There is very little doubt that tremendous potential exists for expanding your contact lens practice in the ever-increasing presbyopic marketplace. It is rapidly growing and is currently the largest segment of the population as well as the largest relatively untapped segment of the contact lens market.1,2,3,4 With 78 million baby boomers (i.e., those born in the United States between 1946 and 1964) now entering presbyopia, a large group of potential bifocal contact lens wearers will exist.1 It is certainly evident that a contact lens that provides more natural vision will appeal to them, as would any product or service that claims to be all natural. The older cohort—those in the 45 to 54 age range—are in their peak earning period. They are willing to pay extra for features and benefits they perceive to be of value or that enhance the quality or services being provided.1 Therefore, with the natural vision, binocularity, and cosmesis provided by bifocal contact lenses to a population in which vanity is important, the bifocal market has much potential in the coming decade.1,5,6 Although this chapter will refer to this form of contact lens as “bifocals,” most of these designs provide correction for more than two distances and would best be described as “multifocals.” Other forms of presbyopic contact lens correction include single-vision distance-correcting contact lenses in combination with reading glasses, and monovision, in which one eye is optimally corrected for distance and the other eye is optimally corrected for near.
The primary question is: Will practitioners fit them? Although 18% of soft lenses in the United States are prescribed for presbyopia,7 two-thirds are prescribed for monovision.8 Worldwide, the values are much smaller, with 6% of presbyopes wearing soft lenses and only half of this group wearing bifocal or multifocal lenses.
Why is this percentage of contact lens-wearing presbyopes so low? Certainly, the reasons are multifold and include practitioner apprehension. Common comments from patients have indicated that when asked about bifocal contact lenses, it is not uncommon to hear such responses as: “I never knew bifocal contact lenses existed” or “I’ve heard of them but my previous doctor said they don’t work.” Actually, the latter is a true comment. Bifocal contact lenses are not successful—until they are diagnostically fit to the patient. This is confirmed by a study by Jones et al,9 who divided subjects into “reactive” (i.e., contact lenses were not presented to them initially as an option) and “proactive” (i.e., contact lenses were actively discussed as a viable option). The results showed that, whereas 9 of 80 subjects were fit into contact lenses in the reactive group, 46 of 80 subjects, including 21 of 33 presbyopic patients, were fit into contact lenses in the proactive group.
Bifocal contact lens patients not only receive the binocular vision advantages and more natural vision, but they also can represent the most enthusiastic patients in the practice who can refer others and allow practitioners to build their contact lens practice. Patients being told either that there is no such option or that bifocal lenses are not successful or those automatically being fitted into monovision (one eye optimally corrected for distance, the other eye for near) are not being properly managed. Instead, these patients should be referred to a practitioner who is fitting bifocal contact lenses. There are numerous stories in the literature of how fitting presbyopic patients into bifocal contact lenses had a significant impact on their lives.10,11
Some explanations for the limited bifocal contact lens applications do have merit. Although translating gas-permeable (GP) bifocal designs can claim as good or better vision at distance and near versus progressive addition spectacle lenses (PALs), most contact lens bifocal/multifocal designs do represent some compromise. Most designs have multiple vision corrections in front of the pupil at the same time, termed simultaneous vision designs. Although the compromise in vision may only be mild with some designs, it must be considered with patients having critical vision demands. In addition, the spectacle lens market is enjoying considerable success as a result of the enormous amount of publicity aimed at showing the glamour and beauty of today’s fashion frames. Presbyopic spectacle sales also benefit practice income.
