Soft Lens Problem Solving
J. Bart Campbell
Vinita Allee Henry
John W. Marohn
Two significant developments in the field of soft lenses have enormously enhanced the clinician’s available tools for soft lens problem solving: the development of modern disposable lenses and the development of silicone hydrogel lenses. During the 1990s, disposable contact lenses rapidly became the modality of choice for most wearers being fitted for the first time or being refitted with hydrogel lenses. This resulted in changes in the way contact lenses are perceived and cared for by the public, and in the way practitioners manage fittings and many complications.
However, most disposable contact lenses are manufactured with the same hydrogel materials initially used for conventional replacement lenses. Consequently, there is no inherent difference in the interaction between the eye and the lens. That said, hydrogel disposable contact lenses do provide substantial benefits in managing deposition-related complications. In fact, such complications should be eliminated when disposable lenses are used properly.
Disposable lenses have also encouraged manufacturers to develop a generation of care systems that emphasize convenience through the utilization of multipurpose solutions. Although these systems should enhance compliance, they may not accomplish the task of disinfection and cleaning when patients do not follow instructions.1,2
The emergence of silicone hydrogel lenses in the late 1990s addressed a major problem not solved by the initial generation of hydrogel disposable lenses: oxygen transmissibility (Dk/t). Lenses manufactured from silicone hydrogel materials have vastly improved Dk/t values compared to conventional hydrogel materials. This characteristic, combined with the existing disposable modality, has enabled the clinician to address two of the biggest causes of soft lens problems: lens deposition and corneal hypoxia. However, patient compliance remains a key issue in avoiding complications. This fact, combined with a demand for 30-day continuous wear (CW) of silicone hydrogel lenses, has resulted in the conclusion that even these lenses are not without complications.3
It must also be noted that there are still conventional replacement contact lens wearers in existence. Patients who have extremely high refractive errors, high amounts of astigmatism, and other special conditions often have not been fitted in disposable lenses because there are fewer lenses available in the required parameters. These patients, as well as the wearers of disposable lenses who do not replace their lenses or who experience non-deposition-related complications, continue to provide the practitioner with ample justification to be concerned with soft lens problem solving.
▪ TERMINOLOGY
Most lenses that practitioners refer to as “disposable” do not actually meet the criteria for disposable lenses that have been defined by the Food and Drug Administration (FDA). To meet the FDA criteria, a device must be used only once and then discarded. Only the so-called “1-day” or “daily disposable” lenses are routinely used in this fashion. Typically, practitioners prescribe “disposable” lenses to be replaced every 7 to 14 days. Further complicating the terminology issue are lenses prescribed as “planned-replacement,” “frequent-replacement,” or
“programmed-replacement” lenses. In this replacement schedule, the lenses are usually replaced every 1 to 3 months.
“programmed-replacement” lenses. In this replacement schedule, the lenses are usually replaced every 1 to 3 months.
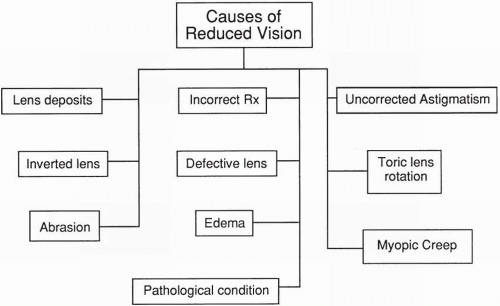 ▪ FIGURE 13.1 Summary of causes of reduced vision. |
▪ SYMPTOMS
Reduced Vision
Visual reduction as a result of contact lens wear may be attributed to a number of causes (Fig. 13.1). A problem-oriented case history is often invaluable in disclosing the factor(s) instrumental in contact lens-induced reduction of visual acuity. The clinician should determine onset and duration, and whether the reduced visual acuity is present when spectacles are worn. Reasons for contact lens-related visual acuity reduction may include lens contamination, uncorrected refractive error, defective lens material, improper lens-to-cornea fitting relationship, and excessive tearing. The use of pinhole visual acuity measurement may assist in determining if the cause of decreased visual acuity is uncorrected refractive error. Visual acuity reduction, noted with both contact lens and spectacle correction, may be attributed to corneal abnormalities, including edema, abrasions, punctate keratitis, and infectious keratitis. The presence of intraocular abnormalities as a source of visual acuity reduction must also be recognized, and all contact lens wearers should undergo regularly scheduled comprehensive visual examinations.
