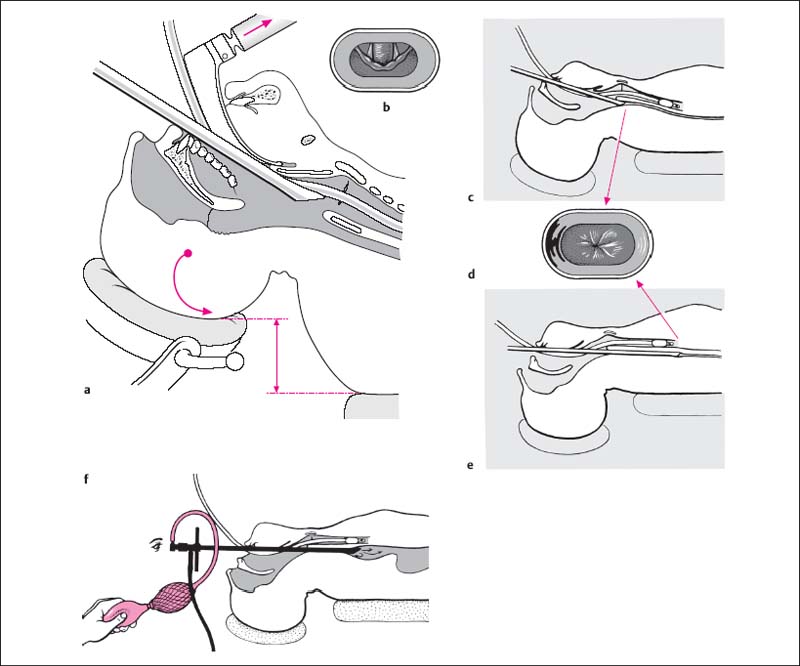
12 Surgery of the Esophagus and Mediastinum The length of the esophagus ranges from 20 to 34 cm in adults. The esophagus has three physiologic constrictions that are relevant to endoscopy. The first constriction, caused by the tone of the constrictor muscles, is located at the esophageal inlet approximately 14 cm (12–16 cm) from the upper incisor teeth. The middle constriction, formed by the aortic arch and left main bronchus, is located ca. 27 cm (22–29 cm) from the upper incisor teeth, and the lower constriction (cardia) is located at ca. 41 cm (32–50 cm). Esophagoscopy can be performed with a rigid tube or flexible esophagoscope. The indications for both methods overlap somewhat, but the choice of an endoscope will depend partly on the preference and experience of the surgeon. The rigid esophagoscope can be used both diagnostically and therapeutically and is the instrument of choice for foreign body extractions. Fiber-optic instruments, on the other hand, are better for performing diagnostic endoscopy under local anesthesia. This technique is often combined with gastroduodenoscopy. A rigid tube is introduced transorally into the esophagus for dilation, inspection, incisional biopsy, or foreign body extraction. Contrast radiography of the esophagus. Barium should be withheld if there is possible esophageal wall injury from a foreign body or risk of aspiration. Esophagoscopes of assorted lengths and diameters. Endoscopic forceps, cup forceps, suction tips, dilators, optical esophagoscope with telescopes (if needed), optical forceps, and apparatus for air insufflation. The tube length and diameter should conform to patient anatomy (height, age, sex, condition of cervical spine). General endotracheal anesthesia (relatively large endotracheal tube with minimal cuff inflation, complete muscular relaxation). Positioning. Supine with the head initially elevated for introducing the endoscope. As the endoscope is advanced, the head is lowered. Protection of the upper teeth is mandatory. Exposure of the larynx and piriform sinus. The head is slightly elevated and tipped back (as for intubation or bronchoscopy). The laryngoscope handle is drawn straight back so that the blade presses downward on the tongue, exposing the epiglottis and arytenoid processes (Fig. 12.1a, b). Saliva is removed by suction. Insertion of the esophagoscope. The esophagoscope is introduced at the right oral commissure and inserted behind the arytenoid processes, which are easily lifted forward with the instrument tip in this position. Meanwhile an assistant draws back the upper lip to protect it from pressure injury. The rigid esophagoscope is gently advanced to a site just proximal to the esophageal inlet, which appears as an oblong slit. As the tube passes behind the arytenoid cartilage, further observation is done through the endoscope and the laryngoscope blade is removed. Entering the esophagus. To advance the scope across the esophageal inlet, the patient’s head is slightly lowered until the transverse opening of the inlet is centered in the field of view. With the patient fully relaxed, the surgeon can easily advance the tube into the esophagus with just two fingers and without having to apply force. Stabilizing the tube. The left hand stabilizes the tube against the dental arch while simultaneously protecting the teeth and retracting the lips. Further insertion and inspection of the esophagus. The tube is advanced further under constant vision, and secretions are aspirated as needed. The lumen of the esophagus should always be kept at the center of the field; this is accomplished by lowering the head further and slightly elevating the tip of the tube as it advances (Fig. 12.1a–f). The tip of the scope will also tend to follow the natural curve of the esophagus toward the left side. Gastric acid reflux often occurs when the endoscope passes through the cardia. Fig. 12.1a–f Rigid esophagoscopy. a The head is elevated and tilted back for insertion of the esophago-scope. The pharynx is expanded with a laryngoscope blade. b The tip of the tube is carefully advanced behind the visible arytenoid cartilages. c When the tip of the scope has passed through the esophageal inlet, the head is lowered. d This permits the tube to remain centered on the esophageal lumen. e At deeper levels the head is lowered further and the tip of the tube is elevated slightly in the anterior direction. f With a pneumatic esophagoscope, visualization is improved by insufflating air into the esophagus. No special measures are necessary after esophagoscopy. Oral intake may have to be withheld in patients with mucosal lesions. Antibiotic coverage is generally withheld as it could mask an incipient mediastinitis. Foreign bodies most frequently become lodged at the first esophageal constriction and less commonly at the second or third constriction. Predisposing factors are esophageal strictures due to caustic ingestion or neoplasia. Exposure of the foreign body. The esophagoscope is introduced as described above, and the foreign body is visualized. The