Surgery for Otosclerosis and Fixation of the Stapes
Surgery for Otosclerosis and Fixation of the Stapes
Joseph B. Nadol, Jr.
Harold F. Schuknecht
There are more than 20 genetically determined disorders that produce a conductive hearing loss that involves stapes fixation (1). In addition, there are numerous acquired disorders, including tympanosclerosis and trauma, which may result in significant conductive hearing loss due to fixation of the stapes. Nevertheless, the most common disorder causing fixation of the stapes is otosclerosis, an autosomal dominantly inherited bony dysplasia that seems to affect only the otic capsule and only in man (2). In addition to its known genetic predisposition, chronic viral infection of bone may also play a role in the pathogenesis of otosclerosis (3). Otosclerosis may cause conductive hearing loss in one or both ears in up to 1% of the Caucasian population.
HISTORICAL PERSPECTIVE
When the first attempts were made to improve hearing by surgical approaches to the oval window (4, 5, 6, 7, 8, 9), otosclerosis had not yet been recognized as a pathologic entity. These early efforts were unsuccessful because of inadequate instrumentation and the lack of adequate magnification. Then, after an exciting and moderately successful 20 years of fenestration surgery introduced by Sourdille (10) and Lempert (11), and a short-lived experience with stapes mobilization begun by Rosen (12), the era of stapedectomy began. Although Hall and Rytzner (13) had some success with stapedectomy, it was Shea’s technique (14) of substituting a vein graft and polyethylene tube for the stapes that gave the first consistently successful results.
The nomenclature of contemporary stapedectomy procedures is somewhat confusing. Thus some would call the creation of a small fenestra in the footplate a stapedotomy, whereas others would call this a partial stapedectomy. At a most fundamental level, there are three principal types of stapes procedures in contemporary usage designed to overcome conductive hearing loss (Table 22.1).
The fundamental differences in technique involve two steps of the procedure. The first is the management of the oval window and footplate and the second is the technique of interposition to reestablish continuity of the ossicular chain with the oval window. Bone removal at the oval window may include total or partial removal of the footplate. Partial removal may include fractional removal, such as removal of the posterior third or half of the footplate. In the small fenestra technique, a circular opening is made in the central footplate either with a laser or with a microdrill. Some authors have recommended sectioning of the footplate to allow partial remobilization of the posterior half. Thus Silverstein (15) has recommended a laser STAMP procedure in which ossicular chain is separated from the fixed anterior footplate by removal of the anterior crus and transverse sectioning of the footplate with a laser to allow reestablishment of mobility through the posterior crus and newly mobilized posterior segment.
Numerous prostheses have been developed to reestablish continuity between the ossicular chain and the oval window, including a variety of pistons of varying diameters and materials, combinations of prosthetic materials and tissue grafts such as the fat-wire prosthesis, and reestablishment of continuity using the posterior crus, as championed by Hough (16). In conformance with the algorithm for describing surgical procedures described in Chapter 11, we recommend the nomenclature illustrated in Table 22.2. Notice that the term stapedotomy has been deliberately avoided, because it means a small-fenestra partial stapedectomy to some authors and sectioning of the footplate without creating a fenestra to others.
