Superficial Keratopathy
Douglas J. Coster
Corneal surface abnormalities are common. They are important because they can affect vision and are often uncomfortable. The anterior corneal surface, and the tear film it supports, is the most important element in the optical system of the eye. Minor disruptions to epithelium can be painful; it is richly innervated with pain fibers.
The cornea has two distinct functions: first, as an optical element of the eye, the cornea must have a clear, intact ultrastructure for normal vision; second, as a defensive element to protect the internal milieu of the eye. As a protective element, the cornea is equipped to deal with the various challenges facing an exteriorized mucous membrane. It is richly innervated, adjacent to the highly vascularized limbus from which inflammatory cells are recruited, bathed in a constantly moving tear film, and capable of regenerating epithelium rapidly from the limbal stem cells.
The superficial cornea is prone to disease as a result of direct external challenge such as may occur with local infectious agents, from systemic diseases that influence the cornea via the circulation and/or the tear film, such as calcium or immunoglobulin deposition, or from abnormalities of growth and differentiation of the corneal epithelium, such as dysplasia and neoplastic conditions. For some conditions, such as Thygeson’s keratopathy, the etiology is unknown.
It is always important when considering patients with diseases of the superficial cornea to be aware that what is seen in the cornea may be the manifestation of a process affecting the other elements of the outer eye, or even the body as a whole. To understand these conditions, it is helpful to keep in mind two concepts: first, that the outer eye is best considered as a coherent ecosystem, and second, that the corneal epithelium is generated from limbal stem cells.
BIOLOGIC CONCEPTS RELEVANTTO THE OCULAR SURFACE
ECOSYSTEM OF THE OUTER EYE
All elements of the outer eye should be considered as part of an interactive ecosystem rather than as isolated elements. Components of this interactive ecosystem are the tear film, corneal epithelium, corneal stroma, limbus, conjunctiva, and lid margins. This environment is also influenced by more remote structures such as the lacrimal drainage system and the skin of the face. No evaluation of the superficial cornea is complete without careful appraisal of all the elements of the ecosystem of the outer eye.
ROLE OF LIMBAL STEM CELLS
Superficial keratopathy, in its various forms, involves the corneal epithelium. The corneal epithelium is crucial to the optical function of the corneal surface and the protective role of the cornea. It is the bulwark of resistance against microbial infection and is necessary for the integrity of the underlying corneal stroma. Unresolved corneal ulceration may result in the loss of the eye.
Under normal circumstances, the corneal epithelium has considerable capacity for replication and repair. This replicative capacity resides in the limbal stem cells. Disturbances of the limbal stem cell population can have a marked effect on the growth and differentiation of the corneal epithelium, with obvious clinical manifestations. In its most severe form, stem cell insufficiency will result in conjunctivalization of the corneal surface. In slightly less severe form, the corneal epithelium will be seen to be abnormal with patchy opacity and irregularity and underlying vascularization. Corneal epithelial cells migrate centripetally from the limbus and tangentially around the central cornea. Cells that are marked in some way, such as those bearing pigment in pigmented races or those opacified by abnormal depositions, as in Fabry’s disease, clearly demonstrate this patternof movement. This is the basis of vortex kera-topathy.
CLINICAL EXAMINATION
All ophthalmic examinations must begin with a general inspection of the patient, paying particular at-tention to the globe and surrounding adnexal structures. If a broad general inspection is not routinely performed, potentially important diagnostic clues, such as joint abnormalities, telangiectases of the facial skin, seborrhea, eyelid vesicles, and even the pattern of conjunctival injection, can be overlooked. General examination is particularly important when dealing with corneal epithelial keratopathy, which often is the manifestation of a more widespread disorder.
A general external examination is followed by slit-lamp biomicroscopy, which must be methodical and exhaustive. This should begin with observation of the lid margins and the tarsal and bulbar conjunctiva. A suggested approach to corneal examination includes initial inspection under moderate power using the technique of sclerotic scatter. This can highlight minimal changes that might otherwise be missed. Epithelial abnormalities are frequently best identified with broad-beam tangential illumination. Once an epithelial abnormality has been identified, it can be more carefully characterized under higher magnification, using techniques of direct focal illumination, retroillumination, and specular reflection. Some forms of superficial keratopathy can be seen with the naked eye. These lesions are described as “coarse” lesions to distinguish them from “fine” lesions, which can be seen only with magnification.
Even the most skilled biomicroscopist will find it necessary to augment the examination with the use of special staining techniques. Rose bengal, which has an affinity for devitalized corneal and conjunctival epithelial cells as well as for keratin and mucus, is particularly valuable. It is most useful in the diagnosis of keratoconjunctivitis sicca (KCS), and the pattern of staining can be helpful in differentiating various other forms of epithelial disease. Topical fluorescein is no substitute for rose bengal but can complement it because its affinity is different. Fluorescein does not stain epithelial cells but penetrates epithelial defects and can pool or diffuse through intercellular spaces. One drop of 1% rose bengal placed on the upper bulbar conjunctiva while the patient looks down is generally sufficient. Norn has shown that although a 10% solution identified more subtle defects, it could cause artifactual staining and provoke more discomfort on instillation.1
Once a pattern suggestive of superficial corneal pathology is recognized, the examiner may wish to pursue a more pointed history and external examination, seeking additional clues to support a specific pathologic process.