Lens Deposits
Surface deposits are most often attributed to inadequate lens hygiene. A mucoproteinaceous film, primarily composed of lysozyme, is frequently the major factor in causing reduced vision.4 Complaints of “foggy” or “hazy” vision with distortion, especially when bright lights are viewed, are often expressed by affected patients. This symptom will not be noted after the lens is removed. If it is, the possibility of corneal edema must be considered. Lipid deposits and calcium-lipid complexes (e.g., “jelly bumps”), in addition to other organic and inorganic debris, may cause visual reduction, but their principal effect is on lens comfort.5 Diagnosis is achieved by examining the lens in vivo with the biomicroscope; excessive deposition may be noted without the use of magnification.
Treatment of lens deposition often depends on the type of deposit. Protein coatings, if observed before extensive accumulation is present, may be removed with enzymatic cleaning
because of their superficial nature. If the lens is moderately coated, a series of two to three successive enzymatic cleanings may be necessary to remove the protein adequately; a weekly enzymatic cleaning should be sufficient for most patients. Utilization of a daily protein remover, either one incorporated into a multipurpose solution or a separate solution like SupraClens (Alcon Laboratories), may be helpful. Rubbing of the lens following enzyme soaking with either saline solution or cleaner, in addition to the recommended daily cleaning, may be beneficial in removing any remaining protein. The presence of jelly bumps on the lens surface necessitates replacement of the lens because of their penetrating nature into the lens matrix. Removal of the jelly bumps results in subsequent holes or pits, rendering the lens inadequate for continued wear. Nevertheless, the current practice is to refit the patient in disposable contact lenses if possible. This precludes the need for “heroic” measures to save a contaminated lens.
because of their superficial nature. If the lens is moderately coated, a series of two to three successive enzymatic cleanings may be necessary to remove the protein adequately; a weekly enzymatic cleaning should be sufficient for most patients. Utilization of a daily protein remover, either one incorporated into a multipurpose solution or a separate solution like SupraClens (Alcon Laboratories), may be helpful. Rubbing of the lens following enzyme soaking with either saline solution or cleaner, in addition to the recommended daily cleaning, may be beneficial in removing any remaining protein. The presence of jelly bumps on the lens surface necessitates replacement of the lens because of their penetrating nature into the lens matrix. Removal of the jelly bumps results in subsequent holes or pits, rendering the lens inadequate for continued wear. Nevertheless, the current practice is to refit the patient in disposable contact lenses if possible. This precludes the need for “heroic” measures to save a contaminated lens.
Incorrect Prescription
Reduction in Snellen visual acuity will be observed if the patient is wearing an incorrect lens prescription. Verification of soft lens power is difficult to perform because of the nature of the material but may be necessary if inadequate visual acuity is noted. If possible, it is desirable to evaluate new lenses on the patient’s eyes at the time of dispensing. This can easily detect incorrect prescriptions, visible lens defects, and uncomfortable lenses. Unfortunately, such evaluations may not be possible in every case and are never possible with every disposable lens. In these situations, patients must be thoroughly educated to be aware of symptoms that indicate defective lenses and to discontinue wear of the affected lens. In addition to manufacturer error, the possibility of such problems as lens reversal by the patient or practitioner or an incorrect refraction must be considered. An expedient method of determining whether the reduction in visual acuity is refractive or possibly pathologic in nature is a pinhole visual acuity measurement. An overrefraction is also definitive in indicating whether the patient is wearing an incorrect prescription or whether the lenses may be switched. If the difference in the refractive error between the two eyes is relatively equal, the patient may not notice that the lenses are switched. New lenses must be ordered with the correct prescription or, if switched, each lens should be placed in the appropriate eye.
Uncorrected Refractive Astigmatism
Another source of reduced visual acuity in soft lens wearers is uncorrected refractive astigmatism. The inherent flexibility of these lenses limits their ability to correct effectively for astigmatism generated by the corneal surface. Approximately 16% of the refractive astigmatism is compensated for by the lens-cornea interface, reflecting the inability of the soft lens to conform totally to the corneal surface.6 Patients with 0.75 D to 1.00 D of refractive astigmatism may begin to experience symptoms of decreased visual acuity while wearing spherical soft lenses.7 Some aspheric soft contact lens designs have been found to provide good vision in patients with small amounts of astigmatism (i.e., 0.50-1.00 D). Aspheric soft contact lens designs do not correct astigmatism, but enhance the optics by reducing the spherical aberration; thus, the patient may perceive enhanced vision.8,9 The ability to tolerate small amounts of blur depends primarily on the visual awareness and activities performed by the contact lens wearer. Persons who perform extensive near tasks involving small detail may require a toric lens correction. Overrefraction with placement of the appropriate cylinder in the phoropter will improve visual acuity, allowing the patient to determine the acceptability of the compromised vision. Astigmatic correction may be obtained with the use of either a soft toric or rigid gas-permeable (GP) contact lens.