TABLE 22.1Nomenclature for contemporary stapes surgery
Management of oval window and footplate
Total removal of footplate
Partial removal of footplate
Fractional removal
Small fenestra
Sectioning footplate without removal (“partial mobilization”)
Reestablishment of continuity between ossicular chain and oval window
Incus to oval window
Piston
Maintenance of posterior crus (“physiologic stapedectomy”)
Fat-wire
Malleus to oval window
Piston
Fat-wire
TABLE 22.2Algorithm and nomenclature for planning and describing stapes surgery
Elements of procedure
Incision and approach
Exposure of middle ear
Management of oval window and fixed footplate
Method for reestablishing continuity between ossicular chain and oval window
Incus to oval window
Examples
Transcanal Endaural
Anteriorly based tympanomeatal flap
Total removal of stapes footplate
Piston with tissue graft without tissue graft
Postauricular
Partial removal of footplate, posterior half, small fenestra drill-out
Fat-wire prosthesis Vein graft with preservation of posterior crus
Drill-out with small fenestra
Malleus to oval window piston or fat-wire prosthesis
On the basis of animal experiments in which several different types of tissue and prostheses were tested in cats, Schuknecht et al. (17) devised the fat-wire technique in conjunction with total stapes removal. In the search for simpler surgical techniques and for improvement in results, new methods were proposed by many surgeons. Among these were partial stapedectomy (18), vein graft and Teflon strut (19), wire loop prosthesis (20), Teflon-wire piston (21,22), Gelfoam-wire prefabricated prosthesis (23), and stainless steel piston (24,25). In 1969 Schuknecht and Applebaum (26) reported that consistent excellent hearing gains could be achieved by introducing a small diameter (0.6-mm) Teflon-wire piston through a small fenestra in the footplate. Small fenestra stapedectomy has virtually eliminated many of the complications of total stapedectomy, such as postoperative vertigo, reparative granuloma, and fibrous fixation of the lenticular process to the promontory, and is our procedure of choice for stapes fixation caused by otosclerosis and other causes.
INDICATIONS/CONTRAINDICATIONS AND INFORMED CONSENT FOR STAPEDECTOMY SURGERY
Indications
In general, there should be a conductive loss of at least 25 db in frequencies 250 to 1 kHz or higher as determined by audiometry and the presence of a negative Rinne using a 512 cps tuning fork. The presence of a concomitant sensorineural hearing loss does not necessarily contraindicate stapes surgery. Thus if a hearing aid will still be required even after successful stapedectomy, the procedure may well be worthwhile to improve auditory performance using amplification. This is particularly relevant in a patient with a profound mixed hearing loss in whom, after stapedectomy, a high gain amplifier may be beneficial. Only one ear is operated on at a time. The ear with the higher pure-tone average is generally selected. Following successful stapedectomy on one side, an interval of 8 to 12 months is generally allowed to pass to be sure the results are stable before recommending surgery in the opposite ear.
Contraindications
Elective stapedectomy on an only hearing ear is almost always contraindicated. One exception may be a case of a profound mixed loss in which a conventional hearing aid provides no auditory improvement and in which cochlear implantation would be indicated if stapedectomy does not allow the use of a conventional hearing aid. Stapedectomy is contraindicated in cases with active infection either of the middle ear or external auditory canal or in the case of perforation of the tympanic membrane. Patients with unstable medical conditions, as determined by a medical consultant, may be better advised to continue to use a hearing aid rather than undergo elective surgery. Patients in whom vestibular function is absolutely critical for their employment may be better advised to avoid stapedectomy rather than risk postoperative vestibular symptoms. In general, elective stapedectomy should not be done if the operative or nonoperative ear is unstable. Thus ipsilateral Meniere’s disease or immune-mediated sensorineural loss is a relevant contraindication to surgery. Likewise the presence of contralateral chronic active otitis media, Meniere’s disease, or immune-mediated sensorineural loss is also a relative contraindication.
Informed Consent for Stapedectomy
Insofar as possible, the surgeon should advise his patient on the broad outline of the procedure plan, as described in Table 22.2. Thus most patients will be advised that their surgery is to be done by a transcanal route, that a laser may be employed during the procedure, and that, for example, a piston prosthesis is planned. However, it is important for the patient to recognize and accept the fact that the surgical procedure may have to be modified depending on findings at the time of the procedure. The risks of surgery include failure of surgery to improve hearing by virtue of residual conductive hearing loss; creation of a sensorineural loss, either partial or complete; vestibular dysfunction; perforation of the tympanic membrane; facial nerve dysfunction (either motor or sensory); and late failure of the procedure or development of a perilymph fistula. The patient should certainly be aware of the nonoperative option of the use of a hearing aid.
The entire spectrum of stapes surgery will not be covered in this chapter. Rather, the preferred methodology as practiced at the Massachusetts Eye and Ear Infirmary will be discussed. During the course of this description, alternative methodology for the specific portion of the procedure will be included.
