Supranuclear Control of Eye Movements
Michael X. Repka
Supranuclear centers, located in the brainstem, the cerebellum, the basal ganglia, and the cerebral cortex, direct the movements of the eyes.1 These centers coordinate eye movements and control the response of the eyes to changes in target speed and position, and head position. The function of each of these structures has been inferred from the effects of their destruction, either experimentally or as a result of disease. The supranuclear centers are connected by internuclear pathways; the most important is the medial longitudinal fasciculus.
BRAINSTEM CONTROL CENTERS
Paramedian Pontine Reticular Formation
The abducens nucleus is the key pathway for conjugate horizontal gaze movements. The nucleus contains abducens motor neurons, internuclear neurons, and neurons that project to the paramedian tracts (PMT). The paramedian pontine reticular formation (PPRF) is the brainstem structure responsible for generating horizontal conjugate gaze. The PPRF is positioned ventral to the medial longitudinal fasciculus (MLF) and adjacent to the abducens nerve nucleus. Its major efferent projections are to the ipsilateral abducens nucleus (Fig. 4-1). Secondary efferent projections are to the rostral interstitial nucleus of the MLF (riMLF), which controls vertical gaze. Most afferent connections to the PPRF are from the vestibular nuclei, but there also is input from the cerebellum, superior colliculus, and frontal eye fields (FEF).
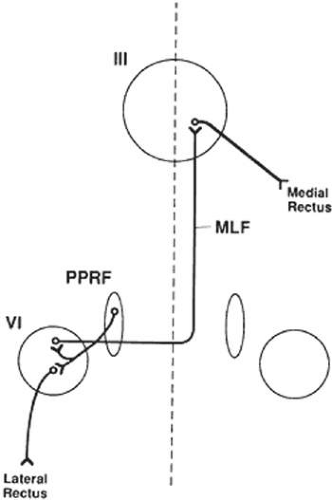 Figure 4-1. The brainstem pathway for horizontal gaze. Supranuclear inputs converge on the paramedian pontine reticular formation (PPRF), the premotor center for horizontal eye movements. The innervation for a horizontal eye movement flows from the ipsilateral PPRF to both an abducens motor neuron and an internuclear neuron in the abducens nucleus. The latter internuclear neuron decussates to the contralateral medial longitudinal fasciculus, where it ascends to reach the contralateral medial rectus subnucleus. |
Three types of cells have been identified in the PPRF: excitatory burst cells, inhibitory burst cells, and omnipause cells. The excitatory burst cells, located rostral to the abducens nucleus, generate ipsilateral horizontal saccades by way of projections to the ipsilateral abducens nucleus. The axons synapse in the abducens nucleus on motor neurons that innervate the ipsilateral lateral rectus and on internuclear neurons that innervate the contralateral medial rectus subnucleus by way of the contralateral MLF (Fig. 4-1). Burst cells discharge only when there is need for a fast eye movement and do not discharge during fixation, pursuit, or vergence eye movements.
Inhibitory burst cell axons have their synapse in the contralateral abducens nucleus. Stimulation of these neurons decreases the firing rate of those motor neurons and internuclear neurons, thereby inhibiting the antagonist muscles of the intended eye movement. Their firing rate is inversely proportional to the burst cells. Omnipause neurons tonically discharge, except when a saccade is being generated. These cells project to both types of burst cells within the ipsilateral PPRF. These cells are important during fixation and smooth pursuit. Abnormalities of the omnipause neurons lead to opsoclonus and ocular flutter.
A lesion of the abducens nucleus causes an ipsilateral gaze palsy. In the rare instance in which there is an isolated lesion of the PPRF, there is an inability to make ipsilateral saccades or have fast phases of nystagmus. However, the response to vestibular stimuli (e.g., oculocephalic testing, caloric) and pursuit will be preserved. This is because there is a direct connection from the contralateral medial vestibular nucleus directly to the abducens nucleus, bypassing the PPRF (Fig. 4-2). These fibers synapse on abducens motor neurons and interneurons to the contralateral medial rectus muscle. Thus, labyrinthine reflex and pursuit eye movements will continue to be generated.