Toric Lens Rotation
Soft toric lens rotation, either subsequent to each blink or as a result of persistent mislocation, is a principal cause of reduced visual acuity in astigmatic patients. Patients who exhibit astigmatism on an oblique axis are more prone to lens rotation than are those exhibiting with-the-rule
and against-the-rule astigmatism. An oblique cross-cylinder effect, generated as a result of misalignment between the refractive cylinder axis and the toric lens, results in disturbances in visual acuity. Near tasks may be compromised by toric lens rotation with eye convergence, resulting from encyclo-rotation of the globe. A nasal and upward rotation of soft lenses has been noted and may need to be compensated for in axis selection, especially for presbyopic and esotropic patients.7 This problem is even more pronounced for presbyopic patients wearing toric contact lenses with one eye corrected for distance vision and the other corrected for near vision (i.e., monovision). Slit-lamp examination of the toric lens will determine whether the lens is stable with adequate centration and movement or whether excessive “rocking” occurs after each blink. Refraction performed over the patient’s current contact lenses or diagnostic lenses may be beneficial in determining the appropriate power and axis to order for the patient. This is especially apparent in persons with refractive astigmatism >3.00 D, in whom small amounts of rotation that can have a significant impact on visual acuity may be difficult to assess.10 Excessive lens movement may require a steeper base curve to reduce rotation and improve visual acuity. Changing to a different design (e.g., slab off, thin zone designs) may also be beneficial. The option of refitting into spherical GP lenses may also be considered in a challenging case, especially when corneal toricity accounts for most of the patient’s refractive astigmatism.
and against-the-rule astigmatism. An oblique cross-cylinder effect, generated as a result of misalignment between the refractive cylinder axis and the toric lens, results in disturbances in visual acuity. Near tasks may be compromised by toric lens rotation with eye convergence, resulting from encyclo-rotation of the globe. A nasal and upward rotation of soft lenses has been noted and may need to be compensated for in axis selection, especially for presbyopic and esotropic patients.7 This problem is even more pronounced for presbyopic patients wearing toric contact lenses with one eye corrected for distance vision and the other corrected for near vision (i.e., monovision). Slit-lamp examination of the toric lens will determine whether the lens is stable with adequate centration and movement or whether excessive “rocking” occurs after each blink. Refraction performed over the patient’s current contact lenses or diagnostic lenses may be beneficial in determining the appropriate power and axis to order for the patient. This is especially apparent in persons with refractive astigmatism >3.00 D, in whom small amounts of rotation that can have a significant impact on visual acuity may be difficult to assess.10 Excessive lens movement may require a steeper base curve to reduce rotation and improve visual acuity. Changing to a different design (e.g., slab off, thin zone designs) may also be beneficial. The option of refitting into spherical GP lenses may also be considered in a challenging case, especially when corneal toricity accounts for most of the patient’s refractive astigmatism.
Defective Lenses
Characteristics of a defective lens include either abrasions (scratches, tears, nicks, holes) or poor optics. Both may contribute to irritation, discomfort, and reduced visual acuity. During initial wear, lenses with abrasions are the most common cause of lens replacement. Although the actual defect may not always cause reduced vision, deposit accumulation in the area of a scratch or tear may affect visual acuity. Poor lens manufacturing may result in inadequate optics, resulting in the need for lens exchange. Increased tearing and mucous production secondary to irritation of the palpebral conjunctiva from an elevated lens defect may also degrade vision. Biomicroscopy will elicit the source of the problem if a lens abrasion exists. Careful examination of the lens edge may be necessary to locate a nick or small tear, many of which may not be detected by the practitioner. The absence of improvement in visual acuity with an overrefraction may be indicative of poor optics, necessitating lens replacement. A small peripheral tear, if not irritating to the patient, may be clinically tolerable but will undoubtedly increase in size with continued lens manipulation. Lens replacement is undoubtedly the most effective method of handling defective lenses.
Patients may report discomfort or heightened lens awareness when there are no observable lens defects. If the symptoms are present in only one eye, briefly switching the lenses can determine if the discomfort follows the lens or remains in the initially affected eye. If it follows the lens, then the most expedient solution is simply to replace the lens. If the discomfort remains only in the initially affected eye, closer examination of the eye itself is warranted. Replacement of the lens may still be the only way to alleviate the patient’s concerns, even when no clinically observable cause for the discomfort is present.