METHOD OF PERFORMING PRIMARY STAPEDECTOMY*
Anesthesia
The patient is offered either a local or general anesthesia. Local anesthesia certainly has the advantage of allowing monitoring of vestibular symptoms at the time of fenestration of the footplate and insertion of the prosthesis. This is of particular advantage in revision surgery, where the original prosthesis may be attached by adhesions to the contents of the vestibule. On the other hand, general anesthesia provides assurance, both to the patient and the surgeon, of absolute control of head motion and prevention of pain. In general, approximately 50% of patients will select a general anesthesia. For patients who are particularly nervous or claustrophobic or who otherwise have difficulty maintaining the surgical position, general anesthesia is preferentially recommended.
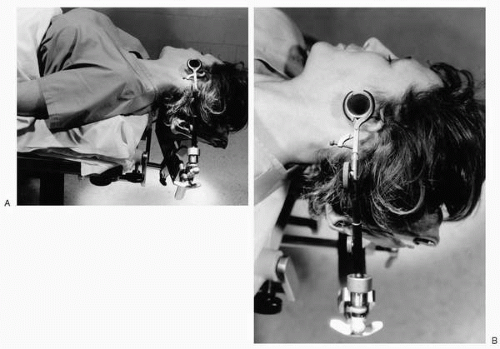
FIG. 22.1 A: The proper position for stapes surgery includes a slight head-hanging position with the chin turned to the opposite shoulder to open the angle between the ear and ipsilateral shoulder. B: A speculum holder is attached to the head rest and has sufficient degrees of freedom to allow easy adjustment of the angulation of the speculum during the procedure.
Surgical Procedure
Positioning
Proper positioning of the patient will facilitate exposure. The patient is placed in a supine head-hanging position and the head rotated slightly to the opposite shoulder to place the tympanic membrane approximately in the horizontal plane and to open the angle between the auricle and the ipsilateral shoulder (Fig. 22.1A). A headrest that is separable from the remainder of the operating table is preferred to facilitate appropriate positioning. The headrest is fitted with a fastening mechanism for a self-retaining speculum holder with sufficient degrees of freedom to allow proper positioning of the speculum and to accommodate varying degrees of head-hanging and rotation (Fig. 22.1B).
With either monitored intravenous anesthesia or general anesthesia, a local anesthetic block of the external auditory canal is performed using a combination of Xylocaine and epinephrine.
Exposure
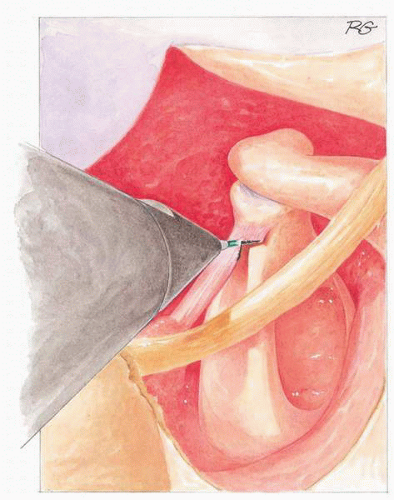
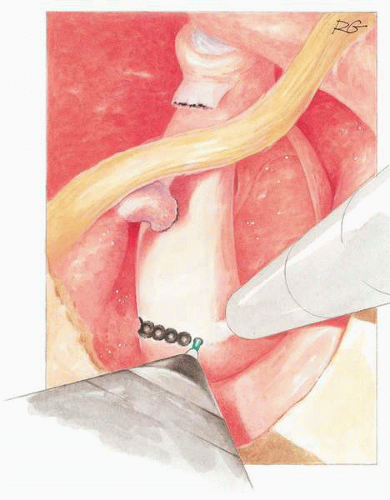
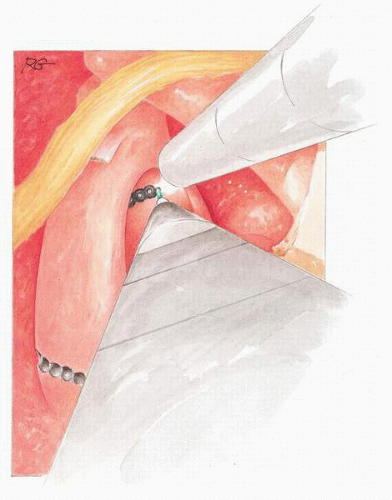
A small triangular tympanomeatal flap is elevated (Fig. 22.2) and the bony tympanic annulus is curetted to provide surgical access to the oval window (Fig. 22.3). Curettage is complete when the bony pyramidal eminence is visible posteriorly and the facial nerve is visible superiorly. At this point, the middle ear should be inspected and patency of the round window, mobility of the incus and malleus, and fixation of the stapes should be confirmed. The incudostapedial joint is separated (Fig. 22.4). Using a scissors or the argon laser, the stapedius tendon is sectioned (Fig. 22.5). A posterior crurotomy is accomplished (Fig. 22.6). If visible, an anterior crurotomy may also be done to separate the superstructure from the footplate (Fig. 22.7). The remaining superstructure is fractured toward the promontory.