Nevertheless, presbyopic patients deserve the opportunity to be educated and, if interested, to be fitted with bifocal contact lenses. These specialty contact lenses are not for everyone, as will be discussed later in this chapter. However, consumer interest is increasing—and will continue to increase—as a result of several recent advancements with these designs including the following: (a) soft disposable multifocal and bifocal designs allow the ability of the presbyope to minimize lens deposit-related problems and to have replacement lenses readily available, while also allowing the practitioner the ability to trial a pair of lenses for a short time period (typically 1 week) and make any indicated changes; (b) silicone hydrogel materials in presbyopic designs have allowed a cohort of contact lens wearers who require high oxygen transmission to achieve this goal; (c) high add aspheric multifocal GP designs have allowed the more mature presbyope to see at all distances via an aspheric design; and (d) GP segmented, translating designs with intermediate vision capabilities allow the advanced presbyope with critical vision needs at all distances to meet these needs. In addition, members of this population are more active than their predecessors, making spectacle correction a less desirable option for visual freedom. As PALs often require numerous head movements to find the optimum position for computer use and other intermediate tasks, because of the varying corrective powers present during any eye movement, they can also represent compromise.12,13,14,15 Also, as will be emphasized in this chapter as well, the fitting and problem solving of these designs are not nearly as complicated as one might perceive them to be. With the baby boomers becoming presbyopic, it makes good sense to present this option to all presbyopic patients in your office.
▪ PATIENT SELECTION AND EVALUATION
Practice Promotion
The first important step toward achieving success with a potential bifocal contact lens patient is practice promotion of this contact lens option. Patient brochures can be displayed in the reception area as well as the examination rooms. This gives the patient every opportunity to review this material before the examination and introduce them to the possibility of wearing bifocal contact lenses. Obviously, practice newsletters and—an ever-increasingly popular modality—the practice website can be used to inform both current and potential future patients about bifocal contact lenses.
Comprehensive Preliminary Evaluation
Aging Changes
To determine if the patient is a good candidate, an understanding of normal changes occurring over time is important.16,17 Aqueous tear production and stability of the tear film both decrease with age, making the patient more susceptible to dry eye, which can affect the wetting and comfort of contact lenses. In fact, it has been found that, whereas 28% of presbyopic patients reported dryness before contact lens wear, 68% reported dryness after 6 months of lens wear.18 Older eyes are also more likely to have developed pingueculae and pterygia, which can further disrupt the tear film and decrease contact lens comfort. Loss of endothelial cells throughout the lifespan makes the cornea more susceptible to edema, and since most bifocal contact lenses are thicker by nature, materials must be chosen with oxygen transmission in mind. As a result of crystalline lens changes, reduction in light transmission, a decrease in retinal sensitivity, and reduced contrast sensitivity occur as well. Loss of eyelid tonicity occurs with age and can present problems with translating bifocals.
Tests to Perform
Fitting a patient who is not a good candidate for bifocal contact lenses will almost always result in failure, and with the high cost of chair time and patience, it is advisable to rule these patients out before any fitting begins. The preliminary evaluation tests to perform are listed in Table 15.1.
Case history. A comprehensive case history should be performed to determine the patient’s goals, motivation (to be discussed), history of medications, history of surgery (notably cosmetic surgery), visual requirements, and occupational requirements. It is important to ask if the patient is currently taking any medications and record all medications being used. Numerous medications—including antihistamines, ibuprofen, estrogen, tricyclic antide-pressants, anticholinergics, and the scopolamine patch—can reduce tear volume.18 It’s important to ask about previous surgeries. With cosmetic lid surgery becoming increasingly popular, this may affect GP bifocal and multifocal lens positioning by exerting excessive lifting with the blink.
Visual requirements. The patient’s visual requirements need to be carefully evaluated. Open discussions between the doctor and the patient about life and work styles are mandatory if success is to be obtained. This will be further discussed in the forthcoming section on consultation.
Anatomic measurements. Performing anatomic measurements such as vertical fissure size, horizontal visible iris diameter, and pupil diameter will be beneficial. Pupil diameter determination should be obtained both in normal room illumination and with the lights dimmed. Patients wearing simultaneous vision designs will be impacted by the variance in pupil diameter with changes in illumination. In particular, patients with a large pupil diameter (>5 mm in normal room illumination), although relatively uncommon in the presbyopic population, would be contraindicated for a GP aspheric lens design because of the glare and ghosting of images that would occur during low illumination conditions.15 In addition, patients with a “low” lower lid (i.e., over 1 mm inferior to lower limbus) will not be good candidates for GP translating bifocals because of poor or no alignment of lower lens to lid. Likewise, patients exhibiting poor (i.e., loose) lid tonicity/elasticity would be poor candidates for translating designs.