Lens Inversion
A common complaint, especially with new soft lens wearers, is difficulty with lens inversion. Patients wearing thin lenses often exhibit frustration in determining whether the lens is properly oriented before insertion (i.e., “right side out”). Mild irritation may be observed as a result of increased movement of the lens. Examination of the lens edge with the biomicroscope will reveal standoff from the bulbar conjunctiva and excessive movement. Some lens manufacturers print their name or a symbol at the periphery of the lens to facilitate determining the presence of lens inversion. Familiarity with each design is essential, as there is no consistency between manufacturers. The “taco test” may assist patients in placing the lens correctly on the
eye (Chapter 12). Removal of the lens, accompanied by correct orientation, will resolve any decrease in visual acuity or irritation noted by the patient. Patients should be counseled that an inverted lens will not damage their eye and that if they are unsure whether the lens is inverted, it is acceptable simply to remove it and try wearing it with the other side toward the eye.
eye (Chapter 12). Removal of the lens, accompanied by correct orientation, will resolve any decrease in visual acuity or irritation noted by the patient. Patients should be counseled that an inverted lens will not damage their eye and that if they are unsure whether the lens is inverted, it is acceptable simply to remove it and try wearing it with the other side toward the eye.
Reduction of Visual Acuity with Contact Lenses and Spectacles
A reduction in visual acuity, apparent with both contact lens and spectacle correction, may be indicative of a more serious complication. Removal of the contact lenses and inspection of the cornea and conjunctiva are imperative in determining the cause of the decreased visual acuity. Some physiologic factors that may influence vision with soft contact lens wear include the following:
An abrasion secondary to insertion and removal, poor lens fit, surface defects, or a foreign body.
Edema related to the physical fit, water content, prescription, or lens deposition.
Central punctate staining secondary to poor lens fit, solution sensitivity, surface defects, inadequate wetting, poor tear exchange, or trapped debris.
Increased mucous production as a result of giant papillary conjunctivitis.
“Myopic creep” resulting from corneal edema.
Irregular astigmatism or corneal distortion secondary to keratoconus or other causes.
A pathologic condition affecting the anterior or posterior segment that is unrelated to contact lens wear.
Discomfort
When a soft contact lens wearer experiences discomfort, the lens should be removed immediately. If the discomfort persists, the patient should be educated to contact the practitioner immediately. A comprehensive case history will be very important in determining the cause of the pain (Fig. 13.2). A differential diagnosis is possible by classifying the discomfort into one of four categories. It is important to determine if the discomfort occurs on insertion or after lens removal and if the onset is immediate or delayed. Duration of the discomfort (e.g., transient, constant, or intermittent) should be determined. Further biomicroscopic evaluation of the cornea, both with lens wear and on removal, will aid in determination of the source of the discomfort. In addition, evaluation of corneal staining with fluorescein application is important.
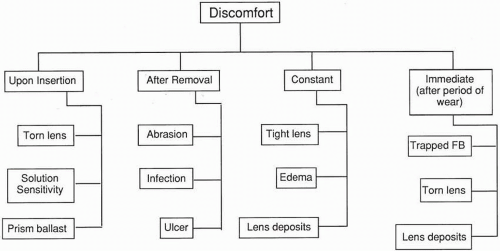 ▪ FIGURE 13.2 Summary of causes of discomfort. |
Discomfort on Lens Insertion
If discomfort occurs on insertion, the source is most likely either a torn lens, a sensitivity to the solutions used, or (if applicable) the prism ballast of a toric lens. A torn lens can be detected by carefully examining both the entire lens surface and the lens edge with the biomicroscope. The upper lid should be raised to evaluate the superior lens edge. Lens tears may be difficult to observe. The lens should be carefully observed on the blink, which will make the tear more evident. The tear may actually be a hole or nick in the lens or have the appearance of a scratch or adhered debris. Apparent trapped debris that cannot be cleaned off and remains on the lens with a blink is most likely a lens defect. A torn lens should be replaced immediately.
If a patient uses an improper solution in the eye or on the soft lens (i.e., hydrogen peroxide or a GP lens solution) or has acquired a sensitivity to the preservative in a solution, an immediate burning and stinging sensation will be experienced. Lens removal should improve the discomfort; however, a mild to moderate superficial punctate keratitis will remain; thus, mild discomfort and injection may still be present. By questioning the patient about the solutions used with the lenses and evaluating the cornea and conjunctiva with a biomicroscope, the practitioner will be able to determine if the source of the discomfort is preservative sensitivity. If the practitioner is still unsure, another care system can be prescribed for the patient. Replacing the lens with a fresh, sterile lens is optimal. If the discomfort is eliminated by a change in the solution system, sensitivity to the solution was most likely the cause. In severe cases, lens wear may have to be discontinued until the subjective discomfort has been alleviated. This may occur after a few hours or take up to several days.
