9
Strabismus Disorders
Scott E. Olitsky and Leonard B. Nelson 
PSEUDOESOTROPIA
Epidemiology and Etiology
 Pseudoesotropia is one of the most common reasons an ophthalmologist is asked to evaluate an infant. In some series, up to half of children with suspected strabismus were found to have pseudoesotropia.
Pseudoesotropia is one of the most common reasons an ophthalmologist is asked to evaluate an infant. In some series, up to half of children with suspected strabismus were found to have pseudoesotropia.
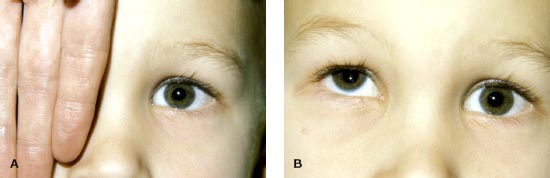
 Pseudoesotropia is characterized by the false appearance of strabismus when the visual axes are actually aligned (Fig. 9-1).
Pseudoesotropia is characterized by the false appearance of strabismus when the visual axes are actually aligned (Fig. 9-1).
History
 Pseudoesotropia is usually caused by a flat, broad nasal bridge; prominent epicanthal folds; or a narrow interpupillary distance. An observer may perceive less white sclera nasally than would be expected, and the impression is that the eye is turned in toward the nose, especially when the child looks to either side.
Pseudoesotropia is usually caused by a flat, broad nasal bridge; prominent epicanthal folds; or a narrow interpupillary distance. An observer may perceive less white sclera nasally than would be expected, and the impression is that the eye is turned in toward the nose, especially when the child looks to either side.
Differential Diagnosis
 Small-angle strabismus
Small-angle strabismus
 Intermittent strabismus
Intermittent strabismus
Diagnostic Evaluation
 Pseudoesotropia can be differentiated from true strabismus when the corneal light reflex is seen to be centered in both eyes or when the cover–uncover test shows no refixation movement.
Pseudoesotropia can be differentiated from true strabismus when the corneal light reflex is seen to be centered in both eyes or when the cover–uncover test shows no refixation movement.
 Tightening the epicanthal folds by pinching the bridge of the nose can also be effective in demonstrating that the “crossing” is not real.
Tightening the epicanthal folds by pinching the bridge of the nose can also be effective in demonstrating that the “crossing” is not real.
 A complete evaluation should be performed, including cycloplegic refraction, to rule out excessive hyperopia that could be causing intermittent esotropia.
A complete evaluation should be performed, including cycloplegic refraction, to rule out excessive hyperopia that could be causing intermittent esotropia.
Treatment
 No treatment is needed. Parents can be reassured that most children will outgrow the appearance of crossing.
No treatment is needed. Parents can be reassured that most children will outgrow the appearance of crossing.
Prognosis
 As the child grows, the bridge of the nose becomes more prominent and displaces the epicanthal folds, and the medial sclera becomes proportional to the amount visible on the lateral aspect of the eye. Parents should be cautioned that children with pseudoesotropia, like any child, can develop true strabismus later in life. Therefore, if a change in appearance occurs, a repeat evaluation may be warranted.
As the child grows, the bridge of the nose becomes more prominent and displaces the epicanthal folds, and the medial sclera becomes proportional to the amount visible on the lateral aspect of the eye. Parents should be cautioned that children with pseudoesotropia, like any child, can develop true strabismus later in life. Therefore, if a change in appearance occurs, a repeat evaluation may be warranted.
FIGURE 9-1. Pseudoesotropia caused by a wide nasal bridge and epicanthal folds. Note that the child is looking slightly to the left which also accentuates the fale appearance that there is less sclera in the right eye.

CONGENITAL (INFANTILE) ESOTROPIA
Epidemiology and Etiology
 The cause of congenital esotropia is unknown. Theories include both a primary defect in sensory development of the brain that leads to the abnormal alignment as well as a primary “motor” theory in which the ocular misalignment is the primary abnormality, which then leads to a secondary disruption of binocular vision. It is likely that both causes exist and may also be equally responsible for the development of the disorder in many children.
The cause of congenital esotropia is unknown. Theories include both a primary defect in sensory development of the brain that leads to the abnormal alignment as well as a primary “motor” theory in which the ocular misalignment is the primary abnormality, which then leads to a secondary disruption of binocular vision. It is likely that both causes exist and may also be equally responsible for the development of the disorder in many children.
The incidence of congenital esotropia is approximately 1 in 1000 children.
