52
Submacular Hemorrhage
Rishi P. Singe  Hilel Lewis
Hilel Lewis
INTRODUCTION
Submacular hemorrhage is a common consequence of choroidal neovascularization (CNV) in patients with age-related macular degeneration (AMD) (Figure 52-1A, 52-1B). It also can be seen secondary to retinal arterial macroaneurysm, trauma, retinopathy resulting from Valsalva’s maneuver and leukemia, and CNV from other causes including presumed ocular histoplasmosis syndrome and high myopia. Observational studies on the natural history of submacular hemorrhage show variable results depending on the underlying cause. Patients with submacular hemorrhage from AMD may develop severe loss of vision, especially if the center of the fovea is involved (1–4). However, submacular hemorrhage from trauma or macroaneurysm may resolve with much less damage to the photoreceptors and retinal pigment epithelium (RPE) (1).
Traditionally, these patients were observed, because precise localization of choroidal neovascular membranes for laser treatment or photodynamic therapy was not possible and other treatment modalities were not available. Recent advances in both submacular surgical techniques and intravitreal anti- vascular endothelial growth factor agents (anti-VEGF) have increased interest in surgical treatment of such patients. Clinical and histopathologic studies published to date do support recommendations regarding surgery and specific interventions for submacular hemorrhage. Although some patients with submacular hemorrhage may benefit from surgical evacuation, the ideal characteristics for good surgical outcomes have not been studied in a randomized large multicenter trial. General guidelines for management can be formulated through our current understandings of histopathological studies and small case series of eyes with submacular hemorrhage.
HISTOLOGY AND PATHOPHYSIOLOGY
How does submacular hemorrhage cause retinal damage? There are a variety of theories that have been formulated based on histological examination of submacular hemorrhage in animal models. It is likely a combination in factors which leads to retinal damage after submacular hemorrhage. First, toxicity may occur resulting from iron released from hemoglobin (5). Second, the blood may act as a barrier, impairing metabolic exchange between the photoreceptors and RPE. Finally, fibrin-mediated mechanical damage to the outer retina may occur because of clot contraction (6, 7).
Glatt and Machemer (5) demonstrated irreversible damage to the photoreceptors within 24 hours after introduction of subretinal blood in a rabbit model and outer retinal degeneration within 3 to 7 days. Toth et al. (7) looked at the early events associated with subretinal hemorrhage in a cat model. The most striking finding in their study was the rapid formation of a fibrin clot interdigitating between the photoreceptor outer segments. This was seen within the first hour of introduction of subretinal hemorrhage. Mechanical shearing of the photoreceptors resulting from traction of fibrin strands followed. The most severe retinal degeneration occurred over the ensuing 3 to 14 days and was found over the areas of dense fibrin coagulum, as opposed to the areas of dense erythrocytes. The authors proposed that fibrin and perhaps other inflammatory products are responsible for the retinal damage rather than iron toxicity or the presence of erythrocytes as a barrier to diffusion. If tissue plasminogen activator (t-PA), a clot- specific fibrinolytic agent, was injected into the subretinal space along with the blood, mechanical shearing of the photoreceptors was not seen. This confirmed the initial observation by Lewis and coauthors that fibrinolytic therapy may be a useful adjunct to surgical removal of subretinal hemorrhage (6).
Lewis et al. (6) also studied the effect of recombinant t-PA on experimental subretinal hemorrhage in rabbits. Subretinal hemorrhage created by injection of blood alone was compared with simultaneous injection of blood and t-PA or blood and balanced salt solution (BSS). Clearance of subretinal hemorrhage was significantly faster in eyes given t-PA than in those given BSS or blood alone. Additionally, eyes receiving t-PA or BSS sustained less degenerative change in retinal appearance and retained larger numbers of well-organized retinal outer segments than those receiving blood alone. It is postulated that this beneficial effect of both t-PA and BSS may be caused by dilution of toxic factors released by lysed blood cells, as well as a reduction in metabolic barrier from clot in the subretinal space.