A rare cause of discomfort is the prism ballast of a toric lens. Occasionally, a patient will complain of lens sensation caused by the thickness of the lens in the area of the prism ballast. If no other source of discomfort is found, a change in the type of toric lens design (i.e., use of eccentric lenticulation, thin zones) may alleviate the lens sensation.
Discomfort with a previously unworn lens versus discomfort with a worn but previously comfortable lens may be approached differently. If the lens is new and the patient experiences discomfort from a design that has previously been satisfactory, the cause may be debris trapped under the lens on insertion. Simply removing the lens and rinsing it may provide relief from the discomfort. If the discomfort persists and the cause is not visible, the lens itself may be defective in a way that is not visible with conventional inspection techniques. The most expedient course of action is to replace the lens. If the discomfort occurs with a lens that has been previously worn with no discomfort, the most likely cause is a torn lens. The lens should be removed and inspected. If no damage is found, the lens may be rinsed and inserted again to determine if the discomfort persists.
Discomfort after Lens Removal
When pain or discomfort is present after lens removal, the origin of the problem is typically the cornea. Pain that continues after lens removal is an ocular emergency, and the patient should be evaluated in the office as soon as possible. Corneal abrasions, ocular infections, corneal ulcers, or other ocular problems may be causing the pain. Fluorescein evaluation is important in determining the extent of the corneal disturbance. Discomfort and pain that remain after the removal of soft lenses should be taken seriously until a differential diagnosis is made.
Constant Discomfort during Lens Wear
When the discomfort of soft lenses is constant, the source of the discomfort may be a poorly fitting lens, corneal edema and edema-related symptoms (i.e., microcysts), or lens deposits. Biomicroscopy and fluorescein evaluation will aid in determination of the cause. A compression ring around the limbal area after lens removal is indicative of a tight lens. Higher-modulus silicone hydrogel lenses that are fitted too flat may exhibit edge lift and cause discomfort. After
alteration of the lens parameters, either by changing the base curve radius (BCR) or the lens diameter, the symptoms should disappear. For a patient experiencing edema-related symptoms, a change to a higher-Dk/t silicone hydrogel lens will be beneficial.
alteration of the lens parameters, either by changing the base curve radius (BCR) or the lens diameter, the symptoms should disappear. For a patient experiencing edema-related symptoms, a change to a higher-Dk/t silicone hydrogel lens will be beneficial.
Another cause of constant discomfort with a soft lens is a deposited lens. These deposits will be evident when the lens is viewed with the biomicroscope. The deposits may be a result of poor lens care, old lenses, or lenses that have been contaminated with substances such as hair spray or lotion. Silicone hydrogel lenses are more prone to lipid deposits than conventional hydrogel lenses. Despite the claims of “no rub” solutions, silicone hydrogel lenses should be rubbed upon removal to aid in the removal of lipid deposits. The authors recommend educating all soft lens patients to rub and rinse their lenses to provide the cleanest and most comfortable lenses. Replacing the deposited lens with a clean, new lens will alleviate the symptoms.
Sudden Discomfort after a Period of Lens Wear
Patients may experience sudden discomfort after the lens has been worn for several hours. The most frequent cause of sudden discomfort is a trapped foreign body, such as dust or cosmetic particles. Removing the lens and rinsing it with solution should eliminate this discomfort. A large foreign body may cause a corneal abrasion; therefore, if the pain continues, it is important for the patient to be evaluated in the office. A deposited lens, especially one with jelly bumps, or a contaminated lens may result in discomfort that increases as the period of lens wear increases. Finally, a torn lens may also cause immediate discomfort; however, typically the discomfort is noticed on lens insertion. Obviously, the treatment for a foreign body is its removal. If the lens is not damaged, deposited, or torn, the lens may be worn again. Conversely, a damaged lens will require replacement. In the case of a foreign body, the cornea, conjunctiva, and lids should be examined to make sure the foreign body has not become embedded.
