Incisions
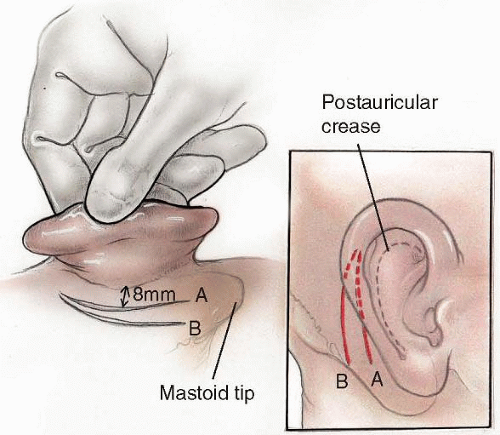
The two principal incisions used for access to the mastoid cortex are the postauricular incision of Wilde and the endaural incision of Lempert. The postauricular incision provides better overall exposure and allows complete access to the mastoid tip. In adults, the incision is placed 8 to 10 mm posterior to the postauricular sulcus, where it is hidden by the pinna (
Fig. 152.1). This incision can be placed more posteriorly for wider exposure as might be necessary during translabyrinthine access to the cerebellopontine angle. It should not be placed directly in the postauricular crease, however, because such placement creates a deep, difficult-to-clean postauricular furrow. In children younger than 2 years, the inferior portion of this incision must be placed more posteriorly than in adults (
Fig. 152.1). This is because the tympanic ring in children is underdeveloped, mastoid pneumatization is incomplete, and the stylomastoid foramen is shallow. Therefore, the facial nerve is vulnerable to injury. The surgeon should also keep in mind that congenital anomalies of the temporal bone can result in highly variable facial nerve position.
The postauricular incision is first outlined with a marking pen and infiltrated with a mixture of local anesthetic and epinephrine. The skin and subcutaneous tissues are incised sharply down to the temporalis fascia (superior to the inferior temporal line) and down to the periosteum overlying the mastoid cortex (inferior to the inferior temporal line). The ear flap is elevated anteriorly to identify the posterior edge of the external ear canal. Additional
elevation superior to the ear canal exposes the root of the zygoma. Posterior to the ear canal, the postauricular muscle and pericranial soft tissues are incised and elevated in the same plane as described above. This dissection is carried to the mastoid tip. Care must be taken not to dissect anterior to the tip because this endangers the facial nerve in the stylomastoid foramen. Unless the mastoid tip is to be removed, the sternocleidomastoid muscle’s insertion onto the tip should not be severed. This minimizes postoperative discomfort. Thus far, the skin and soft tissues of the pinna have been laid anteriorly, but the periosteum still remains attached to the mastoid cortex.
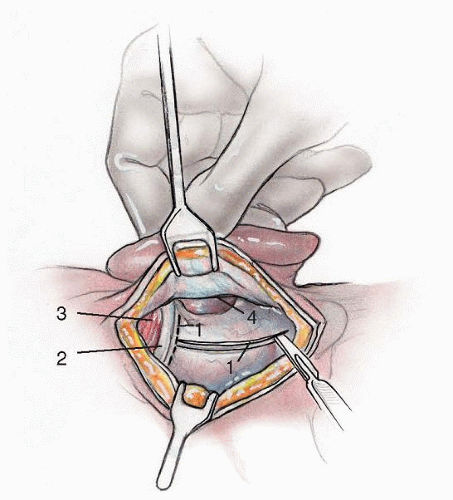
The mastoid cortex is now exposed to start the drilling process (
Fig. 152.2). A T-shaped incision is made through the soft tissues and periosteum overlying bone. The superior limb of the “T” is placed along the inferior temporal line (inferior margin of the temporalis muscle) starting at a point just superior to the anterior-superior ear canal. This incision extends posteriorly as far as is needed for adequate exposure. An inferior limb to the “T” is fashioned from the mastoid tip to the superior limb just described. Periosteal elevators are then used to elevate the periosteum of the mastoid cortex toward the posterior margin of the ear canal (
Fig. 152.2). Superior to the ear canal, the periosteum should be elevated anteriorly along the zygomatic root. Inferior to the ear canal, the surgeon should elevate the periosteum to the anterior margin of the superior aspect of the mastoid tip. If the tip is to be removed, the surgeon must remove all the periosteum from its surface. Taking a few moments to get this anterior extension, superiorly and inferiorly, will allow the ear to be held forward easily with self-retaining retractors. The periosteum can also be elevated somewhat down the ear canal to release tension and prevent a canal laceration.