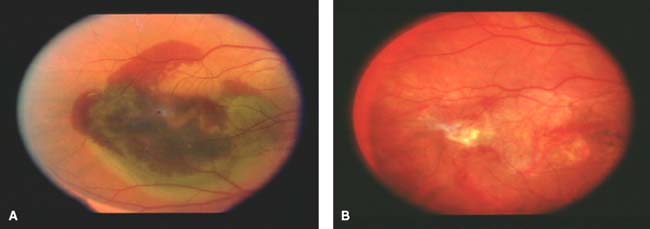
Figure 52-1. A: Preoperative photo demonstrating submacular hemorrhage due to age-related macular degeneration. Visual acuity count fingers at 3 feet. B: Postoperative photo with complete resolution of submacular hemorrhage, localized atrophy, and subretinal fibrosis. Visual acuity is 20/400.
Terasaki et al. (8) evaluated the changes in preoperative versus postoperative focal macular electroretinography in five patients undergoing surgical drainage of submacular hemorrhages. Preoperative electroretinographic response was reduced remarkably or was unrecordable in all eyes. Postoperative electroretinographic responses, recorded between 1 and 4 months after surgery, recovered to about one half of the amplitude of the normal fellow eye. These findings showed that the severe retinal dysfunction associated with submacular hemorrhage can be reversed at least partially with surgical intervention (8).
NATURAL HISTORY
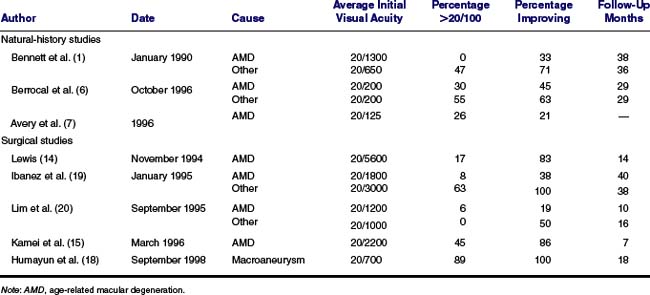
Observational studies in humans have shown a wide variability in the natural course of subretinal hemorrhage (Table 52-1A, 52-1B). The largest series to date reviewed by Scupola et al. (4) examined sixty eyes with submacular hemorrhage due to AMD. In this retrospective series, vision deteriorated in 80% of patients with a mean initial acuity of 20/240 and a mean final acuity of 20/1250 at 24 months follow-up. Worse visual outcome was correlated with larger initial hemorrhage size and greater initial retinal thickness. The natural dissolution of hemorrhage varied from 2 to 18 months and recurrent bleeding occurred in 38% of eyes. At the end of the study, 25% had atrophic scars, 38% had subretinal fibrosis, and 22% had RPE tears (4).
Bennett et al. (1) highlighted the variable outcome of submacular hemorrhage from causes other than AMD. In this study, 29 patients with subretinal hemorrhages greater than one disc diameter involving the center of the fovea were included. The cause of hemorrhages in this study included (listed in descending order of frequency) choroidal neovascular membranes associated with AMD, ruptured retinal arterial macroaneurysms, traumatic choroidal rupture, choroidal neovascular membranes associated with presumed ocular histoplasmosis syndrome and pseudoxanthoma elasticum, and complications of scleral buckling surgery. Initial visual acuities varied widely, from 20/70 to light perception (average 20/860). Final visual acuities with a mean follow-up of 3 years also varied widely, from 20/30 to light perception (average 20/480). The most important predictor of poor visual outcome was the presence of AMD. The average final visual acuity in patients with AMD was 20/1700, and none of these patients had a final visual acuity better than 20/200. Patients with submacular hemorrhage associated with other causes of choroidal neovascular membranes also had poor outcomes, with the exception of one patient with presumed ocular histoplasmosis syndrome whose visual acuity improved from 20/200 to 20/30. The patients with the best outcomes in this series were those with subretinal hemorrhages from traumatic choroidal rupture. This may be explained partly by the fact that, on average, patients with hemorrhages from choroidal rupture had better initial visual acuity than patients with AMD, and all of the traumatic hemorrhages were classified as thin (1).
