this group of patients, some may require a longer amount of time. This is usually of no consequence if the patient is beyond the critical period and without risk of refractive amblyopia and if good visual acuity is maintained in the paired eye. Correction of the pediatric aphakic patient should be performed as soon as possible. Most often this can be achieved within 5 days following the primary surgical procedure. This is especially true if small-incision techniques are used, which allow for a short healing period and reduced postoperative astigmatism.
and optic cap (front optical zone) to be used during lens manufacture (Fig. 17.2). While a flatter flange radius will usually assist in maintaining a superior lens-to-cornea fitting relationship, this may also result in increased lens awareness. An approximate, desired flange radius between 1.0 and 2.0 mm flatter than the base curve radius in millimeters is recommended.4 For example, if a lens is ordered with a 45.00 D (7.50 mm) base curve radius, one would expect to order a flange radius of 8.5 to 9.5 mm. With few exceptions, the optic cap should be equal to the back optic zone diameter. A recommended diagnostic fitting set for lenticular lenses is found in Table 17.1.5 Effective Power and Vertex Power optical considerations are provided in Appendix A and B respectively.
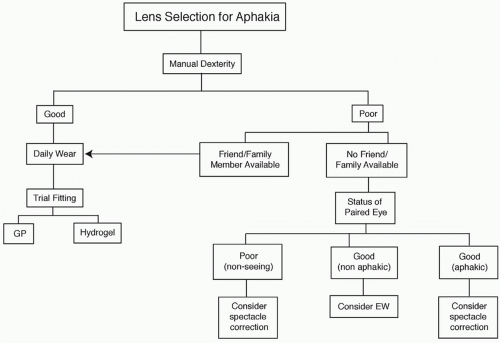 ▪ FIGURE 17.1 Factors influencing the initial lens of choice for contact lens correction of aphakia. |
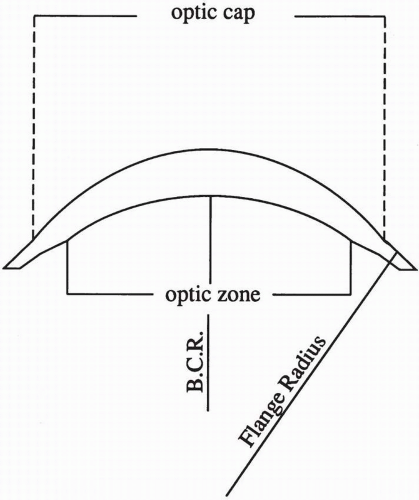 ▪ FIGURE 17.2 Design of a minus carrier aphakic contact lens. |
TABLE 17.1 SUGGESTED LENTICULAR APHAKIA TRIAL LENS SET (RECOMMENDED MATERIAL IS PMMA OR A LOW DK GAS PERMEABLE MATERIAL) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
secondary to trauma may also have iris defects resulting in large or ectopic pupils. These patients may benefit from a dark-tinted, hydrogel contact lens creating an artificial pupil and iris, which attenuates bright light. Hydrogel lens designs are more suitable for this application, as they more readily accept tint and encompass more of the corneal surface while providing better centration with decreased movement.
TABLE 17.2 SUGGESTED SINGLE-CUT APHAKIA TRIAL LENS SET | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 17.3 HYDROGEL AND SILICONE HYDROGEL PLANNED-REPLACEMENT LENSES IN APHAKIC POWERS | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