Signs and Symptoms
 Few children who are eventually diagnosed with this disorder are actually born with an esotropia. Although parents often give a history of their child’s eyes crossing since birth, the crossing is rarely seen in the newborn nursery and is generally not observed during the first few weeks of life.
Few children who are eventually diagnosed with this disorder are actually born with an esotropia. Although parents often give a history of their child’s eyes crossing since birth, the crossing is rarely seen in the newborn nursery and is generally not observed during the first few weeks of life.
 The diagnosis is generally made when an infant presents before 6 months of age with a large (≥30 prism diopter), constant esotropia, full abduction, a normal level of hyperopia, and no underlying ophthalmic disorder that could lead to vision loss and a secondary strabismus (Fig. 9-2). Children with congenital esotropia often appear to exhibit an apparent abduction deficit. This pseudoparesis is usually secondary to the presence of cross-fixation. If the child has equal vision, he or she will have no need to abduct either eye. The child will use the adducted, or crossed, eye to look to the opposite field of gaze. In this case, he or she will show a bilateral pseudoparesis of abduction. If amblyopia is present, only the better-seeing eye will cross fixate, making the amblyopic eye appear to have an abduction weakness. To differentiate between a true abducens paralysis and a pseudoparalysis, a doll’s head maneuver can be used or abduction can be examined after the infant has worn a patch over one eye for a period of time.
The diagnosis is generally made when an infant presents before 6 months of age with a large (≥30 prism diopter), constant esotropia, full abduction, a normal level of hyperopia, and no underlying ophthalmic disorder that could lead to vision loss and a secondary strabismus (Fig. 9-2). Children with congenital esotropia often appear to exhibit an apparent abduction deficit. This pseudoparesis is usually secondary to the presence of cross-fixation. If the child has equal vision, he or she will have no need to abduct either eye. The child will use the adducted, or crossed, eye to look to the opposite field of gaze. In this case, he or she will show a bilateral pseudoparesis of abduction. If amblyopia is present, only the better-seeing eye will cross fixate, making the amblyopic eye appear to have an abduction weakness. To differentiate between a true abducens paralysis and a pseudoparalysis, a doll’s head maneuver can be used or abduction can be examined after the infant has worn a patch over one eye for a period of time.
Differential Diagnosis
 Pseudoesotropia
Pseudoesotropia
 Duane’s retraction syndrome
Duane’s retraction syndrome
 Mobius syndrome
Mobius syndrome
 Congenital sixth nerve palsy
Congenital sixth nerve palsy
 Early-onset accommodative esotropia
Early-onset accommodative esotropia
 Sensory esotropia
Sensory esotropia
 Esotropia in the neurologically impaired
Esotropia in the neurologically impaired
Diagnostic Evaluation
 All children with suspected congenital esotropia should under a complete examination, including a dilated funduscopic evaluation and cycloplegic refraction to rule out possible early onset accommodative esotropia or a secondary strabismus (Fig. 9-3).
All children with suspected congenital esotropia should under a complete examination, including a dilated funduscopic evaluation and cycloplegic refraction to rule out possible early onset accommodative esotropia or a secondary strabismus (Fig. 9-3).
 Amblyopia can be diagnosed by looking for a fixation preference.
Amblyopia can be diagnosed by looking for a fixation preference.
 If an accommodative component to the crossing is considered to be a possibility, the child should be given the full cycloplegic refraction and reevaluated to look for any effect on the crossing.
If an accommodative component to the crossing is considered to be a possibility, the child should be given the full cycloplegic refraction and reevaluated to look for any effect on the crossing.
Treatment
 The treatment for congenital esotropia consists of strabismus surgery. Surgery is performed after any associated amblyopia, if present, is treated. It is important to treat amblyopia before surgery. It is much easier to follow the progress of amblyopia in a preverbal child while his or her eyes are crossed. In addition, parental compliance with amblyopia treatment tends to be much lower after the eyes are straightened and appear “normal.”
The treatment for congenital esotropia consists of strabismus surgery. Surgery is performed after any associated amblyopia, if present, is treated. It is important to treat amblyopia before surgery. It is much easier to follow the progress of amblyopia in a preverbal child while his or her eyes are crossed. In addition, parental compliance with amblyopia treatment tends to be much lower after the eyes are straightened and appear “normal.”
 The primary goal of treatment in congenital esotropia is to eliminate or reduce the deviation as much as possible. Ideally, this results in normal visual acuity in each eye, straight-looking eyes, and the development of binocular vision.