Berrocal et al. (3) reviewed fundus photographs and medical records of 31 patients with subretinal hemorrhage involving the entire foveal avascular zone. The majority of hemorrhages were associated with AMD. In the remaining eyes, hemorrhages were secondary to retinal arterial macroaneurysms, presumed ocular histoplasmosis syndrome, trauma, and retinopathy resulting from Valsalva’s maneuver, idiopathic central serous choroidopathy, central retinal vein occlusion, and CNV associated with choroidal rupture. The mean time to clearance of all subretinal hemorrhages was 7 months (range 2 months to 24 months). Initial and final visual acuities in this study were significantly better than in Bennett’s study. Final visual acuity was 20/80 or better in 19% of the patients with AMD. The size or thickness of the hemorrhage was not predictive of final visual outcome in this study. Again, patients with submacular hemorrhages from other causes faired better than those with AMD (3).
TABLE 52-1 COMPARISON OF NATURAL-HISTORY STUDIES AND SURGICAL STUDIES
Avery et al. (2) examined only patients with AMD and subretinal hemorrhages extending beneath the center of the fovea resulting from choroidal neovascular membranes. At 36 months, 44% lost six or more lines, 22% lost two to five lines, 12% retained vision within one line, and 21% had maintained spontaneous improvement of two or more lines. Their analyses suggested that eyes with large hemorrhages or moderate to marked retinal elevation have poorer visual prognosis. This series again confirmed the poor natural visual outcomes in patients with submacular hemorrhage secondary to AMD (2).
These reports, although useful, do not provide us with accurate information on the natural history of submacular hemorrhage because they only included a small number of patients, the follow-up was limited, and the studies were retrospective. From the limited information to date, it is likely that eyes with very large or thick hemorrhages beneath the fovea, the location of the hemorrhage with respect to being above or below the RPE, the length of time the hemorrhage has been present, and any associated abnormalities of the retina or RPE are likely to have poorer prognoses (1, 3). Further, most patients with submacular hemorrhages associated with CNV (particularly in AMD) have a poorer visual outcome. Several factors may account for the apparently worse visual prognosis for patients with submacular hemorrhage in AMD. Some authors have proposed that diffuse preexisting abnormalities involving Bruch’s membrane, the RPE, and the retina may limit the metabolic reserves of these tissues and result in diminished ability to tolerate the presence of subretinal hemorrhage (9). The scarring process of CNV also plays a role in retinal damage in these eyes.
The most recent report of the Submacular Surgery Trials (SST) evaluating surgery for hemorrhagic choroidal neovascular lesions for AMD gives also helpful insight into the natural history by examining the nontreatment arm. In this randomized, prospective, multicenter clinical trial, patients were randomized to surgical removal versus observation. Patients had predominately hemorrhagic subfoveal lesions in which at least 50% of the choroidal neovascular lesion was occupied by thick blood. Eligible lesions were between 3.5 disc areas and 9 disc areas and median initial acuity was 20/200. The final median acuity at 36 months was 20/640 with 44% of eyes maintaining or improving acuity over the length of the study (10). However, it should be noted that patients within the SST need not have subfoveal hemorrhage in order to be enrolled within the trial, rather that they just needed subfoveal CNV.
SURGICAL MANAGEMENT
For thin localized subretinal hemorrhages due to AMD, intravitreal anti-VEGF agents may be suitable therapy. However, there are currently no medical treatments for thick larger submacular hemorrhages and the only alternative to observation is surgery. With recent improvements in vitreoretinal surgical techniques and instrumentation, surgical displacement or removal of submacular hemorrhage is possible.
INITIAL SURGICAL APPROACHES
Surgical techniques for the removal of submacular hemorrhage have significantly evolved over the past 10 years. The earliest attempts to drain large submacular hemorrhages used a transscleral approach. In 1983, Dellaporta described passing an endodiathermy probe through the sclera, choroid, and retina, allowing the blood to pass into the retroscleral space and also into the vitreous cavity. Lasers also have been used to create retinotomies, allowing blood to spill into the vitreous cavity (11, 12). Hanscom and Diddie first used vitrectomy with internal retinotomy, endodrainage, and air-fluid exchange in the management of submacular hemorrhage (13). Several others also adopted this approach. With it, large access retinotomies were required, which were associated frequently with postoperative retinal detachment and proliferative vitreoretinopathy (14, 15). Additionally, mechanical clot extraction usually was required, which could result in damage to photoreceptors or the RPE at the time of removal.