Self-retaining retractors should now be placed to hold the auricle forward. The suprameatal spine of Henle marks the lateral extent of the posterior-superior bony ear canal.
The surgeon has raised two anteriorly based flaps: (a) the pinna and subcutaneous tissues and (b) the deeper musculoperiosteal tissues. This deeper flap can be used to partially obliterate the mastoidectomy cavity at the end of a canal-wall-down mastoidectomy. After an intact-canal-wall mastoidectomy, however, both layers should be closed to maintain a patent meatus and a properly positioned auricle.
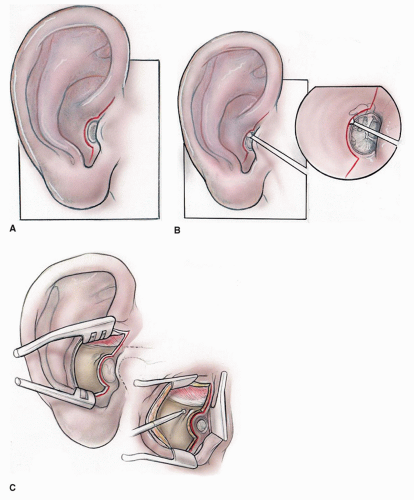
Endaural incisions were first described by Kessel in 1885 and later popularized by Lempert (
1) in 1938. These incisions expose a limited portion of the mastoid cortex. First, a posterior canal wall incision is made from the 12-o’clock to the 6-o’clock position just medial to the bony cartilaginous junction (Lempert I incision). From the 12-o’clock position of the Lempert I incision, a medial-tolateral incision is made into the incisura between the tragus and root of the helix (Lempert II incision). A relaxing incision is then made at the inferior margin of the Lempert I incision (in a medial-to-lateral direction) (
Fig. 152.3A). This allows the posterior ear canal and conchal skin to be mobilized (
Fig. 152.3A and B). Skin, soft tissues, muscle, and periosteum over the mastoid cortex are elevated using
Lempert elevators, and a self-retaining retractor is placed. Indications for this incision include simple mastoidectomy in very poorly pneumatized temporal bones, atticotomies, canaloplasties, and some tympanoplasties. The endaural incision is closed in a layered fashion approximating deep tissues and then skin.
Surface Landmarks
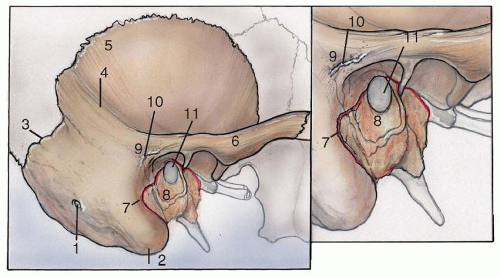
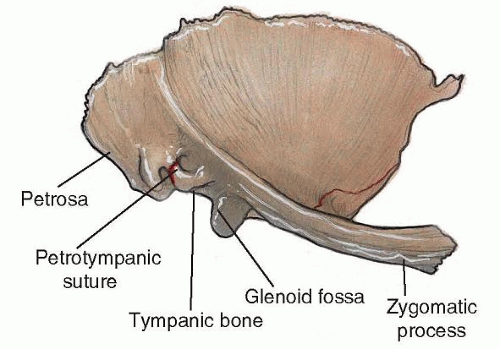
The inferior temporal line (linea temporalis) defines the inferior limit of the temporalis muscle and provides a topographic landmark for the approximate level of the floor of the middle cranial fossa. Inferior to the temporal line is a protuberance at the posterosuperior margin of the ear canal called the suprameatal spine of Henle. Macewen triangle (cribrose area) is a depressed pit just posterior to the spine of Henle and serves as a topographic landmark for the underlying mastoid antrum. The antrum is typically located 15 mm medial to the cribrose area. The zygomatic root is palpable anterior-superior to the ear canal. The anterior, inferior, and posterior-inferior walls of the external auditory canal are formed by the tympanic bone while the region between the tympanosquamous and tympanomastoid suture lines (i.e., the posterior-superior bony ear canal) is made of squamous bone (
Fig. 152.4). The canal skin in this region is thicker and more vascular than the inferior canal skin. When creating a laterally based conchal flap, this thickened “vascular strip” is elevated and preserved. The surface anatomy of the adult and young child’s temporal bone differs (
Fig. 152.5). Children younger than 2 years have immature tympanic rings and poorly developed mastoids. In children or adults with canal atresia, mal-development of the tympanic bone may result in facial nerve exit directly from the mastoid cortex (
2).