Fenestration
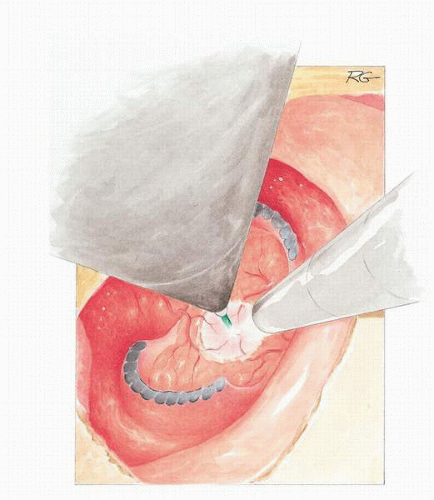
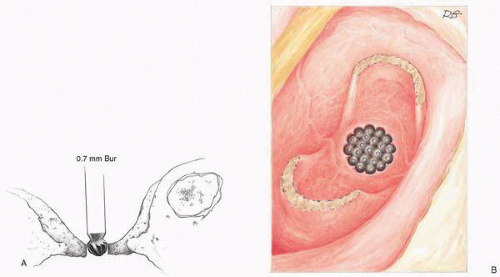
If the mucous membrane of the footplate is thin, it is not disturbed; if it is thick, it is elevated from the footplate but only in the area to be fenestrated or coagulated with a laser (Fig. 22.8). Using a motor-driven, sharp cutting bur or diamond-surfaced bur measuring 0.7 mm in diameter (Fig. 22.9A) or a laser (Fig. 22.9B), an opening is made in the thinnest part of the footplate. Lasers in the visible range (argon and KTP-532) and invisible range (CO2) are used for stapes surgery. The advantages of visible laser include the fact that the aiming and treatment beams are identical and can be delivered through a fiber-optic handheld bundle. However, visible lasers are only partially absorbed by the white bone of the stapes footplate and theoretically pass through an open vestibule and are absorbed by a pigmented tissue within the inner ear. Significant temperature elevation at the level of the saccule and utricle has been reported using the visible lasers (30). However Marquet (31), Perkins (32), DiBartolomeo (33), McGee (34), and Horn et al. (35) have all used the argon or KTP-532 lasers with success.
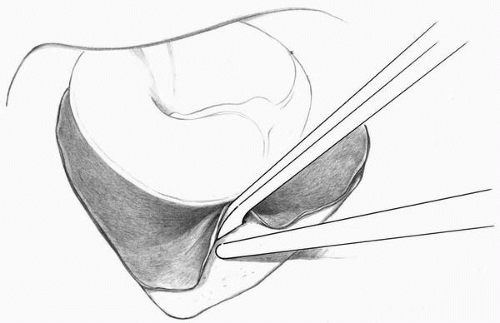
FIG. 22.2 A triangular segment of meatal skin is incised with a roller knife and is elevated to the tympanic annulus to create an anteriorly based tympanomeatal flap.
Optical delivery systems now provide the precision to allow the CO2 to be applied to middle ear surgery. The CO2 laser has the advantage of no significant penetration or caloric effect on the perilymph (36). However, it has the disadvantage of not being deliverable through a fiber-optic bundle and hence must be attached to the operating microscope with a separate coaxial aiming beam.