VITRECTOMY WITH DISPLACEMENT UTILIZING TISSUE-PLASMINOGEN ACTIVATOR
Modern vitrectomy techniques now utilize recombinant t-PA to lyse the fibrin within the clot, prior to removal of the liquefied blood. t-PA converts fibrin-bound plasminogen to plasmin, thereby producing clot lysis. The toxicity of arginine (used as a carrier for t-PA) to the retina and RPE has been established in numerous studies (16, 17). A 48 μg dose of t-PA is sufficient in most cases to engulf the subretinal clots. This dose is below the rabbit and cat studies which have shown dose dependent toxicities at concentrations greater than or equal to 50 μg (6, 17, 18). Retinal toxicity from t-PA is thought to be due to the vehicle manifests as diffuse pigmentary alterations sparing the posterior pole, poor visual acuity after the absorption of submacular hemorrhage, and reduced scotopic and photopic electroretinogram (ERG) A and B-waves. This toxicity has been seen in humans between 50 to 100 μg.
TABLE 52-2 TISSUE PLASMINOGEN ACTIVATOR FOR SUBMACULAR HEMORRHAGE 1998 UPDATE (N = 42, FOLLOW-UP = 10 MO)
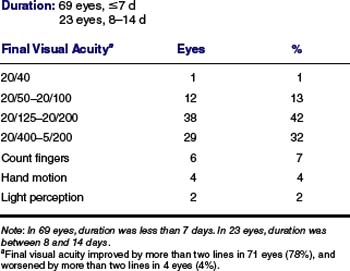
The current indications for surgical evacuation of submacular hemorrhage are based on the results of pilot studies (19, 20). In general, surgery should be considered in patients with good vision before the hemorrhage occurred (those with CNV of long duration prior to the hemorrhage are unlikely to benefit from surgery); patients with duration of hemorrhage less than 14 days; patients with hemorrhage more than 500 μm thick beneath the center of the foveal avascular zone and greater than 3.5 Macular Photocoagulation Study disc diameters in size; hemorrhage posterior to the midpoint between the temporal arcades and the equator, and patients without hemorrhage beneath the RPE (Table 52-2).
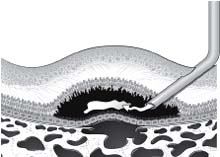
The current technique for surgical removal of submacular hemorrhage is as follows (Figure 52-2A, 52-2B, 52-2C). A standard three-port pars plana vitrectomy is performed with the induction of a posterior vitreous detachment. The intraocular pressure is increased to cause central retinal artery occlusion. A specially designed, sharp, bent, 36-gauge spatula is used to enter the subretinal space and create a tunnel between the RPE and the outer retina. If the hemorrhage is limited to the macular region or posterior pole, a 130-degree bent spatula is used. If the subretinal hemorrhage is more extensive, however, reaching the equator or more anteriorly, a 90-degree bent spatula is used to prevent damage to the retina from the heel of the instrument. A 33-gauge bent cannula then is placed through the retinotomy, and recombinant t-PA is injected into the subretinal clot. We use a concentration of 12.5 μg per 0.1 ml of BSS, but this concentration also depends on the size and volume of the clot. Care is taken to inject directly into the clot rather than between the clot and the RPE or between the clot and the outer retina. This is to avoid damage to the RPE or outer retina from the injection. Enough t-PA solution is injected to bathe the entire subretinal clot, up to 50 μg. The intraocular pressure then is lowered gradually to normal levels. Diathermy or endophotocoagulation of the access retinotomy is not necessary given the size and location.
In initial studies, a 45- to 60-minute intraoperative clot lysis was necessary followed by the injection/aspiration of BSS into the subretinal space. However, a recent modification of the technique has shown that this intraoperative waiting period is unnecessary. Instead, a partial air fluid exchange is performed and approximately 70% of the vitreous cavity is filled with air. The patients are taken to the recovery room in the supine position for 1 hour and then the patients are positioned upright or on their side for 24 hours. A neck collar can assist in the proper upright positioning.