Types of Mastoidectomy
The ear canal is made up of a cylinder of skin contained within a bony cylinder. In the normal ear, the tympanic membrane is the medial boundary for both those cylinders. During routine office examination, it is not possible to see the epitympanum or mastoid region when the canal wall is intact. This is because the scutum blocks the epitympanum from view, and the posterior canal wall blocks access to the mastoid cavity. Therefore, removing the superior and posterior aspects of the bony canal allows direct access to the epitympanum and mastoid. This has the advantage of more thorough postoperative examination of the ear in the office; however, it leaves patients with cavities that require lifelong maintenance.
Mastoidectomy procedures can be categorized as canalwall-up and canal-wall-down operations. Canal-wall-up procedures include the so-called simple mastoidectomy and the complete mastoidectomy with and without a facial recess approach. Canal-wall-down operations include the radical mastoidectomy, the modified radical mastoidectomy (MRM), and the Bondy MRM. A radical mastoidectomy removes the posterior and superior bony ear canal as well as the tympanic membrane, malleus, and incus. The stapes is usually preserved. The eustachian tube is obstructed, and no middle ear space remains. The entire cavity becomes lined with squamous epithelium. The radical mastoidectomy is “modified” when the tympanic membrane is reconstructed and mucosa-lined middle ear space is created. Ossicular reconstruction can also be performed during a MRM. The Bondy MRM is performed when disease spares the middle ear and only involves the epitympanum and mastoid. The scutum and posterior bony ear canal are removed to exteriorize the antrum and epitympanum, but the middle ear is not entered. Tympanoplasty and ossicular reconstruction can be performed whether the canal wall is taken down or left intact.
Complete Mastoidectomy
The complete mastoidectomy affords access to the antrum, attic, labyrinth, endolymphatic sac, and vertical segment of the facial nerve. All the air cells along the tegmen, sigmoid sinus, facial nerve, and semicircular canals are usually removed. The epitympanum is made accessible through the aditus ad antrum, and the incus and head of the malleus can be inspected directly. The incus and the head of the malleus may be removed for greater access to the supratubal recess in the anterior part of the attic.
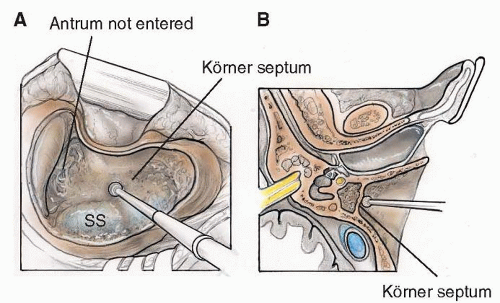
Using the postauricular incision, the ear is laid forward and the mastoid cortex exposed as described above. The temporal line, spine of Henle, cribrose area, and posterior bony ear canal are used as the initial landmarks for drilling. The location of the mastoid antrum can be approximated by the intersection of a horizontal and vertical line drawn tangential to the superior and posterior margins of the bony external auditory canal. A large cutting burr and continuous suction/irrigation are used to begin the mastoidectomy. Cortical bone is removed inferior to the middle fossa dura (tegmen mastoideum), the posterior edge of the bony ear canal is delineated, and the sigmoid sinus is identified. It is useful to widely saucerize the mastoidectomy bowl by removing any overhanging edges. This permits more light to enter the cavity and allows the surgeon to bring in his or her instruments into the operative field at an angle rather than directly along his or her line of sight. After determining the level of the tegmen, air cells lateral to the sigmoid sinus should be removed to see the blue hue of the sinus through thin bone. The sinodural angle, marking the posterior-superior limit of the mastoid cavity, is then opened. Drilling proceeds medially along the tegmen toward the epitympanum. Keeping this anterior-superior portion of the dissection as the deepest portion of the cavity avoids inadvertent injury to the facial nerve. Körner septum is a plate of bone lateral to the antrum, and it represents the posterior extension of the petrosquamous suture line within the mastoid (
3) (
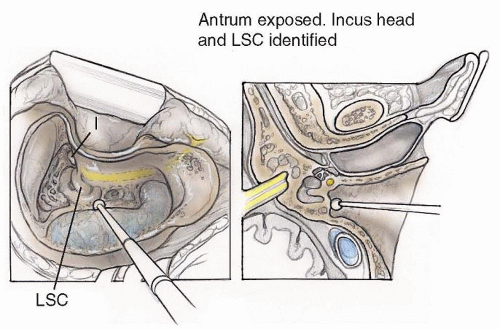
Fig. 152.7). The superior aspect of Körner septum must be removed to enter the mastoid antrum. The floor of the antrum, which is the lateral semicircular canal, is a vital landmark that must be clearly visualized (
Fig. 152.8). Otic capsule bone of the labyrinth usually appears to be a slightly lighter hue when compared with the surrounding membranous bone.