TABLE 15.1 PRELIMINARY EVALUATION TESTS FOR THE POTENTIAL PRESBYOPIC CONTACT LENS PATIENT
1.
Case history
• Medications
• History of surgery
• Visual requirements
• Occupational environment
• Goals
2.
External findings
• Vertical fissure size
• Lid position and tonicity
• Pupil size (normal room illumination; dim illumination)
• Blink rate/quality
3.
Tear volume and quality
4.
Corneal integrity
5.
Refraction: BVA at distance and near; add power
6.
Keratometry/corneal topography
BVA, best corrected visual acuity.
Tear film evaluation. The patient should blink completely and frequently (at minimum, every 5 seconds). The tear meniscus should be evaluated, and the customary tests for tear quality [tear breakup time (TBUT)] and quantity (i.e., Zone-Quick or Schirmer) should be performed. Patients exhibiting a TBUT of ≥10 seconds should experience successful all-day wear,19 whereas those with less than this value should be advised that they will not typically achieve an all-day wearing period.20 In particular, if the TBUT is between 6 and 9 seconds, patients should be informed that all-day wear may not be possible and extended wear is not recommended.21 These individuals tend to optimize their wearing period via the use of either silicone hydrogel disposable lenses or GP lenses. They also benefit from regular cleaning of their lenses as well as frequent rewetting drop use. A TBUT of ≤5 seconds typically contraindicates contact lens wear, especially if the measurement is repeatable.22
Biomicroscopy. A careful biomicroscopic evaluation is important to rule out corneal dry spots or other causes of staining. Lid eversion will be important to ensure that significant papillary hypertrophy is not present.
Refraction. A refraction will help in determining motivation. The best candidates for bifocal contact lenses should have more than 1 D of hyperopia or more than 1.25 D of myopia.23 Low hyperopic patients typically expect better vision through the contact lenses since spectacles were not necessary before presbyopia. Low myopic and emmetropic patients entering presbyopia are also difficult to please since they can typically see quite well at near without any correction. However, they should not be excluded if, in fact, they are motivated. These individuals may appreciate wearing one distance lens only (if exhibiting low myopia) or either one near lens or a soft bifocal lens on one eye if emmetropic. If the patient is amblyopic, unless an optimum translating bifocal fitting relationship can be achieved, a bifocal lens is often contraindicated because of possible further compromise in vision.
Corneal topography. Finally, corneal topography evaluation will assist in both determining whether the patient is a good candidate for bifocal lenses and what specific lens design would be indicated. Although corneal topography evaluation is not essential when fitting the presbyopic patient into contact lenses, it is beneficial in determining the size and location of the apex and the eccentricity of the cornea and, in some cases, assisting with the design parameters.15 In particular, when GP lenses are the preferred option, a centrally positioned apex lends itself to an aspheric design, whereas an inferior positioned apex would be desirable for segmented, translating designs. Patients having keratoconus or other forms of irregular cornea are often poor candidates because of some compromise in distance acuity that may result with bifocal contact lenses.
The characteristics of good and poor candidates for bifocal contact lens wear are given in Table 15.2.
Patient Consultation
This is perhaps the most important factor when considering bifocal contact lens success. Good bifocal contact lens patients need to be sufficiently motivated to give their lenses appropriate care and should be made thoroughly aware of the level of visual quality to be expected well before the initial fitting. A comprehensive education program is extremely valuable, as it will help to develop the correct amount of optimism and realism concerning bifocal contact lens wear. A well-informed patient is your best patient.