The primary goal of treatment in congenital esotropia is to eliminate or reduce the deviation as much as possible. Ideally, this results in normal visual acuity in each eye, straight-looking eyes, and the development of binocular vision.
Prognosis
 Children with congenital esotropia do not develop normal (bifoveal) binocular vision. Successful treatment provides the opportunity to develop some degree of binocular vision (monofixation syndrome), which allows the development of motor fusion, which helps to keep their eyes aligned.
Children with congenital esotropia do not develop normal (bifoveal) binocular vision. Successful treatment provides the opportunity to develop some degree of binocular vision (monofixation syndrome), which allows the development of motor fusion, which helps to keep their eyes aligned.
 Even with successful initial treatment, many children with a history of congenital esotropia may redevelop strabismus or amblyopia and therefore need to be monitored closely during the visually immature period of life.
Even with successful initial treatment, many children with a history of congenital esotropia may redevelop strabismus or amblyopia and therefore need to be monitored closely during the visually immature period of life.
 Recurrent horizontal strabismus is common as are vertical deviations. These may develop months or years after the initial surgery has been performed. The two most common forms of vertical deviations to develop are inferior oblique muscle overaction (IOOA) and dissociated vertical deviation (DVD).
Recurrent horizontal strabismus is common as are vertical deviations. These may develop months or years after the initial surgery has been performed. The two most common forms of vertical deviations to develop are inferior oblique muscle overaction (IOOA) and dissociated vertical deviation (DVD).
REFERENCES
Archer SM, Sondhi N, Helveston EM. Strabismus in infancy. Ophthalmology. 1989;96:133.
Arthur BW, Smith JT, Scott WE. Long-term stability of alignment in the monofixation syndrome. J Pediatr Ophthalmol Strabismus. 1989;26:224.
Birch E, Stager D, Wright K, et al. The natural history of infantile esotropia during the first six months of life. J AAPOS. 1998;2:325–328.
Birch EE, Stager DR, Everett ME. Random dot stereoacuity following surgical correction of infantile esotropia. J Pediatr Ophthalmol Strabismus. 1995;32:231.
Hiles DA, Watson A, Biglan AW. Characteristics of infantile esotropia following early bimedial rectus recession. Arch Ophthalmol. 1980;98:697.
Ing M, Costenbader FD, Parks MM, et al. Early surgery for congenital esotropia. Am J Ophthalmol. 1966;62:1419.
Parks MM. The monofixation syndrome. Trans Am Ophthalmol Soc. 1969;67:609.
FIGURE 9-2. Congenital (infantile) esotropia. (From Nelson LB, Olitsky SE. A Color Handbook of Pediatric Clinical Ophthalmology. London: Manson Publishing, 2011.)

FIGURE 9-3. Sensory esotropia secondary to a congenital cataract in the right eye.

INFERIOR OBLIQUE OVERACTION
Epidemiology and Etiology
 Inferior oblique overaction occurs in a primary and secondary form. Most patients with primary IOOA have history of congenital esotropia, but it may occur in association with other forms of strabismus as well. Up to 80% of patients with a history of congenital esotropia may develop IOOA. Secondary IOOA occurs in patients with superior oblique palsy.
Inferior oblique overaction occurs in a primary and secondary form. Most patients with primary IOOA have history of congenital esotropia, but it may occur in association with other forms of strabismus as well. Up to 80% of patients with a history of congenital esotropia may develop IOOA. Secondary IOOA occurs in patients with superior oblique palsy.
Signs and Symptoms
 IOOA results in elevation of the involved eye as it moves nasally (Fig. 9-4).
IOOA results in elevation of the involved eye as it moves nasally (Fig. 9-4).
Differential Diagnosis
 DVD
DVD
 Duane’s syndrome with upshoot
Duane’s syndrome with upshoot
Diagnostic Evaluation
 The amount of overaction is evaluated in the field of action of the inferior oblique muscle in question. IOOA can be classified as grades I to IV. Grade I represents 1 mm of higher elevation of the adducting eye in gaze up and to the side. Grade IV indicates 4 mm of higher elevation. These differences in elevation between the two eyes are measured from the 6 o’clock position on each limbus. A measurement of the degree of adduction that is required to elicit the overaction is also helpful when considering treatment.
The amount of overaction is evaluated in the field of action of the inferior oblique muscle in question. IOOA can be classified as grades I to IV. Grade I represents 1 mm of higher elevation of the adducting eye in gaze up and to the side. Grade IV indicates 4 mm of higher elevation. These differences in elevation between the two eyes are measured from the 6 o’clock position on each limbus. A measurement of the degree of adduction that is required to elicit the overaction is also helpful when considering treatment.
