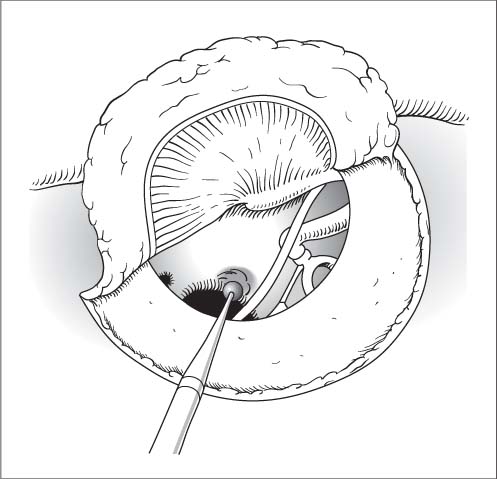
20 Surgery of the Middle Ear and Facial Nerve after Trauma Tympanoplastic principles are followed (see Chapter 18, p. 367ff). The possibility of dural or cerebral prolapse through fractures in the roof of the ear canal or tegmen should always be considered. A fistula in the round or oval window is exposed and covered with connective tissue via tympanoscopy. Acute, usually fluctuating hearing loss, often with vertigo and tinnitus after trauma or a massive rise of intracranial pressure (e. g., exertion during heavy lifting). Incision. Endaural as in stapes surgery (Chapter 21, p. 399). Window exposure. The posterolateral attic wall is taken down with a House curette until the pyramidal process can be seen. The bony overhang over the hypotympanum is also taken down slightly. The overhanging upper border usually prevents a direct view of the round window itself and can be carefully burred down (Fig. 20.1). Window inspection. Using high magnification, the surgeon looks for a tear in the annular ligament, a footplate fracture, or a window rupture. The stapes is gently rocked with a needle (alternating pressure test) to check for perilymph leakage from the round or oval window niche. Fistula repair. A perilymphatic fistula is covered with connective tissue. A ruptured round window is closed by placing fibrin-coated connective tissue into the niche. Fig. 20.1 Window rupture. The overhang over the round window is removed with a burr. Fracture lines are exposed by performing a mastoidectomy and, if necessary, opening the tympanic spaces. The fracture is traced to the dural tear, which is identified and closed with fascia, perichondrium, or fibrin-coated collagen fleece. Same as for a mastoidectomy (Chapter 19, p. 387). High-resolution CT. General anesthesia. Exposure.
Middle Ear Trauma
Injuries of the Tympanic Membrane and Ossicular Chain
Rupture of the Round or Oval Window
Surgical Principle
Indications
Specific Points Regarding Informed Consent
 See Stapedectomy in Chapter 21 (p. 399).
See Stapedectomy in Chapter 21 (p. 399).
 Emphasize the uncertain prognosis for residual hearing and vertigo.
Emphasize the uncertain prognosis for residual hearing and vertigo.
Surgical Technique
 Rules, Tips, and Tricks
Rules, Tips, and Tricks
 Slight dislocations of the footplate should be carefully reduced and connective tissue packed around the footplate. Massive dislocations or displaced footplate fractures are an indication for stapedectomy.
Slight dislocations of the footplate should be carefully reduced and connective tissue packed around the footplate. Massive dislocations or displaced footplate fractures are an indication for stapedectomy.
 The round window is often veiled by delicate mucous membranes that prevent the direct visualization of a rupture. Leakage of perilymph in response to the alternating pressure test confirms a window rupture.
The round window is often veiled by delicate mucous membranes that prevent the direct visualization of a rupture. Leakage of perilymph in response to the alternating pressure test confirms a window rupture.
Postoperative Care
 Stennert infusion protocol (starting with 1 g hydrocortisone).
Stennert infusion protocol (starting with 1 g hydrocortisone).
 Avoid straining or other acts that could raise the intracranial pressure.
Avoid straining or other acts that could raise the intracranial pressure.
Otorrhea of Cerebrospinal Fluid
Surgical Principle
Indications
 Persistent (approx. 8 days) CSF leak following trauma or surgery.
Persistent (approx. 8 days) CSF leak following trauma or surgery.
 Traumatic CSF leak in a patient with pre-existing chronic otitis media (immediate action required).
Traumatic CSF leak in a patient with pre-existing chronic otitis media (immediate action required).
 Spontaneous CSF leak in chronic otitis media.
Spontaneous CSF leak in chronic otitis media.
Contraindications
 Grave prognosis due to intracranial trauma or multiple injuries.
Grave prognosis due to intracranial trauma or multiple injuries.
 Spontaneous closure.
Spontaneous closure.
Specific Points Regarding Informed Consent
 Persistent CSF leak. Emphasize the possible need for reoperation or extending to a transtemporal or translabyrinthine approach (deafness, vertigo).
Persistent CSF leak. Emphasize the possible need for reoperation or extending to a transtemporal or translabyrinthine approach (deafness, vertigo).
 Increased risk of meningitis and brain abscess.
Increased risk of meningitis and brain abscess.
 Sinus hemorrhage.
Sinus hemorrhage.
Operative Planning
Anesthesia
Surgical Technique
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