Burning or Stinging Sensation
Burning and stinging are most often related to contact lens solution sensitivity. Reinforcement of appropriate lens hygiene at each visit is beneficial in maintaining patient compliance and avoiding unnecessary irritation. Irritation with continued use of a chemical disinfecting system may indicate a possible hypersensitivity or toxic reaction to the preservative and/or an added surfactant. Discomfort noted by patients is typically minimal because of the low concentration of preservatives in the solution. Often the complaint is a feeling of dryness, rather than burning. A generalized stippling is indicative of a toxic or hypersensitivity reaction, and, if severe enough, may elicit tearing and photophobia as well as decreased visual acuity. Patients who exhibit this problem may achieve success with the use of a preservative-free, hydrogen peroxide disinfecting system. Incomplete neutralization of hydrogen peroxide can result in the symptoms of burning and stinging; a low pH (4.0) after disinfection and the buffer system to control pH may also contribute to irritation. A typical scenario with systems that use a catalytic disc for neutralization is a gradually increasing burning sensation each morning on lens insertion. Although most patients no longer use a separate daily cleaner or enzyme cleaner with their soft lenses, the use of a daily cleaner before insertion or inadequate rinsing of the lens after cleaning may elicit a burning sensation. Any residual cleaner remaining on the lens after enzyme cleaning may also cause discomfort. A comprehensive case history may be extremely beneficial in determining the cause of the ocular irritation. Reviewing cleaning and disinfection procedures at each visit can assist in alleviating solutionrelated discomfort associated with the use of inappropriate technique. Instructions and diagrams may help in maintaining patient compliance with acceptable cleaning and disinfecting procedures. The emergence of multipurpose solutions may make it difficult to determine the offending component, as many of these products contain surfactants and other compounds in the disinfecting solution (Fig. 13.3).
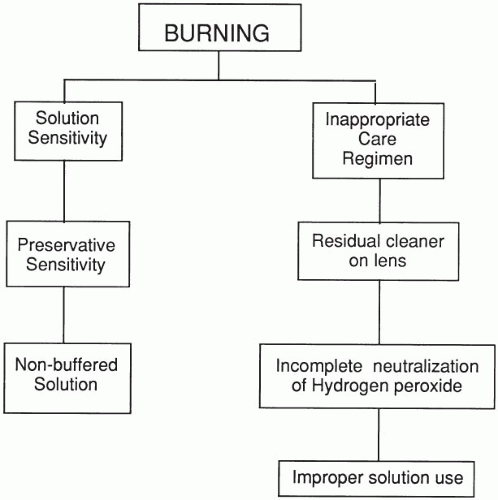 ▪ FIGURE 13.3 Summary of causes of burning. |
Photophobia
Definition
The term photophobia is often used loosely in describing irritation and discomfort as a result of contact lens wear. When the term is used appropriately, photophobia is typically considered a pathologic condition that occurs when light entering the eye causes pain. Photophobia may be contrasted with dazzle, a sensation of discomfort as a result of excessive light that is usually not associated with pain. A temporary sensation of dazzle is experienced with inadequate adaptation of the eye from dark to lighted conditions. Also, dazzle, unlike photophobia, is not accompanied by blepharospasm and lacrimation. Pathologic conditions affecting the anterior segment of the eye are often accompanied by photophobia. Typically, the more superficial the corneal defect, the more severe the photophobia because of the arrangement of the innervation of the epithelium.11 It is important to remember that photophobia is a symptom of an ocular problem and that the logical method to address this symptom is to determine and then treat the condition causing the photophobia.
Causes
Epithelial abrasions may be observed in contact lens wearers and, in severe cases, may induce photophobia. Superficial corneal abrasions may occur as a result of contact lens defects (including tears and nicks), moderate lens “overwear,” mild trauma, trapped debris, and an uneven surface. Often, superficial defects go unnoticed by the patient but may result in mild discomfort and irritation. Deeper abrasions typically result in more severe pain, including lacrimation, blepharospasm, and photophobia. Removal of the entire thickness of the epithelium occurs most commonly as a result of blunt trauma (e.g., hand, thumb, or ball in the eye), improper insertion or removal of the contact lens, or a foreign body under the lens.12
In addition to abrasions, photophobia has been attributed to other factors.5,11,13 Initial adaptation to contact lens wear may initiate photophobia, and this is considered normal unless the symptom continues longer than a few weeks. Uncorrected refractive error and residual astigmatism may also contribute to a photophobic response.11
Determining the Cause of Photophobia
A thorough case history may be extremely beneficial in eliciting the cause of photophobia. Biomicroscopic examination of both the contact lens and the cornea will eliminate any gross defects contributing to the symptoms. The presence of discharge, in conjunction with lacrimation and blepharospasm, may indicate the possibility of infection. The type of discharge (e.g., mucopurulent, watery, stringy) should be elicited in determining the possible etiology. Fluorescein staining is beneficial in determining the presence, location, and depth of an abrasion. The configuration of the staining pattern may allude to a causative factor (e.g., tear, nick, foreign body, deposited lens). Examination of the lens under magnification may further assist in locating any lens defects.