Clear advantages of the laser include (i) its hemostatic properties; (ii) precision that far exceeds other handheld instruments; (iii) the ability to vaporize the thicker posterior crus, therefore reducing the chance of a floating footplate; (iv) the ability to create a precise fenestra in the footplate without excessive footplate or perilymph motion, thus minimizing the risk of acoustic trauma; and (v) the ability to fenestrate a floating footplate without risk of depressing the footplate into the vestibule as is inherent in other fenestration techniques.
Because the argon laser is delivered through a fiber-optic bundle, it becomes defocused very rapidly after leaving the end of the probe. Thus the probe is withdrawn a few millimeters, the cutting action is lost, and the laser becomes an excellent coagulator of small mucosal vessels which are common in the area of the otosclerotic focus anteriorly. Using the argon laser (typical setting 1.8 watts, 0.1 second), a rosette is created in the center of the footplate (Fig. 22.9B). Because the fiber-optic bundle delivers a spot size of approximately 200 microns, a rosette 3 to 4 diameters wide should result in a circular fenestra in the footplate measuring approximately 0.7 mm, which is sufficient to accommodate a 0.6-mm diameter piston. To avoid development of heat at the footplate level, 2 to 3 seconds is allowed to pass between each laser pulse. Once the “black char” of the laser spot has been created, absorption of subsequent pulses is made easier by overlapping the laser spots, taking advantage of the fact that the visible laser is better absorbed by a dark color. The typical appearance of a single lasered spot on the footplate will be a black char measuring approximately 200 microns in diameter, a more central white char, consisting of vaporized bone, and a central “pinhole” where the perilymph has been exposed (Fig. 22.9B).
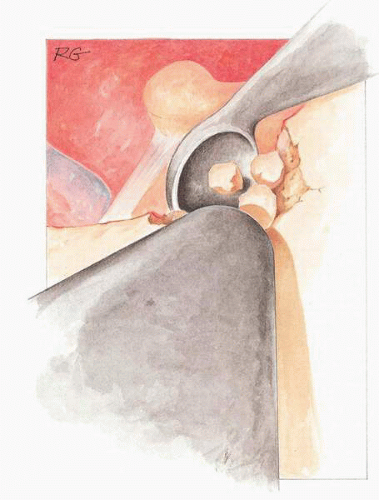
FIG. 22.3 The posterior bony annulus is curetted to allow visualization of the facial nerve superiorly, the pyramidal eminence posteriorly, and the entire circumference of the oval window.
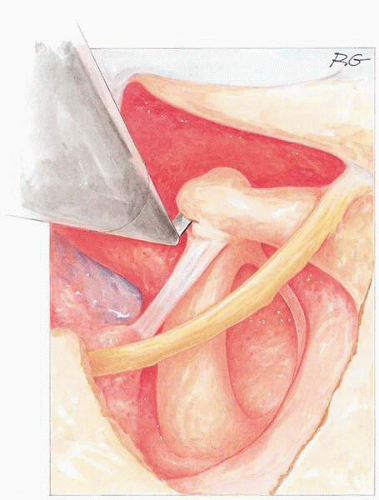
FIG. 22.4 The incudostapedial joint is separated with a joint knife.
FIG. 22.5 The tendon of the stapedius muscle is separated using an argon laser.
FIG. 22.6 A posterior crurotomy is done using the argon laser.
FIG. 22.7 If visible, an anterior crurotomy with laser is done.
FIG. 22.8 By withdrawing the argon laser from the footplate approximately 1 mm the laser beam becomes an effective coagulator for mucosal vessels on the lateral surface of the footplate.
When a sufficient rosette has been created, a fenestra is completed using the side of a straight pick or a rasp while suctioning at the edge of the stapes footplate but never over the fenestra (Fig. 22.10). In case of a thick footplate, a laser may be used at the beginning of the fenestration to devascularize the mucosa overlying the footplate, followed by a microdrill to quickly thin the footplate. The final fenestration may be done with the laser.
Measuring the Length of the Prosthesis
A measuring rod having a diameter of 0.6 mm and calibrated for length is used to determine simultaneously the adequacy of the size of the fenestra and the appropriate length of the piston prosthesis to be used (Fig. 22.11A, B).
