Purpose
To describe a series of 4 patients with Waldenström macroglobulinemia and serous macular detachment, and propose a mechanism for development of subretinal fluid based on optical coherence tomography (OCT) findings.
Design
Retrospective observational case series.
Methods
The records of patients with Waldenström macroglobulinemia and OCT documentation of serous macular detachment at Wills Eye Institute were reviewed. Data collection included clinical examination, as well as findings on fluorescein angiography (FA) and OCT.
Results
Four patients (8 eyes) with Waldenström macroglobulinemia and serous retinal detachment were identified. All eyes had varying degrees of venous stasis retinopathy and intraretinal edema overlying the macular detachment. Three patients had no FA leakage, while 1 patient had macular leakage in a petaloid pattern. Focal outer retinal defects within the detached retina were seen in 4 eyes on OCT imaging. In one eye, development of cystoid macular edema was observed before the outer retinal defect and serous macular detachment. All patients with serous macular detachment had some degree of outer retinal disruption.
Conclusion
Discontinuity of the outer retina within the macular detachment may enable immunoglobulins along with accumulated intraretinal fluid to flow into the subretinal space, creating a serous retinal detachment. Even with systemic treatment of the underlying Waldenström macroglobulinemia, the visual prognosis was guarded.
Waldenström macroglobulinemia is a malignant lymphoproliferative B-cell disorder. Although most common signs and symptoms of this neoplasm occur secondary to organ and bone marrow infiltration, overproduction of monoclonal immunoglobulin type M (IgM) is the most distinguishing feature. As IgM is a large pentamer compound that easily forms aggregates, high levels lead to blood hyperviscosity. Higher serum viscosity is also attributable to rouleaux formation, which occurs because cationic IgM molecules lower the repulsive forces between anionic erythrocytes. These unique molecular features of IgM lead to a constellation of clinical findings known as the hyperviscosity syndrome.
Hyperviscosity syndrome occurs in approximately 17% of all patients with Waldenström macroglobulinemia. The syndrome can have many manifestations, including constitutional symptoms, spontaneous bleeding, neurologic signs, cardiorespiratory distress, and vision loss. The most common retinal findings of hyperviscosity syndrome include scattered hemorrhages and microaneurysms, vascular dilation and tortuosity, venous beading, and optic disc edema. At the time of diagnosis, approximately 8% of patients with Waldenström macroglobulinemia report visual disturbance and 37% exhibit some degree of hyperviscosity-related retinopathy.
Rarely, patients with Waldenström macroglobulinemia and hyperviscosity-related retinopathy develop serous macular detachment. This condition has been previously described in case reports, 2 of which included time-domain optical coherence tomography (OCT) imaging. We report a series of 8 eyes of 4 patients with Waldenström macroglobulinemia and hyperviscosity syndrome who developed serous macular detachments, and propose a mechanism of the origin of the subretinal fluid based on spectral-domain OCT imaging.
Patients and Methods
The Institutional Review Board at Wills Eye Institute approved the retrospective analysis of data for this observational case series. The records of patients with a diagnosis of Waldenström macroglobulinemia who had OCT were reviewed. One patient who did not have serous retinal detachment in at least 1 eye was excluded. The following data were collected for each of the 4 relevant cases: Snellen visual acuity at presentation, sex, age, past medical history, signs of venous stasis retinopathy, extent of retinal detachment, presence of cystoid macular edema (CME), fluorescein angiography (FA) findings, treatment modalities, and final visual acuity.