Treatment
 IOOA can be treated surgically. The thresholds for surgery for IOOA are different, depending on whether weakening the inferior oblique is the only surgery being contemplated or whether weakening the inferior oblique in conjunction with horizontal strabismus surgery is being considered. If the inferior obliques alone are weakened, there should be a significant overaction present to justify surgery. If horizontal surgery is being performed, smaller grades of inferior oblique overaction may be corrected at the same time. Inferior oblique recession, myotomy, myectomy or denervation and extirpation can be performed to weaken the action of the inferior oblique.
IOOA can be treated surgically. The thresholds for surgery for IOOA are different, depending on whether weakening the inferior oblique is the only surgery being contemplated or whether weakening the inferior oblique in conjunction with horizontal strabismus surgery is being considered. If the inferior obliques alone are weakened, there should be a significant overaction present to justify surgery. If horizontal surgery is being performed, smaller grades of inferior oblique overaction may be corrected at the same time. Inferior oblique recession, myotomy, myectomy or denervation and extirpation can be performed to weaken the action of the inferior oblique.
 Anterior transposition of the inferior oblique can also be performed to limit the elevation of the eye and may be the treatment of choice when both IOOA and DVD occur together.
Anterior transposition of the inferior oblique can also be performed to limit the elevation of the eye and may be the treatment of choice when both IOOA and DVD occur together.
Prognosis
 Surgery is generally successful at improving the overacting inferior oblique muscle. Care must be taken to not miss any fibers of the muscle at the time of surgery.
Surgery is generally successful at improving the overacting inferior oblique muscle. Care must be taken to not miss any fibers of the muscle at the time of surgery.
REFERENCE
Parks MM. A study of the weakening surgical procedure for eliminating overaction of the inferior oblique. Am J Ophthalmol. 1972;73:107.
FIGURE 9-4. Inferior oblique overaction in both eyes. Note the elevation of each eye in adduction.

DISSOCIATED VERTICAL DEVIATION
Epidemiology and Etiology
 Most patients with DVD have history of congenital esotropia, but it may occur in association with other forms of strabismus as well.
Most patients with DVD have history of congenital esotropia, but it may occur in association with other forms of strabismus as well.
 Up to 90% of patients with a history of congenital esotropia may develop DVD.
Up to 90% of patients with a history of congenital esotropia may develop DVD.
 DVD appears to be a time-related phenomenon and is not related to successful initial surgery or the development of binocular vision.
DVD appears to be a time-related phenomenon and is not related to successful initial surgery or the development of binocular vision.
Signs and Symptoms
 DVD consists of a slow upward deviation of one or alternate eyes (Fig. 9-5). Excyclotorsion can often be demonstrated on upward drifting of the eye and incyclotorsion on downward motion.
DVD consists of a slow upward deviation of one or alternate eyes (Fig. 9-5). Excyclotorsion can often be demonstrated on upward drifting of the eye and incyclotorsion on downward motion.
 DVD may be latent, detected only when the involved eye is covered, or manifest, occurring intermittently or constantly. It can be differentiated from a true vertical deviation because no corresponding hypotropia occurs in the other eye on cover testing.
DVD may be latent, detected only when the involved eye is covered, or manifest, occurring intermittently or constantly. It can be differentiated from a true vertical deviation because no corresponding hypotropia occurs in the other eye on cover testing.
Differential Diagnosis
 Inferior oblique overaction
Inferior oblique overaction
 Hypertropia
Hypertropia
Diagnostic Evaluation
 DVD can be estimated by using the Hirschberg and Krimsky methods or the prism-cover test. A base-down prism is placed over the involved eye. The strength of the prism is adjusted until no movement occurs as the cover is shifted from the involved to the fixating eye. Because prism-cover measurement is difficult and may be inaccurate, DVD can also be estimated using a semiquantitative grading scale (1 to 4+).
DVD can be estimated by using the Hirschberg and Krimsky methods or the prism-cover test. A base-down prism is placed over the involved eye. The strength of the prism is adjusted until no movement occurs as the cover is shifted from the involved to the fixating eye. Because prism-cover measurement is difficult and may be inaccurate, DVD can also be estimated using a semiquantitative grading scale (1 to 4+).
Treatment
 If amblyopia exists, improvement in vision may improve fusional control and decrease how frequently the deviation is manifest.
If amblyopia exists, improvement in vision may improve fusional control and decrease how frequently the deviation is manifest.