PATTERNS OF MORPHOLOGIC CHANGE IN THE SUPERFICIAL CORNEA
The diagnostic process involves recognizing a typical clinical pattern that is suggestive of particular diagnosis, and then looking for clinical features to support a specific diagnosis and, if necessary, carrying out laboratory investigations to confirm this. Sometimes more than one visit is required to observe the evolution of the process with time, and perhaps in response to treatment, so that a firm diagnosis can be made. For example, a pattern of superficial corneal spots may suggest a viral cause. The additional presence of an acute follicular conjunctivitis with subconjunctival hemorrhages would encourage a clinical diagnosis of adenoviral keratoconjunctivitis. To confirm this would require identification of the virus.
There is another requirement in formulating a diagnostic process: it is necessary to exclude sight-threatening treatable conditions as a priority rather than accept a diagnosis on the grounds of greatest likelihood. In other words, serious diagnoses demand exclusion rather than simply accepting the most likely causes. For example, superficial keratopathy associated with minimal corneal scarring and corneal anesthesia demands exclusion of a neurologic disorder, such as acoustic neuroma, rather than acceptance of the most likely explanation, which is herpetic keratitis.
As in all forms of clinical medicine, the first step in the diagnostic process is to recognize common patterns of disease expression.
The superficial cornea, consisting of Bowman’s layer, the epithelial basement membrane, the epithelium, and the overlying tear film, responds to various disease processes in a limited number of ways. In certain conditions, this response produces a very characteristic pattern of disease, such as the band of rose bengal staining of the cornea and conjunctiva in the palpebral fissure zone caused by KCS. Alternatively, similar patterns of epithelial change can be caused by a wide range of insults, as in the case of diffuse punctate epithelial erosions.
Although corneal ulceration is a commonly encountered pathologic process affecting the superficial cornea, a complete discussion of it is beyond the scope of this chapter; this presentation is confined to the nonulcerative forms of superficial keratopathy. The most important of these are dendriform, plaque, linear, vortex, and superficial punctate keratopathies. Despite the diversity of clinical appearances, these patterns of corneal change share important features. One pattern can be produced by a wide range of pathologic processes, and conversely one etiologic agent can produce more than one pattern of corneal response.
DENDRITIC KERATOPATHY
Corneal epithelial changes characterized by a branching pattern are referred to as dendriform or dendritic keratopathy. The foremost entity manifesting a branching pattern is herpes simplex dendritic keratitis. Few other conditions present with this pattern, but they should be considered in the differential diagnosis of branching epithelial keratopathy. They include healing epithelial abrasions, dendritic plaques in herpes zoster ophthalmicus, and the rare condition of dendriform keratopathy in tyrosinemia (Fig. 1).
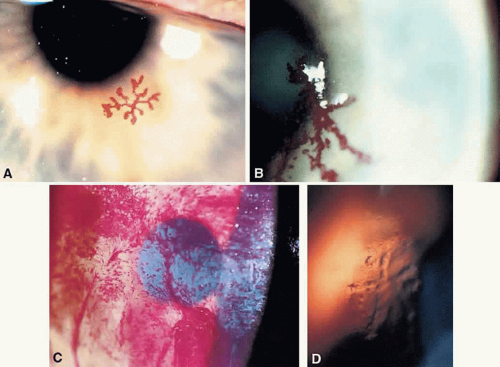 Fig. 1. High-magnification slit-lamp photographs of patterns of superficial keratopathy. A. Dendritic pattern of epitheliopathy without ulceration produced by herpes simplex virus infection. B. Mucous plaques arranged in a branching pattern in a patient with herpes zoster ophthalmicus. C. Branching pattern produced by a healing epithelial defect. D. Corneal lesions of tyrosinemia. |
Herpes simplex dendritic keratitis is a finely branching epithelial lesion that is sharply marginated and frequently associated with terminal end bulbs (see Fig. 1A). Dendritic keratitis may not be truly ulcerative but consists of swollen, infected cells in a dendritic pattern. If the cytopathic process is overwhelming, epithelial cells are shed and a true ulcer is formed.2 The ulcer base stains strikingly with fluorescein, and the marginated, infected cells stain vividly with rose bengal.3,4
Dendriform keratopathy associated with herpes zoster ophthalmicus consists of raised mucus plaques, which usually appear months after the clinical onset and are rarely encountered early in the disease process. They are not difficult to recognize given the patient’s history and clinical appearance. The lesions are coarse (i.e., broad rather than fine), mildly opaque, raised plaques that stain strikingly with rose bengal and poorly with fluorescein5,6 (see Fig. 1B). Fluorescein usually pools about the plaque margin. Débridement results in little damage to the underlying epithelium. It has been assumed that lesions are probably not associated with active viral infection. However, in a recent study in AIDS patients, varicella zoster virus was identified by direct culture of the corneal lesions.7 Although it is exceptionally rare to find herpes simplex and varicella zoster coexisting, they have been encountered together.8
Healing epithelial abrasions can result in a linear or branching pattern along points of epithelial closure (see Fig. 1C). This should not usually be confused with dendritic keratitis because of the history and associated findings. Sliding epithelial cells result in punctate erosions remote from the linear pattern; these stain well with fluorescein or rose bengal, and the staining, distant from the epithelial defect, is helpful in differentiating between the conditions.
