FIGURE 9.1 Oral Appliance.
Mandibular advancement appliance for mild to moderate sleep apnea. (From Flint PW, Haughey BH, Lund VJ, et al. Cummings Otolaryngology—Head and Neck Surgery. 6th ed. Philadelphia, PA: Saunders; 2015, fig. 18-11.)
Surgical Management of Snoring
• Septoplasty/turbinate reduction
• Radiofrequency palatoplasty/somnoplasty (ablation of upper-airway tissue, including the palate, turbinates, and tongue base)
• Palatal implants (Fig. 9.2)
Upper-Airway Resistance Syndrome
Upper-Airway Resistance Syndrome Diagnosis
• 15 or more RERAs per hour
Risk Factor for Upper-Airway Resistance Syndrome
• Female gender
• Nonobese
• Younger age
• Nasal obstruction
Obstructive Sleep Apnea Syndrome
Obstructive Sleep Apnea Syndrome Diagnosis
• ≥5 respiratory events/hour AND respiratory effort with symptoms OR
• ≥15/hour respiratory events with respiratory effort without symptoms
Obstructive Sleep Apnea Syndrome Pathophysiology
• Upper-airway collapse
• Inability for airway dilators to respond
• Decreased sensitivity of chemoreceptors
• Decreased central respiratory drive
• Defective ventilator receptors
Obstructive Sleep Apnea Syndrome Risk Factors: Basic
• Obesity
• Family history
• Anatomy (maxillary hypoplasia; retrognathia)
• Increased age
• Allergies
• Postmenopausal status
• Sedatives and alcohol
• Smoking
Obstructive Sleep Apnea Syndrome: Systemic
• Down syndrome
• Marfan syndrome
• Neuromuscular disorders
• Muscular dystrophy
• Kyphoscoliosis
• Amyloidosis
• Endocrine abnormalities
Obstructive Apnea Syndrome Risk Factors: Miscellaneous
• South Asian ancestry
• ApoE4 allele
Clinical Consequences of Obstructive Sleep Apnea
• Sleep-related
• Daytime somnolence and fatigue, morning headache, motor vehicle accidents, poor job performance, depression, and familial stress
• Cardiovascular consequences