 If DVD is entirely latent, detected on cover testing only, surgery is not indicated. If it is intermittent, surgery is determined by the size and frequency of the deviation as well as the patient’s concern regarding it’s appearance. Surgical treatment for DVD includes recession of the superior rectus and recession of the superior rectus combined with a posterior fixation suture and anterior transposition of the inferior oblique (preferred if IOOA coexists).
If DVD is entirely latent, detected on cover testing only, surgery is not indicated. If it is intermittent, surgery is determined by the size and frequency of the deviation as well as the patient’s concern regarding it’s appearance. Surgical treatment for DVD includes recession of the superior rectus and recession of the superior rectus combined with a posterior fixation suture and anterior transposition of the inferior oblique (preferred if IOOA coexists).
Prognosis
 It is often not possible to completely eliminate DVD. The goal of treatment is to reduce the magnitude of the deviation enough that it is not noticeable when it is manifest.
It is often not possible to completely eliminate DVD. The goal of treatment is to reduce the magnitude of the deviation enough that it is not noticeable when it is manifest.
REFERENCES
Bacal DA, Nelson LB. Anterior transposition of the inferior oblique muscle for both dissociated vertical deviation and/or inferior oblique overaction: results of 94 procedures in 55 patients. Binocular Vision Eye Muscle Surg. 1992;7:219.
Mims JL, Wood RC. Bilateral anterior transposition of the inferior obliques. Arch Ophthalmol. 1989;107:41.
FIGURE 9-5. Dissociated vertical deviation. A. Right eye occluded. B. Dissociated vertical deviation manifest after occlusion. (Courtesy of Alex Levin, MD.)
REFRACTIVE ACCOMMODATIVE ESOTROPIA
Epidemiology and Etiology
 The mechanism of refractive accommodative esotropia involves three factors: uncorrected hyperopia, accommodative convergence, and insufficient fusional divergence. When an individual exerts a given amount of accommodation, a specific amount of convergence (accommodative convergence) is associated with it. An uncorrected hyperope must exert excessive accommodation to clear a blurred retinal image. This in turn stimulates excessive convergence. If the amplitude of fusional divergence is sufficient to correct the excess convergence, no esotropia will result. However, if the fusional divergence amplitudes are inadequate or motor fusion is altered by some sensory obstacle, an esotropia will result.
The mechanism of refractive accommodative esotropia involves three factors: uncorrected hyperopia, accommodative convergence, and insufficient fusional divergence. When an individual exerts a given amount of accommodation, a specific amount of convergence (accommodative convergence) is associated with it. An uncorrected hyperope must exert excessive accommodation to clear a blurred retinal image. This in turn stimulates excessive convergence. If the amplitude of fusional divergence is sufficient to correct the excess convergence, no esotropia will result. However, if the fusional divergence amplitudes are inadequate or motor fusion is altered by some sensory obstacle, an esotropia will result.
Signs and Symptoms
 Refractive accommodative esotropia usually occurs in a child between 2 and 3 years of age with a history of acquired intermittent or constant esotropia. Occasionally, children who are 1 year of age or younger present with accommodative esotropia.
Refractive accommodative esotropia usually occurs in a child between 2 and 3 years of age with a history of acquired intermittent or constant esotropia. Occasionally, children who are 1 year of age or younger present with accommodative esotropia.
 The refraction of patients with refractive accommodative esotropia averages +4.75 diopters. The angle of esodeviation is the same when measured at distance and near fixation and is usually moderate in magnitude, ranging between 20 and 40 prism diopters. Amblyopia is common, especially when the esodeviation has become more nearly constant.
The refraction of patients with refractive accommodative esotropia averages +4.75 diopters. The angle of esodeviation is the same when measured at distance and near fixation and is usually moderate in magnitude, ranging between 20 and 40 prism diopters. Amblyopia is common, especially when the esodeviation has become more nearly constant.
Differential Diagnosis
 Congenital esotropia
Congenital esotropia
 Nonaccommodative esotropia
Nonaccommodative esotropia
 Nonrefractive accommodative esotropia
Nonrefractive accommodative esotropia
Diagnostic Evaluation
 A complete examination should be performed, including a cycloplegic refraction.
A complete examination should be performed, including a cycloplegic refraction.
Treatment
 The full hyperopic correction, determined by cycloplegic refraction, should be prescribed.
The full hyperopic correction, determined by cycloplegic refraction, should be prescribed.