Finally, dendritic epithelial figures can be encountered in tyrosinemia type 2, also called the Richner-Hanhart syndrome.9 Primary features are hyperkeratotic skin lesions of the palms, soles, and elbows associated with keratitis in early life. This rare condition is inherited as an autosomal recessive trait with variable phenotypic expression.10 Associated mental retardation is common. Corneal manifestations vary from finely branched intraepithelial opacities resembling small herpetic dendrites9 to severe keratitis with stellate opacification and ulceration.11 The finer intraepithelial lesions do not reach the corneal surface and thus can be distinguished by the absence of staining. The more severe forms appear during the first year of life, with bilateral superficial corneal opacification with radiating opacities forming a pseudoherpetic pattern (see Fig. 1D). Although it is a rare condition, early diagnosis is important, because a striking clinical response can be obtained through dietary therapy.
PLAQUE KERATOPATHY
Adherence of mucus to the corneal epithelium can produce marked symptoms, a striking clinical appearance, and severe sequelae. Two predisposing factors lead to mucus plaque formation: altered corneal epithelium and a relative excess of mucus in the tear film.
Abnormal patches of epithelium function as mucus receptors.6 Foci of abnormal epithelium may result from a number of mechanisms, such as tear film abnormalities, denervation as occurs in herpes zoster ophthalmicus, superficial keratitis due to injury, or inflammation resulting from many causes. A relative excess of mucus can result from aqueous tear deficiency as occurs in KCS,12 altered glycoprotein secretion by goblet cells resulting in increased viscosity of mucus,13 or excess secretion of mucus as occurs in allergic eye disease.
The mucus-epithelium bond can be firm and secure. Filaments result from tenacious adherence between mucus and epithelial cells with subsequent accumulation of epithelial cells, protein, and lipid (Fig. 2A). Filament formation originates from small mucus plaques and may precede ulceration, a serious consequence of plaque formation. Friction between filaments and the upper eyelid can result in small localized areas of epithelial stripping and intense discomfort.
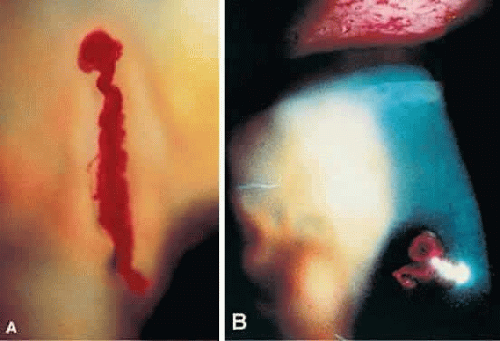 Fig. 2. A. High-magnification photograph of a filament showing a mucous filament based on a patch of abnormal epithelium. B. Slit-lamp photograph of mucous plaques on the corneal surface in a patient with herpes zoster ophthalmicus. |
Plaques vary in size and shape. They may be small and round, as occurs in dry eye states,14 or large and complex in shape, as in herpes zoster ophthalmicus (see Fig. 2B). When associated with aqueous tear deficiency, corneal mucus plaques can occur alone or in conjunction with filaments.2 When a more normal tear film is present, as in herpes zoster ophthalmicus with dendriform corneal plaques, associated filamentary keratitis is uncommon. Similarly, large plaques occurring in vernal keratoconjunctivitis are usually not associated with filamentary keratitis.15
The size, shape, and distribution of plaques and filaments are important considerations. As stated earlier, tear film deficiencies tend to produce numerous small round plaques. Large linear or dendriform lesions occur in herpes zoster ophthalmicus, and large solitary oval plaques occur in vernal keratoconjunctivitis.
Slit-lamp examination together with rose bengal and fluorescein staining reveals the extent and nature of these lesions as well as the general condition of the outer eye. Widespread changes invariably occur in the epithelium, and they are more evident when stained with rose bengal.16 Widespread punctate epithelial erosions are usual, indicating a disturbance of the epithelium-tear film complex. Where mucus adheres to the epithelium, intense staining is apparent.
The most common cause of mucus plaque keratopathy and filamentary keratitis is KCS. One fourth of 66 patients reported on by Fraunfelder and colleagues14 demonstrated corneal plaques at some stage during follow-up. Two thirds of these had Sjögren’s syndrome. The plaques vary in size and shape, being light gray, slightly elevated, and located in the interpalpebral zone or lower two thirds of the corneal surface. Associated filaments are present in more than half of these cases.17 Abnormalities in the tear film, including mucus, epithelial debris, and decreased marginal tear film, together with interpalpebral rose bengal staining, are important ancillary signs. Associated meibomianitis or blepharitis is commonly present and may have a role in increasing mucus viscosity.14
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