• Hypertension, coronary artery disease, cardiac arrhythmia, and cerebrovascular accidents
• Pulmonary consequences
• Pulmonary hypertension
• Cor pulmonale
• Shorter life expectancy
Workup of Obstructive Sleep Apnea
• Loud nightly snoring
• Daytime sleepiness/fatigue (Box 9.1)
• Unrefreshing sleep
• History from bed partner (witnessed breathing pauses and gasps)
• Physical exam
• Vital signs
• Body mass index (BMI)
• Head and neck exam
• Awake supine flexible laryngoscopy with Mueller maneuver
• Laboratory studies
• Polysomnography
• Cephalometric films
• Oximetry
• Thyroid and cardiac studies
Basic Sleep History
• Bedtimes
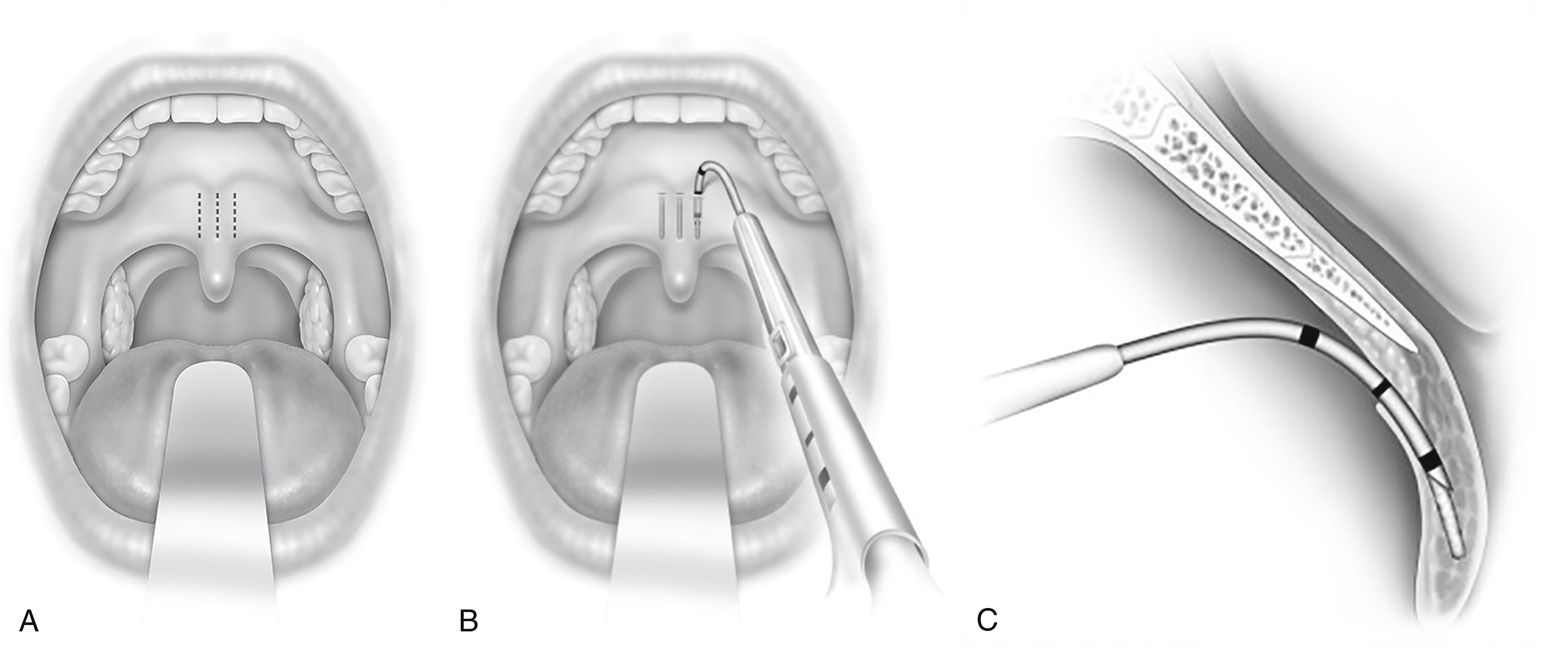
FIGURE 9.2 Placement of Palatal Implants.
(A) Approximate location of implant. (B) Coronal view showing placement of implant. (C) Sagittal view showing placement of implant. Pillar® implant technique may be conducted in the office or operating room. (Modified from Maurer JT. Palatal implants for primary snoring: Short- and long-term results of a new minimally invasive surgical technique. In: Friedman M, ed. Sleep Apnea and Snoring. Philadelphia, Elsevier, 2009.)
• Awake times
• Body position during sleep
• Restless sleep
• Leg movements/kicking
• Alcohol or sedative use
• Caffeine intake
• Mouth breathing at night
• Menopause status
Physical Exam Findings of Obstructive Sleep Apnea (Table 9.3)
• Neck circumference (≥17 inches males; ≥15.5 inches females)
• Waste/hip ratio (≥0.9 male; ≥0.85 female)
• Cricomental distance (≥15 mm excludes OSA)
• Kyphosis
• Micro/retrognathia (class II occlusion)
• Enlarged tonsils
• High arched palate
• Maxillary retrusion (class III occlusion)
Table 9.3
Physical Exam Findings of Obstructive Sleep Apnea
From Flint PW, Haughey BH, Lund VJ, et al. Cummings Otolaryngology—Head and Neck Surgery. 6th ed. Philadelphia, PA: Saunders; 2015, box 18-3.