TABLE 15.2 GOOD AND POOR CANDIDATES FOR BIFOCAL CONTACT LENS WEAR
GOOD CANDIDATES
POOR CANDIDATES
Motivated presbyopes (do not want to wear spectacles)
Vision demands are not very critical
Normal lid tonicity
Good ocular health; good tear quality (>10 sec TBUT) and volume
Unmotivated
Critical vision demands
Poor tear quality (≤5 sec TBUT) and/or volume
Irregular cornea
Amblyopia
TBUT, tear breakup time.
What are the patient’s expectations? Is poor cosmesis with spectacles present? If the patient spends most of the time performing critical near tasks, failure with bifocal contact lenses is probable. The questions about lifestyle/visual demand presented in Table 15.3 have been recommended for potential presbyopic bifocal contact lens wearers.24
Are spectacles undesirable when in the public eye?
a. Yes
X
b. No
X
3.
How much time do you spend doing precise work like accounting?
a. Very little
X
b. A lot
X
4.
How much time do you spend doing intense reading during the day?
a. Very little
X
b. A lot
X
5.
Are spectacles bothersome in your sports and leisure activities?
a. Yes
X
b. No
X
6.
Do you dislike spectacles?
a. Yes
X
b. No
X
From Friant RJ. When bifocal lenses are most likely to succeed. Contact Lens Spectrum 1986;1(6):14-23.
The process begins by always asking patients if they are interested in contact lenses. They may not be aware that you fit contact lenses, not to mention bifocal contact lenses. They may be assuming that bifocal spectacle wear is their only option. This simple invitation to try contact lenses may significantly change a patient’s quality of life; nevertheless, it has been found that practitioners ask <20% of their spectacle-wearing patients if they would be interested in wearing contact lenses.11 If patients show interest and appear to be qualified, they can be told about all of the patients who have experienced an enhanced quality of life through bifocal contact lenses, as they are free from spectacle lens wear. The availability of disposable bifocal lenses allows the practitioner the opportunity to prescribe them on a trial basis for those patients deemed good soft lens candidates.
It is important to determine what patients’ goals from contact lens wear are and, specifically, to determine which distances are most important to them. How they spend their time during the day and what visual tasks are especially important and time consuming (i.e., computer use, driving, reading, etc.) should be asked about. The goal should be to satisfy their primary visual demands. Patients should not be guaranteed that spectacles will not be necessary if they are fitted into a presbyopic contact lens correction. Not only should they have a spectacle correction to use as a backup to contact lenses (perhaps for morning or evening wear or to have available if lens loss or an eye infection occurs), but also monovision wearers should be encouraged to wear overspectacles for critical distance tasks (especially driving), and some aspheric multifocal wearers appreciate additional plus power when reading fine print (especially in dim illumination) or perhaps some additional minus power when driving at night.
A positive, optimistic but realistic approach is best. It is particularly important to “underpromise and overdeliver” with presbyopic patients being fitted into contact lenses. They need to be aware of possible compromises, including the fact that they do not have the focusing ability of a teenager. Even with the best technology available, bifocal contact lenses will not meet all of their visual demands. They need to appreciate that bifocal contact lenses are different from spectacles. Patients should be told that they may not experience the same quality of vision as with spectacles as contact lenses are dynamic devices that sit directly on the eye, unlike spectacles, in which good near vision can be obtained via simply dropping the eyes to view through the bifocal segment. If patients appear to be quite satisfied with spectacle wear and/or are extremely concerned about any possible compromise in vision, they can be told that bifocal lenses may not be the best option for them. In that way their motivation can be assessed. Conversely, there are patients who will accept reasonable visual compromise to experience the benefits of contact lens wear. “20/Happy” is a phrase in common use today to describe patients who experience a slight decrement in acuity chart vision (often 20/25 to 20/30) but are extremely satisfied with their bifocal contact lenses.