Prognosis
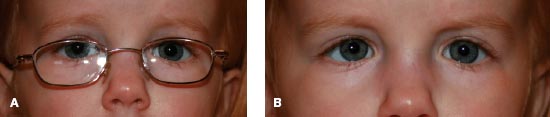
 Most children will maintain straight eyes while wearing their glasses (Fig. 9-6). Some children may show an increase in their hyperopia, which can lead to a recurrent crossing. A nonaccommodative esotropia may develop in a small percentage of children. Patients with relatively smaller levels of hyperopia may eventually outgrow their need for glasses as their hyperopic refractive error lessens with age.
Most children will maintain straight eyes while wearing their glasses (Fig. 9-6). Some children may show an increase in their hyperopia, which can lead to a recurrent crossing. A nonaccommodative esotropia may develop in a small percentage of children. Patients with relatively smaller levels of hyperopia may eventually outgrow their need for glasses as their hyperopic refractive error lessens with age.
REFERENCES
Coats DK, Avilla CW, Paysse EA, et al. Early-onset refractive accommodative esotropia. J AAPOS. 1998; 2:275–278.
Raab EL. Etiologic factors in accommodative esodeviation. Trans Am Ophthalmol Soc. 1982;80:657.
FIGURE 9-6. Refractive accommodative esotropia. A. With the appropriate hyperopic glasses the eyes are straight. B. Without glasses there is an esotropia of 25 prism diopters.
NONREFRACTIVE ACCOMMODATIVE ESOTROPIA
Epidemiology and Etiology
 Children with nonrefractive accommodative esotropia usually present between 2 and 3 years of age with an esodeviation that is greater at near than at distance fixation. The refractive error in this condition may be hyperopic or myopic, although the average refraction is +2.25 diopters.
Children with nonrefractive accommodative esotropia usually present between 2 and 3 years of age with an esodeviation that is greater at near than at distance fixation. The refractive error in this condition may be hyperopic or myopic, although the average refraction is +2.25 diopters.
 In nonrefractive accommodative esotropia, there is a high accommodative convergence to accommodation (AC:A) ratio: The effort to accommodate elicits an abnormally high accommodative convergence response.
In nonrefractive accommodative esotropia, there is a high accommodative convergence to accommodation (AC:A) ratio: The effort to accommodate elicits an abnormally high accommodative convergence response.
Signs and Symptoms
 Some parents notice the crossing that only takes place at near fixation.
Some parents notice the crossing that only takes place at near fixation.
 There are a number of ways of measuring the AC:A ratio. Most clinicians prefer to assess the ratio using the distance–near comparison. The AC:A relationship is derived by simply comparing the distance and near deviation. If the near measurement in a patient with esotropia is greater than 10 prism diopters, the AC:A ratio is considered to be abnormally high.
There are a number of ways of measuring the AC:A ratio. Most clinicians prefer to assess the ratio using the distance–near comparison. The AC:A relationship is derived by simply comparing the distance and near deviation. If the near measurement in a patient with esotropia is greater than 10 prism diopters, the AC:A ratio is considered to be abnormally high.
Differential Diagnosis
 Refractive accommodative esotropia
Refractive accommodative esotropia
Diagnostic Evaluation
 A complete examination, including a measurement of the esotropia at both distance and near fixation as well as a cycloplegic refraction, should be performed.
A complete examination, including a measurement of the esotropia at both distance and near fixation as well as a cycloplegic refraction, should be performed.
Treatment
 Treatment often uses the use of bifocal lenses to eliminate the accommodative effort required for near work. The bifocal is usually prescribed as an executive type lens that bisects the pupil.
Treatment often uses the use of bifocal lenses to eliminate the accommodative effort required for near work. The bifocal is usually prescribed as an executive type lens that bisects the pupil.
 Other treatment options include miotics and strabismus surgery. Some patients may be followed because those with good alignment at distance usually develop normal vision.
Other treatment options include miotics and strabismus surgery. Some patients may be followed because those with good alignment at distance usually develop normal vision.
Prognosis
 Many patients show a normalization of their AC:A ratio over time.
Many patients show a normalization of their AC:A ratio over time.
 Some patients decompensate and develop a nonaccommodative component that may require surgery. The risk of decompensation appears to be related to the magnitude of the distance–near disparity of the crossing.
Some patients decompensate and develop a nonaccommodative component that may require surgery. The risk of decompensation appears to be related to the magnitude of the distance–near disparity of the crossing.
REFERENCES
Kushner BJ. Fifteen-year outcome of surgery for the near angle in patients with accommodative esotropia and a high accommodative convergence to accommodation ratio. Arch Ophthalmol. 2001;119:1150–1153.