Once the antrum is entered, the bone of the posterior ear canal wall must be thinned, although excessive thinning may lead to delayed dissolution of this structure. Identifying the posterior incudal ligament (often seen as a white streak through thin bone just inferior to the fossa incudus) is a useful landmark in finding the incus. By flooding the antrum with clear irrigant, the surface of the fluid forms a lens that will bend light from the microscope and allow the surgeon to see the incus before actually coming upon it (
Fig. 152.8). Touching the incus with a rotating burr must be avoided because transmission of
high-frequency mechanical energy to the inner ear can cause sensorineural hearing loss. Once the incus body is identified, removing the bone lateral to the ossicles (between the tegmen tympani and bone of the superior ear canal) opens the epitympanum. Carrying this dissection anteriorly will expose the head of the malleus.
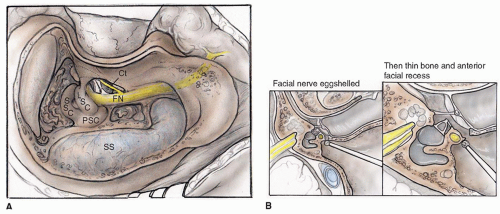
Having found the antrum, the horizontal semicircular canal, and the incus, attention can now be directed to identifying the facial nerve. Bony trabeculae on the bony external auditory canal are removed from a lateral to medial direction. As this dissection proceeds medially, facial recess air cells anterior to the facial nerve will be encountered. The second genu of the facial nerve is located immediately anterior and inferior to the midpoint of the horizontal canal, just medial to the short process of the incus. Here, a 4-mm diamond burr and copious irrigation are used to make wide strokes, starting at the incus superiorly and aimed toward the stylomastoid foramen inferiorly. Adequate irrigation prevents thermal injury to the nerve. The facial nerve should be visualized through thin bone but not completely exposed. As the facial nerve is traced inferiorly, the branch-point of the chorda tympani nerve will be found (
Fig. 152.9A). The chorda can then be traced anteriorly and superiorly.
All of the cells within the mastoid tip may be exenterated. The posterior belly of the digastric muscle inserts medially on the mastoid tip. Identifying the muscle through eggshelled bone is referred to as the “digastric ridge,” which is actually a surgically created landmark (
Fig. 152.9A). Fascia enveloping the digastric muscle is continuous with the fibrous tissue surrounding the facial nerve at the stylomastoid foramen. The stylomastoid foramen enlarges as it exits the inferior portion of the temporal bone. Following the digastric ridge anteriorly in the mastoid tip is one technique used to find the facial nerve. Infralabyrinthine (retrofacial) air cells are those cells medial to the facial nerve, superior to the jugular bulb, and inferior to the posterior semicircular canal. They should be exenterated if disease is found within them or if either the jugular bulb or endolymphatic sac needs to be exposed.
Following a complete mastoidectomy, the surgeon should thoroughly irrigate the cavity to remove bone dust, which may otherwise cause ossicular fixation. The complete mastoidectomy cavity should consist of a well-defined tegmen tympani and tegmen mastoideum superiorly, a clearly delineated sigmoid sinus posteriorly, an open sinodural angle, well-visualized semicircular canals, an intact posterior bony ear canal wall, and the facial nerve seen through thin bone.
Complete Mastoidectomy with a Facial Recess Approach
The facial recess is an aerated extension of the posterior-superior middle ear space. Medial to the tympanic annulus and lateral to the fallopian canal, it allows access to the middle ear from the mastoid cavity without disruption of the tympanic membrane. Some surgeons use the term “posterior tympanotomy” to describe a facial recess approach. The facial recess is a triangular opening bordered posteromedially by the facial nerve, anterolaterally by the chorda tympani nerve, and superiorly by the fossa incudis (
Fig. 152.9). An open facial recess provides access to the ossicles, stapedius tendon, round window, tympanic segment of the facial canal, and cochleariform process (
4). Dissection of the region of the facial recess should be performed with diamond burs and copious suction irrigation to avoid mechanical or thermal damage to the nerves.