Finally, it is important to review all of the contact lens corrective options with patients. Single-vision contact lenses, supplemented by reading glasses, can be mentioned first. Patients can be told that this option should provide them with their best vision at near and distance. They should also be informed that some patients do not like to put the spectacles on and take them off frequently (not to mention the wearing of spectacles in general). The second option to explain would be monovision. A surprising number of patients have already heard of this option, but it should be defined to patients nevertheless as an option in which one eye sees optimally at distance whereas the other eye sees well at near. The fact that the opposite eye will be somewhat blurred for any visual task and the need for supplemental vision correction (i.e., a second distance contact lens or “driving” glasses) for critical vision tasks should be explained. Finally, bifocal contact lenses can be presented. This option allows the patient the aforementioned benefits of visual freedom and binocularity. Although the higher cost should be mentioned (often one and one-half to two times the cost of conventional designs), as well as the possibility of a lens exchange or two to fine-tune the fit (although the patient rarely needs to discontinue lens wear during this period), patients can be told that if they are patient and motivated, there is a good likelihood for success.
▪ SOFT BIFOCAL AND MULTIFOCAL LENSES
Soft contact lenses for presbyopia were introduced in the 1980s. The first lenses were expensive to manufacture and custom made; therefore, the cost to the patient was high. This, compounded with the inherent nature of soft lenses to deposit and tear, as well as the lack of success of the designs and product discontinuation, made this a less than desirable modality for practitioners and patients. Translating designs in GP lenses are beneficial for providing increased near vision; however, translating designs have not been very successful in soft contact lenses. Most soft contact lenses for use with presbyopia are a simultaneous vision design. This may result in compromised vision, as this design does not provide the same clarity as spectacles, but the patient may be satisfied with the vision. The simultaneous existence of a focused image and an out-of-focus image on the retina results in a reduction in retinal image quality.6,25 Despite this, many patients experience satisfactory vision and success when wearing these lenses.
The introduction of disposable/frequent-replacement soft lenses and silicone hydrogel lenses has increased the popularity and success of soft bifocal and multifocal contact lenses. As the baby boomer population increases and their desire to remain lifelong contact lens wearers has increased, bifocal contact lens use is on the rise.8,26 In addition to the disposable lenses and the increased oxygen transmission, material changes that aid dry-eye patients and the ease in fitting and dispensing trial lenses have been a large part of this upward trend in bifocal/multifocal use.
Patient Selection
Motivation is a key factor for these patients. Planting the seed in single-vision soft lens wearers before they require a presbyopic correction is beneficial to them remaining lifelong contact lens wearers. Although the process of fitting is easier than in the past, enthusiasm on the part of the practitioner and patient will affect patient motivation.27
Patient education is another key factor for success. This requires a thorough explanation for what is occurring in presbyopia and methods of correcting for it, including reading glasses over contact lenses, monovision, and bifocal contact lenses. The patient needs to know that these lenses are a little more complicated and may require some compromise, but with motivation and patience, success is obtainable. Thorough education makes patients feel a part of the fitting and makes the process more understandable. Their input is vital in arriving at a successful endpoint.
Normal age-related changes may affect the patient’s ability to wear soft multifocals successfully. Ocular dryness may be an issue and may be managed by lens materials and solutions. More complicated age-related changes, like cataracts and macular degeneration, may result in unacceptable vision.
Good candidates for soft multifocals include successful single-vision soft lens wearers, dissatisfied monovision patients, those with low amounts of astigmatism (unless fitted in a toric multifocal), moderate myopes and hyperopes, and those with a healthy cornea and tears. The patient may have to accept some compromise, usually in one area, either distance, intermediate, or near (Table 15.4).
Lens Designs
Center-Near
Many of the soft multifocal lenses are aspheric with a center-near correction. Examples of disposable/frequent-replacement center-near multifocals are listed in Table 15.5. These centernear designs are discussed in this section.
The Soflens Multifocal and the PureVision Multifocal (Bausch & Lomb) are aspheric, center-near designs. The anterior surface is aspheric and the back surface is a spherical bicurve. The Soflens Multifocal is available in two base curve radii (BCR) (8.5 and 8.8 mm) and is a 2-week replacement lens. The PureVision Multifocal is a silicone hydrogel lens, approved for daily, extended, or continuous wear (up to 30 days). It is available in one BCR (8.6 mm) and is a monthly replacement lens.