Placement and Attachment of the Prosthesis
The Schuknecht Teflon-wire piston consists of a cylindrical piston head made of Teflon (polytetrafluoroethylene) and a malleable piston rod made of 38-gauge (0.004 inch; 0.10 mm) SMO-316 nonmagnetic stainless steel wire. The piston head is 2.5 mm in length and is available in 0.6- and 0.8-mm diameters. One end of the rod is firmly set in the Teflon piston and the other is shaped into an open loop for attachment to the long process of the incus. The prostheses are available from several instrument suppliers in 3.25- to 4.75-mm lengths in increments of 0.25 mm. The combined length of the piston head and rod (exclusive of the loop) is used to identify the length of the prosthesis (Fig. 22.12).
A piston using platinum wire and ribbon has also been developed (Fig. 22.13). It is fashioned after the Schuknecht stainless steel wire Teflon piston and has the advantage of platinum wire shaft and a platinum ribbon loop. The wire allows easy alteration of the angulation once the prosthesis is in place, and the platinum loop provides a wider purchase on the incus. In addition, platinum is also somewhat easier to crimp because it does not have the metallic “memory” of stainless steel.
The prosthesis is grasped at an appropriate angle (Fig. 22.14A, B) and set in place so that the piston enters the fenestra and the wire loop engages the long process of incus in one maneuver. In general, the long axis of the smooth alligator and the prosthesis should be approximately the same. During insertion, if a different angle is required, it can be easily achieved by loosening slightly the grasp on the prosthesis and tapping the prosthesis gently against either the annulus posteriorly or incus anterior to achieve the desired angle. Before the loop is tightened, the mobility of the prosthesis is tested by gently depressing the incus. With this maneuver the prosthesis should move freely within the fenestra. If the patient notices vertigo when this is done, the prosthesis should be removed and replaced with one of a shorter length or modified by cutting off a small segment of the distal part of the piston with scissors. The piston should extend about 0.25 mm into the vestibule.
FIG. 22.9 A: As one method of fenestration, a microdrill using a 0.7-mm cutting and then diamond bur is used to fenestrate the footplate. B: As an alternate to microbur fenestration (Fig. 22.8), the argon laser may be used to fenestrate the footplate. A rosette of laser burns is created in the center of the footplate. Because the diameter of the argon laser fiber-optic bundle is 200 microns, 4 or 5 laser burn diameters are adequate to create a 0.7-mm fenestra. Each burn is characterized by black periphery representing charred bone. A more central white circle represents vaporized bone and a pin hole at the very center represents complete fenestration, through which small droplets of perilymph may be seen.
The loop is then crimped to the incus with sufficient firmness to create a stable linkage (Fig. 22.15). The loop should be securely wrapped around the long process. The posterior blade of the crimping forceps should be parallel to the shaft of the prosthesis. Posterior angulation of the crimping device will result in bending of the straight portion of the wire shaft. Angulating the crimping forceps slightly either superiorly or inferiorly (Fig. 22.16) will allow the operator to monitor the crimping process looking between the two blades of a crimping forceps (Fig. 22.17A, B). Improper closure of the loop (Fig. 22.18A, B) can result in a residual conductive hearing loss or bone erosion from friction caused by a loose prosthesis. After the loop is secured, adjustments may be made in the angle of the prosthesis by bending the wire portion of shaft with a right-angle hook to achieve optimal functional orientation within the fenestra. The success of this maneuver should be monitored by gently elevating the long process of the malleus while watching the motion of the prosthesis. If there is differential motion between the wire loop and incus, friction between the Teflon shaft and the margins of the fenestra should be assumed and a modification of the angle made to achieve smooth motion. A small pledget of Gelfoam soaked in normal saline is placed around the piston (Fig. 22.19). Alternatively, especially if the fenestra is somewhat larger than planned, a tissue graft (e.g., lobular fat or perichondrium) may be used to seal the oval window. The tympanomeatal flap is returned to its anatomic position and held in place with silk strips, soaked in normal saline, and a piece of synthetic sponge or cotton. Antibiotic prophylaxis begun intraoperatively is generally continued for 1 week postoperatively while the rosebud packing is in place. The patient is discharged from the hospital in most cases on the day of surgery or as soon thereafter as the patient’s condition allows.
Only gold members can continue reading. Log In or Register to continue