tip of the scope is brought to bear on the foreign body, which should be centered in the tube. Occasionally the foreign body is lost to view when the tube is advanced but is reacquired by withdrawing the tube slightly. Extraction of smooth-surfaced foreign bodies. Smooth-surfaced foreign bodies such as coins and buttons are grasped with an alligator forceps or other suitable instrument, pulled against the end of the tube, and carefully extracted along with the tube. The scope is then reintroduced to inspect the esophagus for injuries or additional foreign bodies. Extraction of impaled foreign bodies. Impaled foreign bodies such as needles and bone fragments must first be oriented transversely. The esophagoscope tip is initially trained on the less impaled end, which is grasped with an alligator forceps and will become the leading edge during removal. The impaled end is then visualized and carefully extracted with the tube. The interior of the esophagus is then reinspected (Fig. 12.2a–c). Foreign body extraction using special instruments. Special instruments are available for the extraction of certain foreign bodies. Straight pins can be bent to aid removal (Fig. 12.2d
Endoscopic Surgery
Anatomical Data
Rigid Esophagoscopy
Surgical Principle
Indications
 Suspected foreign body in the esophagus.
Suspected foreign body in the esophagus.
 Esophageal polyps.
Esophageal polyps.
 Dilation of strictures or webs.
Dilation of strictures or webs.
 Suspected esophageal neoplasm.
Suspected esophageal neoplasm.
 Investigation of wall changes due to caustic ingestion.
Investigation of wall changes due to caustic ingestion.
 Cardiospasm.
Cardiospasm.
 Suspected esophageal varices or for sclerotherapy (flexible esophagoscopy is generally preferred).
Suspected esophageal varices or for sclerotherapy (flexible esophagoscopy is generally preferred).
Contraindications
 Severe changes in the cervical or thoracic spine.
Severe changes in the cervical or thoracic spine.
 Severe systemic diseases that would contraindicate general anesthesia.
Severe systemic diseases that would contraindicate general anesthesia.
Specific Points Regarding Informed Consent
 Dental injury or tooth loss.
Dental injury or tooth loss.
 Dysphagia, gastric intubation.
Dysphagia, gastric intubation.
 Hoarseness or voice loss.
Hoarseness or voice loss.
 Dyspnea, which may necessitate a tracheostomy.
Dyspnea, which may necessitate a tracheostomy.
 Mucosal injury, perforation of the esophageal wall.
Mucosal injury, perforation of the esophageal wall.
 Pneumonitis with associated lung changes.
Pneumonitis with associated lung changes.
 Mediastinitis.
Mediastinitis.
 Paralysis of the lingual nerve and hypoglossal nerve.
Paralysis of the lingual nerve and hypoglossal nerve.
 Subcutaneous emphysema in the neck.
Subcutaneous emphysema in the neck.
Operative Planning
Special Instruments
Anesthesia
Surgical Technique
 Perforation of the hypopharynx or esophagus leading to mediastinitis, pleural or pericardial injuries, or peritoneal injury. Previously undetected hypopharyngeal diverticula increase the risk of perforation.
Perforation of the hypopharynx or esophagus leading to mediastinitis, pleural or pericardial injuries, or peritoneal injury. Previously undetected hypopharyngeal diverticula increase the risk of perforation.
 Dental injury or tooth loss, especially in patients with pre-existing tooth damage.
Dental injury or tooth loss, especially in patients with pre-existing tooth damage.
 Dislocation of the arytenoid cartilage.
Dislocation of the arytenoid cartilage.
Postoperative Care
 A suspected perforation should be investigated immediately by oral contrast examination with a water-soluble contrast medium (detection of extravasation) and soft lateral neck radiographs (air detection, increased prevertebral density). A suspected deeper perforation should be investigated by chest radiographs (pleural effusion) and standing abdominal radio-graphs (air crescent). Thoracic CT scans may be ordered in consultation with a radiologist. Palpation of the neck will disclose cutaneous emphysema. Watch for signs of sepsis. The detection of an esophageal perforation generally requires immediate intervention, usually aided by a thoracic surgeon.
A suspected perforation should be investigated immediately by oral contrast examination with a water-soluble contrast medium (detection of extravasation) and soft lateral neck radiographs (air detection, increased prevertebral density). A suspected deeper perforation should be investigated by chest radiographs (pleural effusion) and standing abdominal radio-graphs (air crescent). Thoracic CT scans may be ordered in consultation with a radiologist. Palpation of the neck will disclose cutaneous emphysema. Watch for signs of sepsis. The detection of an esophageal perforation generally requires immediate intervention, usually aided by a thoracic surgeon.
Foreign Body Extraction from the Esophagus
Surgical Technique
![]()
Stay updated, free articles. Join our Telegram channel
 Risks and Complications
Risks and Complications
Full access? Get Clinical Tree