Treatment of the Causes of Photophobia
Conservative treatment of superficial abrasions includes contact lens removal to ensure proper healing. Epithelial cell coverage of the abrasion usually is complete within 24 hours. Although antibiotic therapy is typically not warranted, consideration may be necessary in patients exhibiting poor lid hygiene, coated lenses, or poor compliance. Deeper corneal abrasions require more aggressive therapy, including lens removal and antibiotic use if the threat of infection is present; however, preservatives found in medications may slow down the healing process.12
Infections require discontinuation of contact lens wear and appropriate antibiotic treatment (Chapter 21). Microbial keratitis (MK) is a serious infection found primarily in overnight wear of contact lenses. More information on MK is provided in Chapter 16. Lens wear should not be resumed until the clinician is comfortable that the infection has resolved.
Dryness
Dry-eye symptoms are very common among hydrogel lens wearers.14,15,16,17 These symptoms may be a result of the patient’s poor tear quality or quantity or the effect of the contact lens itself on the tear film.18 Historically, the tear film was described as composed of three layers: aqueous, lipid, and mucin. More recent theories have described the tear film as a gel-like structure with several layers derived from these components.19 If a deficit occurs in any component, contact lens wear may be affected. A complete blink approximately every 5 seconds is required to spread the tear film over the cornea. Incomplete or partial blinks will result in dryness of the inferior region of the cornea. Blinking exercises may alleviate dryness in these cases. Other factors that can contribute to dry-eye symptoms with soft contact lenses are the environment, medications, computer use, and pregnancy.
Patient and Environmental Factors
A thorough case history will be important to elicit possible causes of dryness. Additionally, the patient should be questioned about any medical conditions, such as Stevens-Johnson syndrome (mucin deficiency), pregnancy (increase in tear viscosity), or Sjögren syndrome (aqueous deficiency). Medications that can alter the tear film are antihistamines, anticholinergics, antianxiety agents, phenothiazines, and oral contraceptives.20
The occupational environment (e.g., working near heating and air conditioning vents) may exacerbate dryness symptoms. Circulating air from automobile vents may also cause discomfort. The use of vent covers to redirect the air away from the wearer or changing the angle of the automobile vents should relieve dryness. Long-term computer use may cause a decreased blink rate, resulting in symptoms of dryness. This may be alleviated by having the wearer take blink breaks, such as at the end of each page of material. The same technique may be useful for others, such as students, who spend significant amounts of time reading. Airline passengers
may also experience dryness, particularly on long trips, because of the low relative humidity in airplane cabins at high altitude (Fig. 13.4).
may also experience dryness, particularly on long trips, because of the low relative humidity in airplane cabins at high altitude (Fig. 13.4).
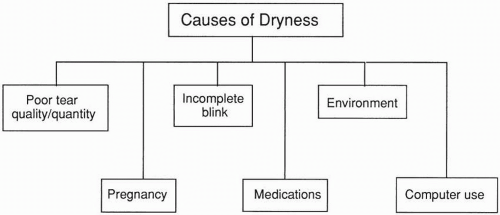 ▪ FIGURE 13.4 Summary of causes of dryness. |
Refitting the patient into a different material may be beneficial in reducing symptoms of dryness. Lenses containing phosphorylcholine have been reported to provide improved comfort.21,22 Additionally, some manufacturers incorporate compounds such as polyvinyl pyrrolidone and polyvinyl alcohol into lenses during the manufacturing process in an effort to provide comfort and lens hydration.23,24,25
Silicone hydrogel lenses have also been reported to provide increased comfort.26 This may be due in part to the low water content of silicone hydrogel lenses, which results in less lens dehydration. There is additional evidence that the increased oxygen provided by silicone hydrogel materials may decrease the ocular inflammatory response that may be found in hydrogel materials with low oxygen permeability (Dk). This inflammatory response may be responsible for ocular surface and lacrimal gland damage, which may cause ocular dryness; therefore, silicone hydrogel materials eliminate this damage and the dryness that results.27
Excessive Lens Movement
Deposited Lens
Surface deposits have been found to occur less frequently on disposable contact lenses than on conventional replacement lenses.28 Conventional replacement soft lenses or those that are used beyond their recommended replacement schedule may become very deposited and exhibit excessive movement. The patient may present with symptoms of decentration of the lens during eye movement or with complaints that the lens is easily dislodged from the eye. On observation with the biomicroscope, it will be apparent that the soft lens has become deposited. These deposits may be filmy coatings or elevated deposits. The most common and effective treatment for lens deposition is to fit the patient in disposable lenses. If the patient is already wearing disposable lenses, then education on compliance with replacement instructions is recommended.29
In addition, a patient exhibiting clinical signs and symptoms of a dry eye may also experience lens decentration or lenses that dislodge as a result of dehydration of the lens. Use of a soft lens that is recommended for dry eyes or the use of lens lubricants may alleviate dryness.