There are numerous indications for performing a posterior tympanotomy. These include transmastoid cochlear implantation, middle ear electromechanical implantation (
5), presence of cholesteatoma within both the middle ear and mastoid, chronic otomastoiditis with granulation tissue or cholesterol granuloma, and tumors within the middle ear and mastoid (
6).
In the anterior epitympanum, a projection of bone extending inferiorly from the tegmen tympani (the cog) can obscure disease in the supratubal recess (
7). The presence of granulation tissue, cholesteatoma, or tumor in the anterior epitympanum and supratubal recess may require removal of the incus, head of the malleus, and the cog for increased exposure. If removal of the incus is necessary, the incudostapedial joint must first be disarticulated through the facial recess before removing the incus and malleus head. Opening the facial recess can also improve aeration of the mastoid by providing an alternate route for air from the eustachian tube to enter the mastoid (other than the aditus ad antrum). Inadequate aeration or loculation of the mastoid cavity may result in recurrent retraction pocket formation, mucocele formation, or chronic otomastoiditis. One way to test for adequate aeration of the mastoid cavity is to fill the middle ear with saline and watch for flow into the mastoid. When the incus has been removed, rarely is a facial recess approach required for aeration. When thinning the posterior bony canal wall, the facial recess is encountered medially. It is first noted as a color change (darker appearing bone) anterior to the facial nerve, just inferior to its second genu. The facial nerve lies medial and inferior to the tip of the short process of the incus. The second genu of the facial nerve usually forms an angle of 95 to 125 degrees; it usually makes a gentle curve rather than an abrupt turn. The nerve may descend directly through the mastoid in a caudal direction, or it may deviate from the vertical by 5 to 35 degrees. The facial nerve travels laterally as it moves inferiorly through its vertical segment and is located lateral to the posterior-inferior tympanic annulus in 65% of cases (
8).
The surgeon should be aware of potential facial nerve anomalies. Dehiscence of the facial nerve is reported to occur in 55% to 57% of temporal bones (
9). The facial nerve is dehiscent approximately 50% of the time just superior to the oval window, in its tympanic segment. Other areas of possible dehiscence include the geniculate ganglion, facial recess, tympanic sinus, and the retrofacial region. Bone erosion secondary to cholesteatoma may also create dehiscence in the fallopian canal. Before encountering the nerve, the vasa nervorum can be appreciated through the eggshelled bone overlying the nerve. The most common site of injury to the facial nerve in mastoid surgery is inferior to the lateral semicircular canal just beyond the second genu (
9).
At a variable point along its descent toward the stylomastoid foramen, the facial nerve gives off the chorda tympani nerve. This nerve travels in an anterior, superior, and lateral direction. Facial nerve anomalies can include a chorda that branches from the facial nerve after it exits from the stylomastoid foramen, a bifid facial nerve (
10), or a nerve coursing through the middle ear space just inferior to the oval window (
11). Once the chorda tympani nerve is identified, the bone between the chorda and the facial nerve may be removed with a small diamond burr and copious irrigation. This opens the facial recess (
Fig. 152.9A). If additional exposure is required, an extended facial recess approach can be performed, where the chorda is sacrificed and the facial recess extended inferiorly. Care must be taken to identify the fibrous annulus of the tympanic membrane and to avoid inadvertent injury to the tympanic membrane or medial ear canal.
Intact Canal Versus Canal-Wall-Down Mastoidectomy
Both the open (canal-wall-down) and the closed (intact canal with facial recess or posterior tympanotomy) procedures have advantages and disadvantages. Judgment as to which procedure to perform depends on the nature of the disease, the reliability of the patient, and the experience of the surgeon (
Table 152.2).
The intact-canal-wall approach offers several advantages over open (canal-wall-down) techniques. First, postoperatively there is no mastoid cavity to care for. Patients
with cavities often require regular office debridement, may have a difficult time fitting hearing aids, need to adhere to water precautions, and have meatoplasties that may be cosmetically unappealing. An intact-canal procedure also allows for a more physiologic ossicular reconstruction with a deeper, better-aerated middle ear. Some authors, however, have found no significant benefit in hearing results for intact-canal-wall mastoidectomy compared with canalwall- down procedures (
12,
13).