedure for suspected Brown’s syndrome is performed, superior oblique forced duction testing is required both preoperatively and intraoperatively to confirm the diagnosis of true Brown’s syndrome and assess the adequacy of the surgical treatment. A simple forced duction test is useful before surgery to confirm the diagnosis. The globe is grasped with a toothed forceps at the limbus in the inferotemporal quadrant. Taking care to maintain the globe in its proper anterior-posterior position, the surgeon attempts to adduct and elevate the eye into the superonasal quadrant. Tightness of the abnormally short superior oblique muscle–tendon complex is easily appreciated as the cause of the elevation limitation. Further confirmation of the diagnosis is accomplished by demonstrating relatively free range of motion into the superior temporal, inferior temporal, and inferior nasal quadrants. A more sensitive technique, described by Guyton,36 is the exaggerated forced duction test. With this technique, the globe is grasped near the limbus with a pair of forceps, at 3 and 9 o’clock, and then maximally retro pulsed, extorted, elevated, and adducted to place the superior oblique tendon on maximum stretch. Its tension then can be felt by rocking the temporal forceps from inferior nasally to superior temporally. As this maneuver is performed, the hand holding the temporal forceps feels a tightening and loosening force as the superior oblique tendon flips over the surface of the globe. With practice, the degree of tightness of the superior oblique tendon can be graded from normal to markedly increased, as in severe Brown’s syndrome. The exaggerated superior oblique forced duction test is valuable immediately after every superior oblique tenotomy or other lengthening procedure to verify that the entire tendon has been isolated and cut. The presence of any residual flip requires a thorough search for residual uncut tendon fibers. Alternatively, this residual action may indicate the presence of posterior fibrous bands that restrict the globe and must be sought and transected. It is likely that many cases of unsuccessful surgery to correct Brown’s syndrome are related to incomplete transsection of all superior oblique tendon fibers, particularly the most posterior ones that can be especially difficult to isolate. The exaggerated superior oblique forced duction test should be performed immediately after tenotomy to prevent this problem.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