Inverted Lens
Another cause of a lens that moves excessively or that dislodges from the eye easily is an inverted lens. Patients should be educated on how to determine lens inversion at the dispensing visit; however, this is more difficult to distinguish with certain types of lenses and some patients. Methods of determining lens inversion by visual inspection have been described
previously (see Chapter 12). Repeated demonstration of these two methods may aid the patient in determining lens inversion. Graphics and photographs demonstrating lens inversion may be of additional help. When the lens is observed with the biomicroscope, it may exhibit excessive movement and edge lift. In addition, visual acuity may be reduced. If the patient finds visual inspection of lens inversion difficult and is experiencing decreased visual acuity, excessive lens movement, minor discomfort, or a lens that dislodges, the patient should suspect lens inversion and attempt to insert the lens in the other direction.
previously (see Chapter 12). Repeated demonstration of these two methods may aid the patient in determining lens inversion. Graphics and photographs demonstrating lens inversion may be of additional help. When the lens is observed with the biomicroscope, it may exhibit excessive movement and edge lift. In addition, visual acuity may be reduced. If the patient finds visual inspection of lens inversion difficult and is experiencing decreased visual acuity, excessive lens movement, minor discomfort, or a lens that dislodges, the patient should suspect lens inversion and attempt to insert the lens in the other direction.
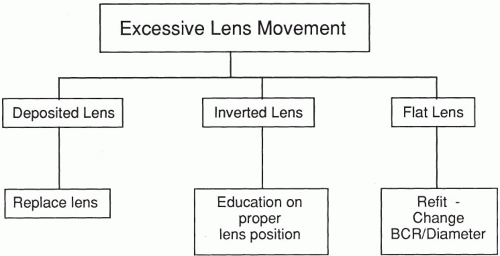 ▪ FIGURE 13.5 Summary of causes and management of excessive lens movement. |
Flat Lens
Excessive lens movement is also observed in soft lenses with a BCR that is too flat. Biomicroscopic evaluation of a soft lens that is too flat may reveal any of the following clinical signs or combination of signs: inferior lens decentration with the patient gazing straight ahead, corneal exposure on lens movement, edge lift, superior decentration on downward gaze, or lens movement >1.5 mm with the blink. A change to a steeper base curve or larger lens diameter should improve the soft lens-to-cornea fitting relationship (Fig. 13.5).
Foggy/Hazy Vision
Diagnosis
Foggy or hazy vision through a soft contact lens may result from a coated lens or corneal edema. A common symptom elicited from patients may be the appearance of halos around or distortion of bright point sources of light. Clinical signs of either a contaminated lens or corneal edema may be observed with a biomicroscope. To assist in determining the cause of the reduced vision, the patient may be questioned about the frequency of cleaning, method of disinfection (chemical, hydrogen peroxide), use of a daily cleaner and weekly enzyme, cleanliness of hands before lens handling, use of hand lotions or soaps containing moisturizers, and age of lenses. Patients in whom corneal edema is suspected should be questioned about their wearing time. The presence of epithelial edema as a result of “overwear” is infrequently noted in hydrogel lens wearers but may be observed in wearers of thick, low-water-content hydrogel lenses.12 Symptoms may be more prevalent after long periods of lens wear.
Treatment
In cases of a contaminated or coated lens, visual acuity will improve with the placement of a new lens on the eye. If the patient’s lens modality is only available in a conventional lens, they may need to utilize an abrasive cleaner, increase the number of enzymatic cleanings per week,
replace the contact lenses more frequently, or switch to a GP material. Patient education on proper cleaning and disinfecting techniques will help prolong the viability of the contact lens.
replace the contact lenses more frequently, or switch to a GP material. Patient education on proper cleaning and disinfecting techniques will help prolong the viability of the contact lens.
Removal of the contact lens and exposure of the cornea to air will result in a reduction of epithelial edema.12 Hypertonic solutions may be beneficial in severe cases of edema, although their use may be unnecessary with the level of epithelial edema found in hydrogel contact lens wearers.30 Switching patients to a lens material with a higher Dk/t (e.g., silicone hydrogel) and maintaining the patient on a daily-wear (DW) schedule will help reduce or eliminate the edema.12 Likewise, those patients who were fitted in lower-water-content lenses for comfort (e.g., dry-eye patients) may be refitted in silicone hydrogel lenses to alleviate epithelial edema.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


