Subjective Refraction: Fogging and Use of the Astigmatic Dials
Jay H. Kaufman
History
Today’s ophthalmologist is the beneficiary of a long and sometimes controversial process that has resulted in the development of modern refractive techniques. Historically, two methods of refraction evolved, objective and subjective, each with its special advantages and disadvantages. In the objective method, the examiner made measurements to determine the proper spectacle prescription without enlisting the patient’s responses. Objective techniques ultimately evolved into the use of retinoscopy and automated refractors. The other, subjective, method depended more on the responses that the patient gave to the examiner’s questions. This could be used as a primary method of refraction, but could also be used as a means of verifying the refractive error as estimated objectively.
Subjective refraction offered certain advantages: Refraction could be done without cumbersome equipment and in the absence of a good pupillary reflex. Because the patient decided on the most desirable prescription, uncomfortable spectacles were less likely to be prescribed. However, subjective refraction often produced variable results because of a natural tendency for the patient to accommodate during the examination. For this reason, when cycloplegia was introduced into refraction, ophthalmologists hailed it as a major asset to subjective methods, although it brought with it another set of disadvantages and complications.
Gradually a subjective refractive technique using fogging and the astigmatic dials was developed that had a high degree of reliability and has retained its usefulness. This technique minimized the problem of accommodation while providing a sensitive measure of the patient’s astigmatism. It has not replaced the standard objective refractive methods that most examiners continue to use, but it does offer an alternative or adjunctive technique that may be preferable for use in some patients. In addition, it is a useful means of verifying a prescription obtained objectively.
The technique dates back to the nineteenth century. Lancaster1 credited Donders with using a star-shaped figure made up of radiating lines as a practical test for astigmatism as early as 1860. Green perfected the astigmatic dial while working with Donders and Snellen from 1866 to 1869. In 1899, Verhoeff2 suggested a chart with two principal meridians to measure the amount of astigmatism. Lancaster himself laid much of the important groundwork for popularizing the technique, and alone and later with Regan taught the refined method.3,4
Numerous variations of the astigmatic dials became available (Fig. 39-1). The number 1 charts include sunburst charts, clock dials with lines at intervals of 30°, and other dials with lines at more frequent intervals, most popularly at 10°. The number 2 dial, or Lancaster cross, consists of two perpendicular lines that can be rotated to any position needed.
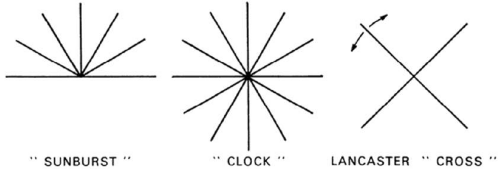 Fig. 39-1. Number 1 and number 2 astigmatic dials. |
Optical Principles of the Method
There are two components to this subjective technique: fogging to eliminate accommodation, and use of the astigmatic dials to determine the magnitude and axis of astigmatism. Optically, fogging means artificial blurring of vision, identical to the naturally occurring state of myopia. It is accomplished by placing convex lenses in front of the eye. Fogging induces relaxation of accommodation because conditions are so arranged that accommodation would blur visual acuity further (Figs. 39-2 and 39-3).
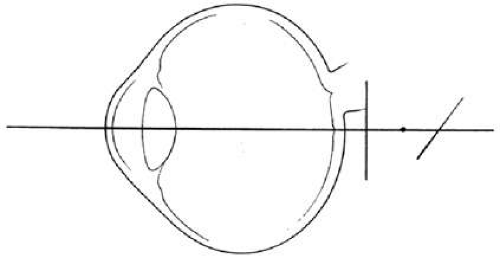 Fig. 39-2. An eye with compound hyperopic astigmatism in which both focal lines are behind the retina. |
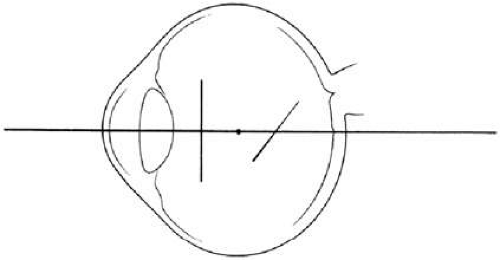 Fig. 39-3. After an adequate fog is achieved, the patient’s error has been converted to compound myopic astigmatism. Accommodation would pull the focal lines farther from the retina.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|