With this method, mechanical clot extraction is unnecessary and inadvertent retinal damage can be avoided (19). It is not necessary to remove all of the hemorrhage if the area beneath the fovea is clear. If hemorrhage remains beneath the fovea, perfluorocarbon liquid may be utilized to displace it away from the fovea or through the retinotomy into the vitreous cavity (referred to as the steamroller technique).
PNEUMATIC DISPLACEMENT WITHOUT VITRECTOMY
Hassan et al. first published papers with a series of patients treated with intravitreal t-PA (0.1 to 0.2 ml of t-PA; total dose 25 to 100 μg), expansile gas, and prone positioning for 1 to 5 days (21). Numerous series have followed demonstrating some benefit to this procedure (22). However, experimental evidence suggests that t-PA injected into the vitreous space does not cross the sensory retina and does not reach the subretinal space (23). Furthermore, previous animal work demonstrated that submacular hemorrhage clot interdigitates between the photoreceptor outer segments. If the clot is not fully liquefied and the gas is applied, potentially more photoreceptors are likely to be damaged with this procedure.
SURGICAL RESULTS
Although several series on surgical removal of submacular hemorrhage have been published, it is difficult to directly compare their results because of marked variability in patient selection, surgical techniques employed, length of follow-up, and methods of assessing visual outcome (19, 20, 24–28). Despite these shortcomings, a comparison of the surgical studies and the natural history studies with regard to initial visual acuity, percentage of eyes with final visual acuity greater than 20/100, percentage of eyes with improvement in final visual acuity, and length of follow-up was performed (Table 52-1A, 52-1B). In all published reports, visual outcomes were worst for patients who underwent submacular surgery for hemorrhage secondary to AMD than for other causes. This may be in part because, as shown by Gass, the CNV and hemorrhage in AMD often are found beneath the RPE, and only secondarily break through into the subretinal space (29).
The percentage of patients with AMD who had an improvement in final visual acuity after surgery varied widely from 19% to 86% (average of 58%). Studies of the natural history of submacular hemorrhage secondary to AMD reported that 21% to 45% of patients had an improvement in visual acuity (average 33%). We must be careful, however, not to interpret these as results as showing the benefits of submacular surgery because these studies are not comparable.
We recently summarized our results which included 34 eyes with subretinal hemorrhage secondary to AMD in patients who underwent surgical drainage using t-PA with no intraoperative clot lysis time. Complete postoperative displacement of blood from the fovea was achieved in 50% of patients. Final visual acuity improved by two or more lines in 64% and the visual acuity improved by six lines in 29%, and worsened by two or more lines in 21%. Stabilization or improvement in visual acuity was obtained in 85% at 3 months, 77% at 6 months, and 75% at 12 months.
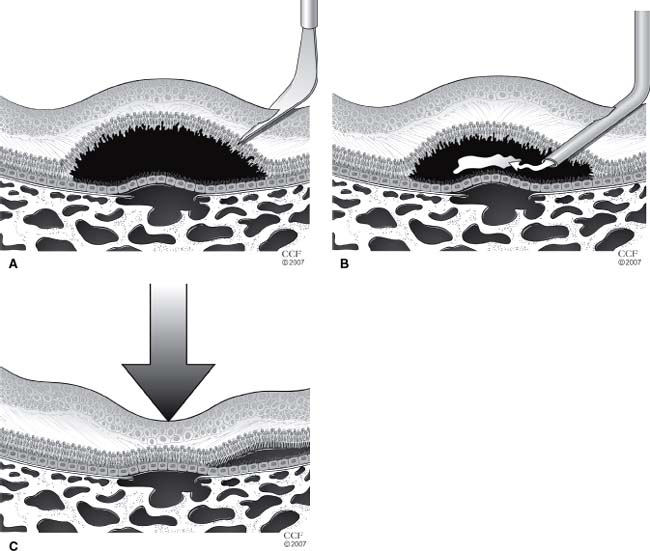
Figure 52-2. A: A 130-degree bent spatula is used to create a retinotomy into the subretinal space. B: A 33-gauge bent cannula is then placed through the retinotomy, and recombinant tissue plasminogen activator is injected into the subretinal clot. C: The hemorrhage is displaced with the intraocular air bubble.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