Ludwig IH, Parks MM, Getson PR. Long-term results of bifocal therapy for accommodative esotropia. J Pediatr Ophthalmol Strabismus. 1989;26:264.
O’Hara MA, Calhoun JH. Surgical correction of excess esotropia at near. J Pediatr Ophthalmol Strabismus. 1990;27:120.
Pratt-Johnson JA, Tillson G. The management of esotropia with high AC/A ratio (convergence excess). J Pediatr Ophthalmol Strabismus. 1985;22:238.
NONACCOMMODATIVE OR PARTIALLY ACCOMMODATIVE ESOTROPIA
Epidemiology and Etiology
 Refractive or nonrefractive accommodative esotropias do not always occur in their “pure” forms. Some patients may show no response to correction of their hyperopia. Other patients may have a significant reduction in esodeviation when given glasses, but a residual esodeviation persists despite full hyperopic correction. Still others may show an initial good response only to develop a crossing that can no longer be completely corrected with glasses. The crossing not corrected with the glasses is the nonaccommodative portion. This condition commonly occurs when there is a delay of months between the onset of accommodative esotropia and antiaccommodative treatment.
Refractive or nonrefractive accommodative esotropias do not always occur in their “pure” forms. Some patients may show no response to correction of their hyperopia. Other patients may have a significant reduction in esodeviation when given glasses, but a residual esodeviation persists despite full hyperopic correction. Still others may show an initial good response only to develop a crossing that can no longer be completely corrected with glasses. The crossing not corrected with the glasses is the nonaccommodative portion. This condition commonly occurs when there is a delay of months between the onset of accommodative esotropia and antiaccommodative treatment.
Signs and Symptoms
 Patients with nonaccommodative esotropia have little or no hyperopia. They may also have a level of hyperopia that does not appear compatible with the degree of crossing.
Patients with nonaccommodative esotropia have little or no hyperopia. They may also have a level of hyperopia that does not appear compatible with the degree of crossing.
 Patients with a partial accommodative esotropia appear to have a level of hyperopia that will correct their crossing. However, they do not demonstrate a resolution of their crossing when wearing their glasses.
Patients with a partial accommodative esotropia appear to have a level of hyperopia that will correct their crossing. However, they do not demonstrate a resolution of their crossing when wearing their glasses.
Differential Diagnosis
 Congenital esotropia
Congenital esotropia
 Accommodative esotropia
Accommodative esotropia
Diagnostic Evaluation
 A complete examination with cycloplegic refraction should be performed. If a significant level of hyperopia exists, the patient should be prescribed the full hyperopic correction and return after wearing glasses for a period of time.
A complete examination with cycloplegic refraction should be performed. If a significant level of hyperopia exists, the patient should be prescribed the full hyperopic correction and return after wearing glasses for a period of time.
Treatment
 If the nonaccommodative component of the crossing is large enough to prevent the development of binocular vision, strabismus surgery should be considered. Some surgeons will not opt for surgery if the crossing is small and not easily noticed.
If the nonaccommodative component of the crossing is large enough to prevent the development of binocular vision, strabismus surgery should be considered. Some surgeons will not opt for surgery if the crossing is small and not easily noticed.
Prognosis
 Patients with small levels of hyperopia may be able to discontinue wearing their glasses. Recurrent strabismus is possible in these patients, who often have abnormal binocular vision even after successful treatment.
Patients with small levels of hyperopia may be able to discontinue wearing their glasses. Recurrent strabismus is possible in these patients, who often have abnormal binocular vision even after successful treatment.
CONGENITAL EXOTROPIA
Epidemiology and Etiology
 Congenital exotropia behaves in a very similar fashion to congenital esotropia. It typically occurs early in life and presents with a large, constant out-turning. Congenital exotropia may be associated with neurologic disease or abnormalities of the bony orbit, as in Crouzon’s syndrome.
Congenital exotropia behaves in a very similar fashion to congenital esotropia. It typically occurs early in life and presents with a large, constant out-turning. Congenital exotropia may be associated with neurologic disease or abnormalities of the bony orbit, as in Crouzon’s syndrome.
Signs and Symptoms
 Patients with congenital exotropia often appear to have decreased adduction on side gaze; with gaze right or left, the abducting eye fixates while the opposite eye approaches midline and stops. This is similar to the cross fixation found in children with congenital esotropia. Occlusion or the doll’s head maneuver will demonstrate that good adduction is possible.
Patients with congenital exotropia often appear to have decreased adduction on side gaze; with gaze right or left, the abducting eye fixates while the opposite eye approaches midline and stops. This is similar to the cross fixation found in children with congenital esotropia. Occlusion or the doll’s head maneuver will demonstrate that good adduction is possible.
