Chapter 34 Surgery for Locally Advanced Thyroid Cancer
Larynx
 This chapter contains additional online-only content, available on expertconsult.com.
This chapter contains additional online-only content, available on expertconsult.com.
Invasive thyroid cancer is defined as disease that extends outside of the thyroid gland or outside the capsule of metastatic nodes to involve adjacent structures. Several decades ago, the problem of invasive disease was more prevalent, as patients tended to present later in the course of their illness when symptoms brought them to the attention of a physician. In the contemporary era, the increase in the prevalence of thyroid cancer in general is largely, but not exclusively, due to early detection of earlier stage disease.1 The impact of this evolution in thyroid cancer care is that clinicians who are treating thyroid cancer often are lulled into complacency as to the complexity of the required surgery and are not prepared to manage more extensive disease that only becomes evident during the procedure. As such, patients are also not informed as to the potential extent of the surgical procedure required to achieve clear margins.
Invasion of the central compartment visceral and neurologic structures has been reported in a number of articles dating back to the publication by Frazell et al. in 1958.2 The incidence of invasive thyroid cancer in a number of thyroid cancer series ranges from as low as 1% to as high as 23%.3–5 The incidence of invasive disease may be affected by the nature of the referrals to a particular center, as well as the era covered in the given series. In addition, the incidence of invasive disease will be affected by whether the series includes only well-differentiated thyroid cancer or poorly differentiated and anaplastic varieties as well.6 The central compartment visceral structures that may be involved include primarily the larynx, trachea, and esophagus. The neurologic structures include the superior and recurrent laryngeal nerves. Caudal extension of disease or metastatic nodes may lead to vascular involvement of the great vessels and extension to the mediastinum.
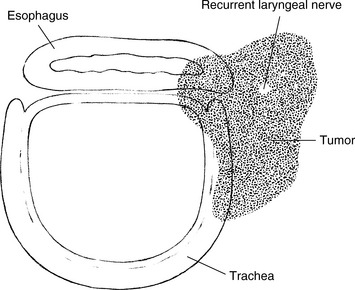
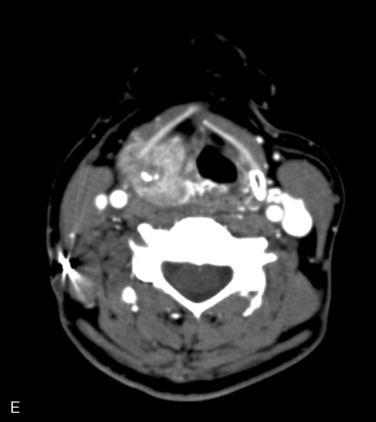
This chapter explores the management of invasive thyroid cancer involving the larynx. Management of the other visceral structures will be covered in other chapters (see Chapters 33, Surgical Anatomy and Monitoring of the Recurrent Laryngeal Nerve, and 35, Surgery for Locally Advanced Thyroid Cancer: Trachea). In virtually every series on invasive thyroid disease, the recurrent laryngeal nerve (RLN) is the most commonly involved central compartment structure. The incidence of RLN involvement was reported by Breaux et al. to occur in 47% of the patients in their series.7 The incidence varied in other series by Fujimoto (56%), McConahey (38%), McCaffrey (47%), Nishida (59%), and Nakao(61%).5,8–11 Several authors have failed to separate laryngeal involvement from tracheal involvement; therefore, the true incidence of laryngeal involvement can be gleaned from only a handful of series. That incidence ranges from 0% reported by Nakao et al. to as high as 34% in the series by Breaux et al.7,11 It is important to state at the outset that invasive thyroid cancer typically involves multiple structures within the central compartment, more often than it involves a single one. For example, in a given patient disease may include the overlying strap muscles as well as the trachea and the esophagus when the invasive disease is situated in the tracheoesophageal groove (Figure 34-1).
 Please see the Expert Consult website for more discussion of this topic.
Please see the Expert Consult website for more discussion of this topic.
In this chapter, we discuss the presenting signs and symptoms, the mechanism for invasion, the diagnosis of invasive disease, and the surgical management of invasion of the larynx. As noted previously, combined visceral invasion is the norm rather than the exception. To be well versed in the management of central compartment invasive thyroid cancer, the reader is advised to review the other chapters that are dedicated to tracheal, recurrent laryngeal nerve, and esophageal invasion in order to understand the full spectrum of preoperative assessment and intraoperative management (see Chapters 33, Surgical Anatomy and Monitoring of the Recurrent Laryngeal Nerve, and 35, Surgery for Locally Advanced Thyroid Cancer: Trachea). The role of postoperative 131I and external beam radiotherapy (EBRT) will be discussed in subsequent chapters (Chapter 52, External Beam Radiotherapy for Thyroid Malignancy).