• Tracheo/laryngomalacia
• Enlarged tongue (modified Mallampati III or IV)
Evaluation of Maxillary Retrusion
• Frankfurt plane
• Line dropped from the nasion to the subnasale should be perpendicular to the Frankfurt plane
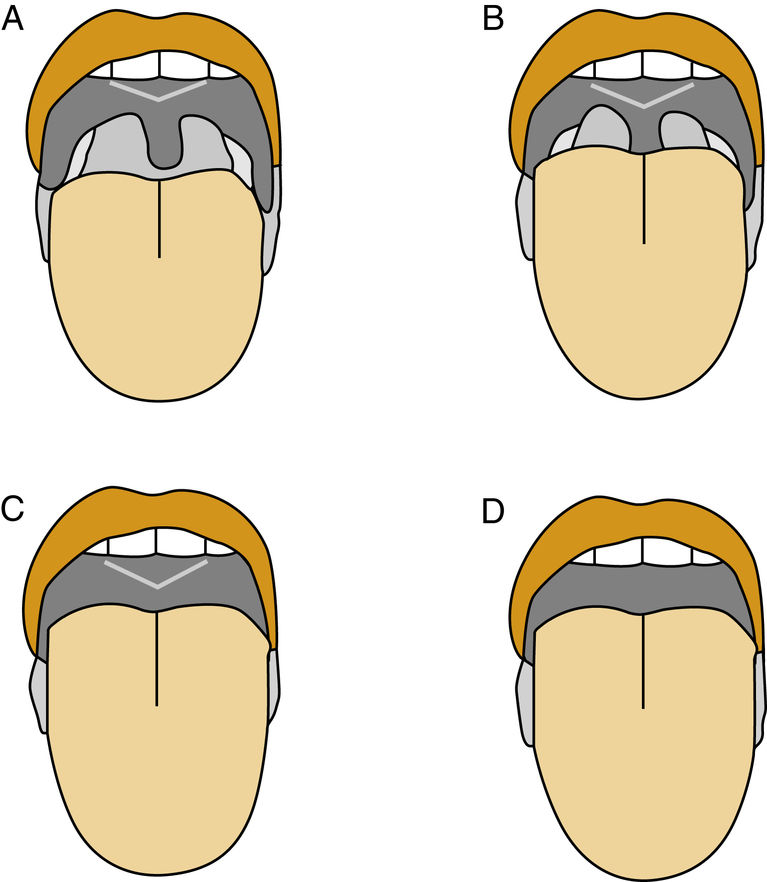
FIGURE 9.3 Modified Mallampati Palate Position.
(A) The entire uvula can be seen with the tongue at rest. (B) A partial view of the uvula is seen. (C) Only the soft and hard palate can be seen. (D) Only the hard palate can be seen. (From Flint PW, Haughey BH, Lund VJ, et al. Cummings Otolaryngology—Head and Neck Surgery. 6th ed. Philadelphia, PA: Saunders; 2015, fig.18-12.)
Tonsil Evaluation
• 1: 0-25% lateral narrowing of oropharynx (in tonsillar fossa)
• 2: 25-50% lateral narrowing of oropharynx (fills fossa)
• 3: 50-75% lateral narrowing of oropharynx (extends beyond fossa)
• 4+: >75% lateral narrowing of oropharynx (touching tonsils)
Evaluation of Retrognathia
• Frankfurt plane
• Line bisecting vermilion border of the lower lip with the pogonion should be perpendicular to the Frankfurt plane
Mallampati Score (Fig. 9.3)
• Class I: full view of the uvula and tonsils
• Class II: partial view of tonsils
• Class III: soft palate edge but the uvula is not visible
• Class IV: soft palate is not visible
Obstructive Sleep Apnea Syndrome Tests
• Drug-induced sleep endoscopy
• Polysomnography
• Lateral cephalometric analysis
• Subjective sleep questionnaires
Polysomnography Parameters
• EEG
• Electrooculum (EOG)
• Electromyogram (EMG)
• Electrocardiogram (ECG)
• Oronasal airflow
• Respiratory effort
• Oximetry
• Vital signs
• Snoring volume