TABLE 15.4 SOFT MULTIFOCAL PATIENT SELECTION
•
Motivation
•
Successful soft lens patient
•
Computer users
•
Dissatisfied monovision wearer
•
Healthy cornea, lids, and tear film
•
Low astigmats (unless fitting a toric multifocal)
•
Emmetropes and low myopes (hyperopes are less successful)
When fitting these lenses, the 8.5-mm BCR is used first on the Soflens Multifocal and the 8.6-mm BCR for the PureVision Multifocal. The lenses come with two add powers, low and high add. If the patient has a spectacle add ≤ + 1.50 D, the low add is recommended to be used on both eyes. For an add power between + 1.75 and +2.25 D, mixed adds are recommended, with the low add on the dominant eye and the high add on the nondominant eye. Adds ≤ +2.50 D are fit with the high add on both eyes.
C-Vue Multifocals and EMA Multifocals (Unilens Corp.) are both aspheric center-near designs with two adds, low and high, similar to the Bausch & Lomb lens designs. Quattro (Blanchard) is an aspheric center-near design that comes in two BCR (8.4 and 8.8 mm). It is available in an add power that corrects up to +2.50 D. When fitting this lens, the spherical power is based on the distant spherical equivalent power corrected for the required add (Table 15.6). If the patient has an add <+ 1.25 D, it is recommended that the dominant eye be fitted in a spherical distance lens and the nondominant eye be fitted with a lens of a power equal to the distance power (spherical equivalent, vertexed) with + 1.25 added. For example, a patient with a −2.50 D OU and +1.00 Add right eye dominant would wear a spherical −2.50 D lens on the OD and a −1.25 D Quattro lens on the OS. BCR selection is 8.4 mm with a 14.2 mm diameter for keratometry readings ≤44.50 D, and 8.8 mm with a 14.5 mm diameter for keratometry readings ≤44.25 D.
Focus Progressive and Focus Dailies Progressive lenses (Ciba Vision) are aspheric, centernear designs with an add power that corrects up to +3.00 D. A formula is used to determine the distance prescription to select. The formula is based on adding half the patient’s add power to their spherical equivalent, vertex-corrected distance prescription. For example, a patient with −3.00 D spectacle prescription and a + 1.00 D add would require the following:
Proclear, Proclear XR, Frequency, and Proclear Toric Multifocal (N lenses)
CooperVision
C-Vue 55 and Toric Multifocal
Unilens
EMA Multifocal
Unilens
TABLE 15.6 QUATTRO POWER SELECTION (ADDED TO DISTANCE RX—SPHERICAL EQUIVALENT, VERTEXED)
ADD (YR OLD)
DOMINANT EYE RX
NONDOMINANT EYE RX
+1.25 (≤46)
1.00
1.25
+1.50 (47-48)
1.00
1.25
+1.75 (49-50)
1.25
1.50
+2.00 (51-52)
1.50
1.75
+2.25 (53-54)
1.75
2.00
+2.50 (≥55)
1.75
2.25
These lenses are labeled with only the distance prescription. This simplifies the fitting process, but limits the available choices for the patient. If the patient’s distance vision is not acceptable, decreasing the amount of the plus power added to the distance prescription of, at minimum, the distance eye, may be beneficial.28 The Focus Dailies Progressive is the only daily disposable multifocal lens, which can be advantageous for occasional wearers, frequent travelers, and those with allergies.
There are conventional replacement (6-12 months) center-near lenses available, which are fit similar to these lenses. Because of the number of conventional center-near lenses, they will not be discussed individually in this chapter.
Center-Distance
Currently available disposable/frequent-replacement center-distance lenses are listed in Table 15.7.