Presenting Signs and Symptoms of Invasive Thyroid Cancer
1. The patient with biopsy-proved or suspicious disease who is found to have an abnormal examination related to vocal cord dysfunction or the identification of a subglottic or tracheal mass. In addition, the surgeon may identify asymmetry in the pyriform sinuses because of submucosal involvement in that location.
2. The symptomatic patient who presents with biopsy-proved or suspicious disease and a change in voice, dysphagia, dyspnea, or hemoptysis.
3. The patient who presents with biopsy-proved systemic metastases.
4. The patient with recurrent thyroid cancer following prior therapy.
5. The patient with biopsy-proved disease who undergoes preoperative cross-sectional imaging that demonstrates invasion of the visceral structures or extracapsular extension from a metastatic lymph node.
All of the patients in the first four categories should undergo more extensive imaging of the neck and mediastinum to better define the extent of the patient’s primary tumor. Even when cross-sectional imaging fails to show intraluminal extension by thyroid cancer, the surgeon may find involvement of the cartilaginous structure during the operative procedure. Initial findings at presentation will include a palpable neck mass (98% to 100%), hoarseness (18% to 22%), dysphagia (25%), hemoptysis (11% to 25%), or dyspnea (5% to 33%).12,13 Patients with transmural tumor extension will most likely experience symptomatic hemorrhage or impending airway obstruction.12 From 20% to 70% of patients with invasive thyroid carcinoma may present with vocal cord paralysis.12,14 However, a word of caution was noted by Randolph et al. who reported that only one third of the patients with vocal cord paralysis had voice changes. Therefore, the sensitivity of voice changes as a marker for vocal cord paralysis was surprisingly low at only 33%.14
Although virtually all patients with invasive thyroid cancer will present with a palpable neck mass, this finding has a low sensitivity in indicating invasive disease. Thus, in the absence of any other worrisome symptoms, the physical exam and subsequent imaging studies play an important role in diagnosing and evaluating the extent of invasive disease. Physical findings that may suggest invasion include a fixed cervical mass, a mass overlying the thyroid cartilage, or frank adherence or invasion of cervical skin. Because of the low sensitivity of voice changes as a marker for invasion, all patients are required to undergo either indirect or fiberoptic laryngoscopy to assess for true vocal cord paralysis or paresis, blood, pooling of secretions, submucosal changes, or distinct intramural invasion into the larynx, trachea, or hypopharynx. Office-based tracheoscopy and esophagoscopy may be performed to document the extent of invasion, to allow better surgical planning, and for a more comprehensive discussion with the patient.15,16
 Please see the Expert Consult website for more discussion of this topic.
Please see the Expert Consult website for more discussion of this topic.
It is important to realize that not all that is visualized intraluminally in a patient with thyroid cancer represents invasive disease. The authors recently presented their experience with several cases mistaken for invasive thyroid disease. The disease entities included in that series were a benign, intratracheal, thyroid rest in a patient with thyroid cancer; a benign tracheal stenosis adjacent to a benign thyroid nodule; a collision tumor of the larynx and thyroid, involving a papillary thyroid cancer (PTC) and a primary squamous cell cancer of the larynx; a large schwannoma of the recurrent laryngeal nerve with severe tracheal compression; and two cases of chondrosarcoma of the trachea and the larynx. Although the majority of patients with an intraluminal mass in the setting of biopsy-proved thyroid cancer will have invasive disease, the surgeon should maintain a level of awareness of these other entities to ensure that the extent of the planned surgery is appropriate for the patient’s actual disease process.12
Imaging
Imaging modalities have become an integral part of the diagnosis and staging of thyroid cancer. Ultrasonography (US) is widely accepted as the first-line imaging tool. In skilled hands, high-resolution ultrasound is very sensitive and specific in detecting suspicious nodules in the thyroid and metastatic lymph nodes in the lateral neck. However, its role in evaluating extrathyroidal extension involving the trachea, larynx, and esophagus is limited. There are several reports that vary significantly as to the sensitivity of US in detecting tracheal invasion, but no data exist as to the utility of US in laryngeal involvement.17,18 Computed tomography (CT) has a higher sensitivity in detecting central and mediastinal lymph node metastases, as well as evaluating the anatomic extent of extrathyroidal extension.19–21 The use of CT with iodine contrast may delay postoperative therapy with radioactive iodine, but lack of contrast CT may impede its overall sensitivity. In some instances, magnetic resonance imaging (MRI) has been found to be useful in the evaluation of the scope of extrathyroidal extension to surrounding structures.22–24
 Please see the Expert Consult website for more discussion of this topic.