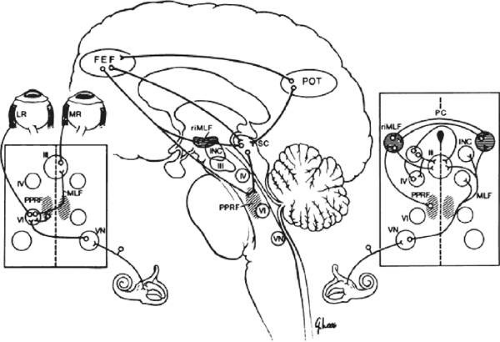 Figure 4-2. Summary of supranuclear control of eye movements. The central figure shows the supranuclear connections from the frontal eye fields (FEF) and the parietal-occipital-temporal (POT) region to the superior colliculus (SC), rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF), and the paramedial pontine reticular formation (PPRF). The FEF and SC are involved in the production of saccades, whereas the POT is important in the production of pursuit eye movements. The left inset shows the brainstem pathways for horizontal gaze. Axons from the cell bodies located in the PPRF travel to the ipsilateral abducens nucleus. In the nucleus, they establish a synapse with abducens neurons, whose axons travel to the ipsilateral lateral rectus (LR) muscle, and with abducens internuclear neurons, whose axons cross the midline and travel in the medial longitudinal fasciculus (MLF) to the subnucleus of the oculomotor nucleus (III) concerned with medial rectus (MR) function in the contralateral eye. Vestibular input for horizontal eye movements comes from the contralateral vestibular apparatus by way of the vestibular nuclei. An axon from the vestibular nucleus crosses to the opposite abducens nucleus, where it innervates a motor neuron and an internuclear neuron for horizontal gaze in the opposite direction. The right inset shows the brainstem pathways for vertical gaze. The region of the riMLF appears to be most important for generating downgaze, whereas the posterior commissure region appears most important for generating upgaze. Vestibular input for vertical gaze arises in the contralateral vestibular nucleus, decussates, and ascends in the MLF to the oculomotor nucleus and the trochlear nucleus. (Miller NR: Walsh and Hoyt’s Clinical Neuro-Ophthalmology, vol 2. 4th ed. Baltimore: Williams & Wilkins, 1985:627) |
Medial Longitudinal Fasciculus
The medial longitudinal fasciculus (MLF) is a fiber tract that extends from the spinal cord to the oculomotor nerve nucleus. It contains primarily ascending fibers, most arise in the superior and medial vestibular nuclei. The MLF is in close proximity to the ocular motor nuclei and influences both ipsilateral and contralateral nuclei. An abnormality of the MLF causes problems with horizontal, vertical, and torsional gaze coordination of the two eyes. A clinically important connection passing through the MLF links the contralateral abducens nucleus with the ipsilateral medial rectus subnucleus. Abnormalities of this tract produce an internuclear ophthalmoplegia. Such a lesion produces slowed or complete loss of adduction of the ipsilateral eye and abducting nystagmus of the fellow eye.
Rostral Interstitial Nucleus of the Medial Longitudinal Fasciculus
The rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF) is located in the mesencephalon at the rostral termination of the MLF. The riMLF has connections to motor neurons in the oculomotor and trochlear nerve nuclei, as well as to the PPRF. On the basis of experimental and pathologic studies, the riMLF appears to be the immediate premotor area for vertical fast eye movements, upward and downward, as well as torsional. These nuclei project to the trochlear nerve and oculomotor nerve nuclei. Its function is thus analogous to the PPRF for vertical eye movements. Damage to this area generally causes more difficulty with downward movement than with upward movement.
This nucleus is adjacent to the interstitial nucleus of Cajal. This structure appears instrumental in vertical and torsional gaze holding. Lesions of this are produce the ocular tilt reaction: an ipsilateral head tilt with depression and extorsion of the ipsilateral eye and an elevation and intorsion of the contralateral eye.2
Posterior Commissure and Nucleus of the Posterior Commissure
Dorsal and rostral to the riMLF is the posterior commissure, a fiber tract that contains some scattered neuronal cell bodies. Lesions in this region produce abnormalities of upward gaze. It is likely that the burst neurons for upward gaze leave here to reach the riMLF before reaching the oculomotor and trochlear nuclei. Involvement of the posterior commissure may be part of the dorsal midbrain syndrome (Parinaud syndrome). In this syndrome, there is impairment of upwardly directed saccades or, in extreme cases, loss of all vertical movement. Other signs include pupillary mydriasis and light-near pupillary dissociation, corectopia, and convergence-retraction nystagmus.
Superior Colliculus
These structures in the dorsal midbrain play a role in both ocular motor and sensory function. The superior colliculus receives visual input directly from branches of retinal ganglion cell axons. Visual input also comes indirectly from the visual cortex, the parietal and frontal lobes, and the substantia nigra. There are efferent projections to the brainstem premotor areas, both PPRF and riMLF. The superior colliculus can generate visually directed saccades independently and may play a role in the control of pursuit eye movements. In primates, ablation of both frontal eye fields (FEF) and both superior colliculi is necessary to produce permanent saccadic defects.
Cerebellum
The cerebellum is involved in the modulation of all types of eye movements, as well as in the long-term adaptive processes that compensate for ocular motor dysmetria. Numerous functions are attributed. These include stabilizing eye on an object (gaze holding), smooth pursuit, combined head and eye tracking, and saccade size and adjustment of the vestibule-ocular reflex. The latter ability is essential for maintaining accurate ocular motor performance during growth and aging, during and after ocular motor disease, or even while using spectacles. For instance, the use of anisometropic spectacles produces a varying anisophoria in different directions of gaze, which must be compensated in each direction of gaze.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