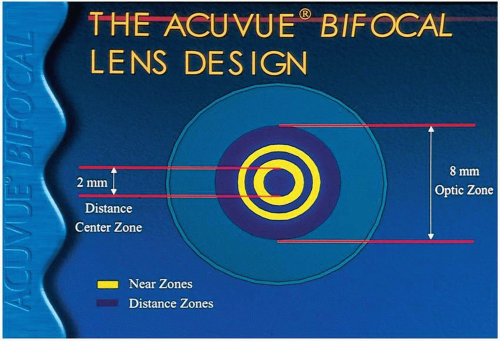
The Acuvue Bifocal (Vistakon) is a concentric bifocal with five alternating concentric rings and four add powers (+1.00, +1.50, +2.00, and +2.50 D). The central distance zone is 2 mm wide surrounded by a near zone, alternating distance and near for a total width of 8 mm (Fig. 15.1). The add power selection is based on the patient’s age (Table 15.8).
This lens is less dependent on pupil size than aspheric designs because of the alternating zones within the pupil, which aid in providing an equal area of distance and near over a range of pupil sizes.29 One study found that the Acuvue Bifocal, when compared with progressive addition spectacles at varying illuminations, resulted in similar near performance.30
Proclear, Proclear XR, Frequency, and Proclear Toric Multifocal (D lens)
CooperVision
Acuvue Bifocal
Vistakon
UCL Multifocal
United Contact Lens
▪ FIGURE 15.1 The Acuvue Bifocal.
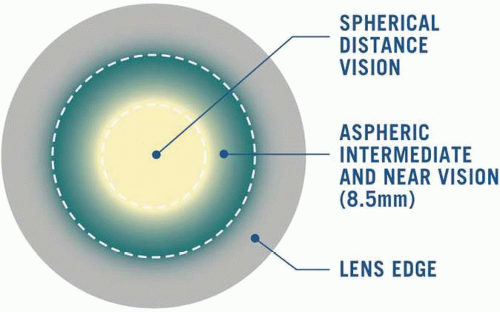
Biomedics EP (CooperVision) has a center spherical distance zone with a progressive aspheric zone that provides intermediate and near vision for emerging presbyopes (Fig. 15.2). The design is similar to the D lens of other CooperVision multifocals. This lens is easy to fit as there is only one BCR and the lens power is selected based on the patient’s distance spectacle prescription. This lens can provide an effective add power of, at maximum, +1.50 D. No add power is recorded on the lens pack as it is the same for all lenses. This lens is made of omafilcon A (Proclear material); therefore, it is recommended for dry-eye patients. This is beneficial for those presbyopic patients that experience dryness.
Frequency 55 and Proclear Multifocals (CooperVision) have a unique design that allows creativity in fitting patients’ visual needs. Both lenses are available in one base curve radius and four add powers (+1.00, +1.50, +2.00, and +2.50 D). A recent addition to this family of multifocals, the Proclear XR Multifocal, has expanded parameters for distance powers of ±20 D and add powers from +0.75 to +4.00 D in 0.50 D steps. This creates a wide range of multifocal lenses for almost every patient, regardless of their spectacle power. In the future, we can expect this design to be available in the Biofinity silicone hydrogel material.
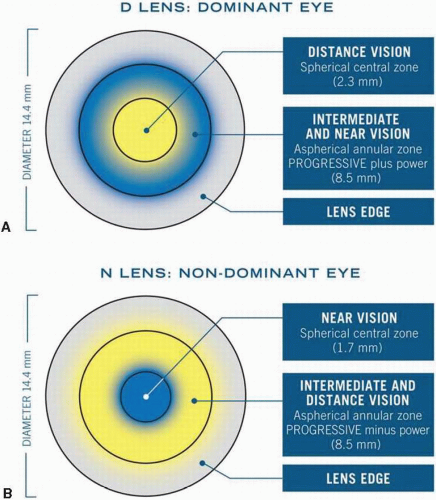
These multifocals have a D lens, which is fitted on the dominant eye and has a center-distance spherical zone, surrounded by an aspheric progressive intermediate zone and then an outer spherical near zone. The N lens, fitted on the nondominant eye, has a center-near spherical zone, surrounded by the aspheric intermediate progressive zone and a distance spherical zone. This design is termed Balanced Progressive Technology (Fig. 15.3A,B). This lens design has been very successful. One study comparing the Soflens Multifocal with the Frequency Multifocal found that the Frequency lens had better near vision and superior stereopsis when compared by patients wearing the Soflens.28,31
▪ FIGURE 15.2 Biomedics EP. (Courtesy of CooperVision.)