Please see the Expert Consult website for more discussion of this topic.
There are no data to currently suggest a role for FDG-PET or FDG-PET/CT imaging in the evaluation of laryngeal extension of thyroid cancer, but it may have a role in the evaluation of distant metastatic disease especially in the 131I negative patients.25,26 Patients presenting with findings suspicious for thyroid cancer should undergo an initial ultrasound exam including fine-needle aspiration biopsy to confirm the diagnosis. If these patients have further clinical or ultrasound findings suspicious for extrathyroidal or mediastinal extension, a CT or MRI scan should then be performed. Finally, angiography with balloon occlusion studies may be required in patients with extensive extrathyroidal disease involving the great vessels in order to further clarify the surgical planning.
Mechanism for Visceral Invasion by Thyroid Cancer
Many parameters have been identified as important prognostic features in patients with well-differentiated thyroid cancer, including patient age, tumor size, histology, and distant metastases (see Chapter 21, Dynamic Risk Group Analysis for Differentiated Thyroid Cancer). Among the various staging systems that have been proposed for differentiated thyroid cancer, the presence of extrathyroidal extension (ETE) is one of the few that is universally accepted.27–34 In the seventh edition of the American Joint Commission on Cancer Staging Manual, extrathyroidal extension is divided between minimal extension to the sternothyroid muscle or to the overlying soft tissues (T3) and more extensive invasion of the subcutaneous soft tissue, the larynx/trachea, esophagus, and RLN (T4).35 The incidence of ETE increases with increasing size of the primary tumor.36 However, even micropapillary thyroid cancers, less than a centimeter in size, can extend outside the thyroid capsule in as much as 21% of cases.37 The presence of ETE has been associated with an increased incidence of both recurrence and death resulting from disease.38 Breaux and Guillamondegui reported the institutional experience at the MD Anderson Cancer Center and noted an increased incidence of mortality from disease in invasive cancers greater than 4 cm in diameter. In addition, if more than four structures were involved by invasive disease, there were no survivors.7
 Please see the Expert Consult website for more discussion of this topic.
Please see the Expert Consult website for more discussion of this topic.
It is apparent that ETE is a product of both the biologic aggressiveness of the tumor and its location within the gland. Tumors that are subcapsular in location have a much greater likelihood of extending beyond the thyroid parenchyma. The issue of how to define ETE has come into question in a publication by Mete et al.39 The anatomy of the thyroid capsule is poorly understood, and these authors provided a thorough review of the contemporary view of the outer layer of the thyroid gland. The authors concluded that the thyroid gland does not have a true capsule but rather a discontinuous layer of fibroadipose tissue that constitutes a pseudocapsule. Also they point out that the region of the isthmus is unique because of the direct continuity of the thyroid parenchyma with the subcutaneous fat, and there are also normal skeletal muscle fibers located in close proximity to gland parenchyma in this area. As a result, the classification of a tumor as exhibiting ETE must be interpreted carefully. The mere presence of thyroid cancer in direct continuity with subcutaneous tissue or muscle, particularly for a tumor in the isthmus, may not constitute ETE. It is therefore evident that differences in incidence as well as the prognostic significance of ETE may be greatly affected by this ambiguous anatomic detail. Marked ETE, leading to upstaging to pT4, is more readily identified and less controversial.
The presence of extracapsular extension (ECE) in a lymph node is also identified as having an impact on the prognosis and is a cause of invasion of the RLN from paratracheal nodes involved by metastatic disease exhibiting this feature. Yamashita et al. reported the impact of ECE on prognosis, leading to an increased risk of distant disease as well as the risk of dying from disease.40 Leboulleux et al. further identified the number of laryngeal nerves (LNs) with ECE as being an important predictor of recurrent cancer. In that series, the authors found that the presence of fewer than three such LNs was associated with a 10-year recurrence rate of 2%, whereas more than three LNs with ECE led to a 10-year recurrence rate of 38%.41 Finally, Ito identified that both minimal ECE and extensive ECE were associated with a worse cause-specific survival.42
Further classification of invasive thyroid cancer involving the trachea was delineated by Shin et al. who divided the disease into four stages. Stage 1 tracheal invasion involves tumor abutment of the outer perichondrium, but without invasion through it. Stage 2 invasion involves cartilage erosion without transmural extension. In stage 3 invasion, the tumor invades through the cartilage but not through the mucosa. Finally, stage 4 disease is both transcartilaginous and transmucosal. In addition, the stage of invasion had prognostic significance. There was a clear distinction between those patients with stages 1, 2, and 3 disease in which none of the patients died of disease within the first 5 years after surgery, whereas 5 of 11 patients with stage 4 invasion succumbed during that time interval.43 Although it seems apparent that the biologic aggressiveness of thyroid cancer leading to the various stages reported by Shin for the trachea should apply to the larynx, there has been no such classification of the depth of invasion of the larynx by thyroid cancer.