 Amblyopia is not common because these children typically alternate fixation. The refractive error is similar to that of the general population.
Amblyopia is not common because these children typically alternate fixation. The refractive error is similar to that of the general population.
Differential Diagnosis
 Early-onset intermittent exotropia
Early-onset intermittent exotropia
 Third cranial nerve palsy
Third cranial nerve palsy
 Bilateral intranuclear ophthalmoplegia
Bilateral intranuclear ophthalmoplegia
Diagnostic Evaluation
 A complete examination should be performed.
A complete examination should be performed.
 Other signs of a cranial nerve palsy (ptosis, decreased motility) should be eliminated.
Other signs of a cranial nerve palsy (ptosis, decreased motility) should be eliminated.
Treatment
 Patients with congenital constant exotropia are operated on early in life in the same manner as patients with congenital esotropia.
Patients with congenital constant exotropia are operated on early in life in the same manner as patients with congenital esotropia.
Prognosis
 Similar to patients with congenital esotropia, early surgery in these patients can lead to gross binocular vision but not bifoveal fixation.
Similar to patients with congenital esotropia, early surgery in these patients can lead to gross binocular vision but not bifoveal fixation.
 These patients also tend to develop DVD and IOOA and should be followed closely for the development of these associated motility disturbances.
These patients also tend to develop DVD and IOOA and should be followed closely for the development of these associated motility disturbances.
REFERENCE
Hunter DG, Kelly JB, Buffenn AN, et al. Long-term outcome of uncomplicated infantile exotropia. J AAPOS. 2001;5:352–356.
INTERMITTENT EXOTROPIA
Epidemiology and Etiology
 Intermittent exotropia is the most common exodeviation in childhood.
Intermittent exotropia is the most common exodeviation in childhood.
 The etiology of intermittent exotropia is unknown but probably results from a combination of mechanical and innervational factors.
The etiology of intermittent exotropia is unknown but probably results from a combination of mechanical and innervational factors.
Signs and Symptoms
 The age of onset of intermittent exotropia varies but is often between age 6 months and 4 years.
The age of onset of intermittent exotropia varies but is often between age 6 months and 4 years.
 It is characterized by outward drifting of one eye, which usually occurs when a child is fixating at distance (Fig. 9-7). The deviation is generally more frequent with fatigue or illness. Exposure to bright light may cause reflex closure of the exotropic eye.
It is characterized by outward drifting of one eye, which usually occurs when a child is fixating at distance (Fig. 9-7). The deviation is generally more frequent with fatigue or illness. Exposure to bright light may cause reflex closure of the exotropic eye.
 Because the deviation generally begins with distance fixation and is only seen when the child is tired, it is often not seen when the child is examined by a primary medical doctor at close distance or during a well-child visit.
Because the deviation generally begins with distance fixation and is only seen when the child is tired, it is often not seen when the child is examined by a primary medical doctor at close distance or during a well-child visit.
Differential Diagnosis
 Congenital exotropia
Congenital exotropia
Diagnostic Evaluation
 A complete evaluation should be performed. Motility measurements at both distance and near fixation should be completed. A qualitative measurement of the control of the strabismus should be noted.
A complete evaluation should be performed. Motility measurements at both distance and near fixation should be completed. A qualitative measurement of the control of the strabismus should be noted.
Treatment
 Any coexistent amblyopia should be treated. Significant refractive errors should be corrected. Some ophthalmologists use medical treatments to avoid surgery in some patients. These nonsurgical treatments include part-time occlusion, orthoptic therapy, and over minus lens therapy. Most patients eventually require strabismus surgery when the deviation becomes manifest frequently.
Any coexistent amblyopia should be treated. Significant refractive errors should be corrected. Some ophthalmologists use medical treatments to avoid surgery in some patients. These nonsurgical treatments include part-time occlusion, orthoptic therapy, and over minus lens therapy. Most patients eventually require strabismus surgery when the deviation becomes manifest frequently.
Prognosis
 Surgery is successful in aligning most patients’ eyes. Some patients will redevelop strabismus and may require more surgery.
Surgery is successful in aligning most patients’ eyes. Some patients will redevelop strabismus and may require more surgery.
REFERENCE
Kushner BJ. Exotropic deviations: a functional classification and approach to treatment. Am Orthoptic J. 1988;38:81–93.
FIGURE 9-7. Intermittent exotropia demonstrating manifest exotropia at distance fixation.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