When fitting this design, the initial power is based on the spherical equivalent of the current refraction, vertexed back to the cornea. The add should be equivalent to the add for spectacles unless it is between add powers; if this occurs, the lower add should be selected. As indicated previously, the D lens should be used on the dominant eye and the N lens on the nondominant eye. The manufacturer recommends that 20/20 vision be obtained binocularly at distance and near. Monocular visual acuities with the D lens should be 20/20 at distance and 20/40 or better at near. The reverse is true of the N lens, where distance visual acuity should be 20/40 or better and near visual acuity 20/20. If the visual acuity does not meet these criteria, then an overrefraction should be performed monocularly to improve the vision.32 Conventional lens replacement materials, available in this center-distance design, include Satureyes Multifocal and Metrofocal (Metro Optics) and 4Vue and XTRA (Unilens Corp.).
▪ FIGURE 15.3 (A,B) The Frequency 55 and Proclear Multifocals utilize a distance center (“D” in A) and near center (“N” in B). (Courtesy of CooperVision.)
Translating
The only soft lens currently available in a translating design is the Triton Translating Bifocal (Gelflex). Translation is more challenging with a soft lens bifocal than a GP bifocal, but can provide better vision than simultaneous designs. The thicker inferior edge may cause more lens awareness.33 The Triton lens is available in sphere and toric conventional replacement lenses. It is a back surface design with biprism and truncation for stability and position.34 The horizontal diameters are 14.5 and 15.0 mm with vertical diameters of 11.4 to 13.9 mm. The near seg is located 1 mm below the geometric center. Marker dots on the lens at the 3 and 9 o’clock positions mark the geometric center of the lens and aid the practitioner in adjusting the vertical size to affect the fit and seg position.35 In the near future, we can expect more bifocal/multifocal designs and more silicone hydrogel multifocal lens materials.
Soft Toric Multifocals
Several manufacturers make soft toric multifocal lenses, which increases the range of refractive errors that can be corrected. Until there are more of this type of lens available in disposable/frequent-replacement modalities and silicone hydrogel materials, the lenses still will be limited in use. Two soft toric multifocals that are available in multipacks for frequent replacement are the Proclear Multifocal Toric (CooperVision), replaced monthly, and the C-Vue 55 Toric Multifocal (Unilens Corp.), replaced quarterly. Both designs are similar to their spherical counterpart. Both are available in a prescription of ±20 D and a large range of cylinder powers and full axis range. In addition, there are several conventional replacement soft toric multifocals, which include the Cibasoft Progressive Toric (Ciba Vision) and the Essential Soft Toric Multifocal (Blanchard).
Fitting
Preliminary Testing
The fitting process is important to the success of the bifocal contact lens fitting. Examination procedures that should be performed before lenses are placed on the eye include current refraction, add determination, keratometry readings, determination of dominant eye, pupil size, TBUT, and a discussion pertaining to the patient’s visual needs. Initiating the process with a current refraction and add power aids in the selection of the initial diagnostic lenses. In cases where the lenses must be ordered empirically, errors in the refraction contribute to patient and practitioner frustration and increase chair time. Keratometry may not be crucial with every lens design, as many of the lenses are only available in one BCR; however, it is beneficial if the cornea is exceptionally steep or flat, or if the lenses are available in more than one BCR.
Only gold members can continue reading. Log In or Register to continue