Mechanisms of Involvement of the Larynx in Invasive Thyroid Cancer
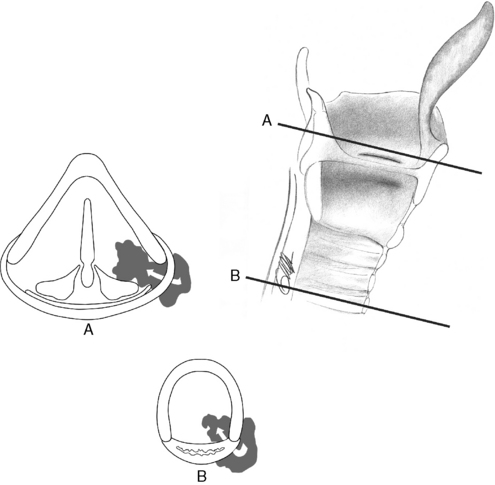
There are three avenues for invasive thyroid cancer to affect the function and the structure of the larynx. The first and most common is by invasion of the RLN directly by the primary tumor or by a metastatic paratracheal lymph node. The second is by direct invasion of the larynx from the primary tumor with extension through the cricoid, the thyroid ala, or the paraglottic space around the posterior aspect of the thyroid cartilage. The last route of invasion is through a metastasis to the cartilage, which happens infrequently (Figure 34-2).
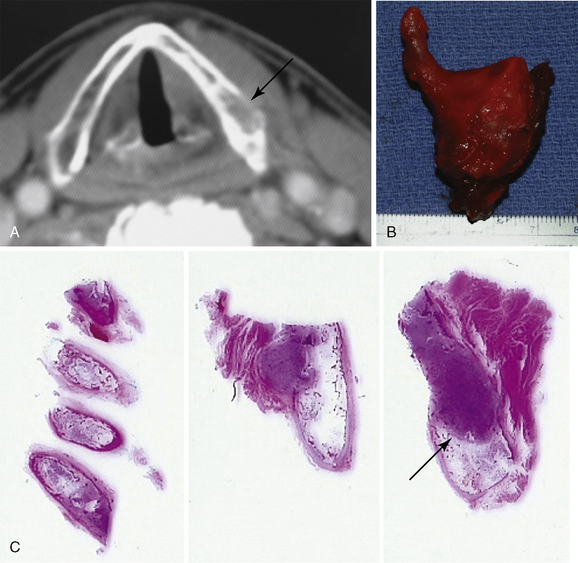
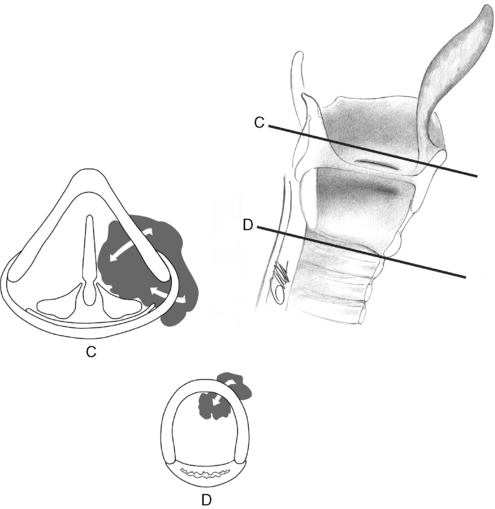
In their review of invasive thyroid cancer treated at the Mayo Clinic from 1940 to 1990, McCaffrey et al. identified four routes of invasion of the laryngotracheal complex. The first is by disease extension from the superior pole around the posterior border of the thyroid ala to involve the paraglottic space. The second route involved invasion of the trachea by a metastatic lymph node. In the third route of spread, the authors described direct invasion of the thyroid ala by disease in the superior pole. Finally, the fourth route of spread was through direct invasion of the cricoid or trachea from a primary tumor in the isthmus10 (Figure 34-3). The whole organ serial section of a patient with invasive papillary thyroid cancer necessitating a total laryngectomy demonstrates most of these pathways for disease spread into the laryngotracheal complex (Figure 34-4).
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