Results
Patient 1
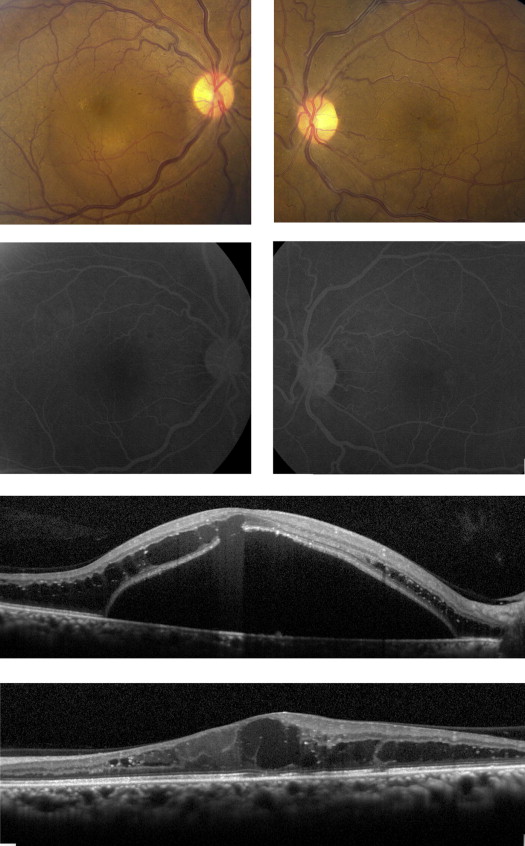
A 48-year-old African-American man presented with a 2-week history of decreased vision in the right eye. His medical history included hypertension, anemia, nephropathy, vitiligo, and non-Hodgkin lymphoma that underwent spontaneous remission. He had a bilateral nonischemic central retinal vein occlusion for which he never required treatment. At presentation to our institution, his best-corrected visual acuity was 20/400 in the right eye and 20/30 in the left eye, with no relative afferent pupillary defect. Slit-lamp biomicroscopy was remarkable for early cataract formation. Dilated funduscopic examination in both eyes revealed venous dilation and tortuosity with a few scattered hemorrhages and microaneurysms in the retinal periphery. The right eye had a 5 disc area shallow neurosensory detachment with fine yellow exudates and overlying CME ( Figure 1 , Top row right) and the left eye had diffuse CME ( Figure 1 , Top row left). FA showed no leakage in the right macula and trace late hyperfluorescence in the left eye ( Figure 1 , Second row) with a few microaneurysms in the midperiphery of both eyes. OCT of the right eye demonstrated a localized neurosensory detachment with disruption of the outer retina and edema overlying the area of detachment ( Figure 1 , Third row). The left eye showed diffuse cystoid spaces and focal disruption of the inner segment / outer segment junction, but no subretinal fluid ( Figure 1 , Bottom row).
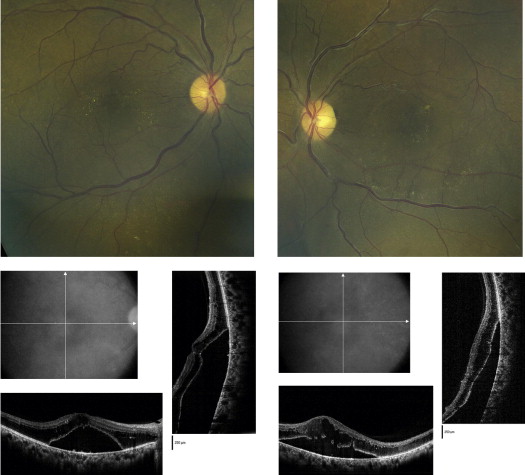
The patient’s blood pressure was 140/100. Laboratory evaluation revealed anemia with a hemoglobin of 11.6 g/dL and normal cortisol and adrenocorticotropic hormone (ACTH) levels. Serum protein electrophoresis (SPEP) was abnormal, with an elevated M (IgM) spike of 4500 mg/dL. Hematology consultation confirmed a diagnosis of Waldenström macroglobulinemia. One month after initial presentation, the vision in both eyes had decreased to count fingers. The neurosensory detachment in the right eye had increased in size and migrated inferiorly, and there was a new 4 disc area shallow neurosensory detachment in the left eye. The patient received plasmapheresis but refused the recommended systemic chemotherapy. Over the next 3 months, the subretinal fluid increased in both eyes and migrated inferiorly ( Figure 2 ). The patient was lost to follow-up.
Patient 2
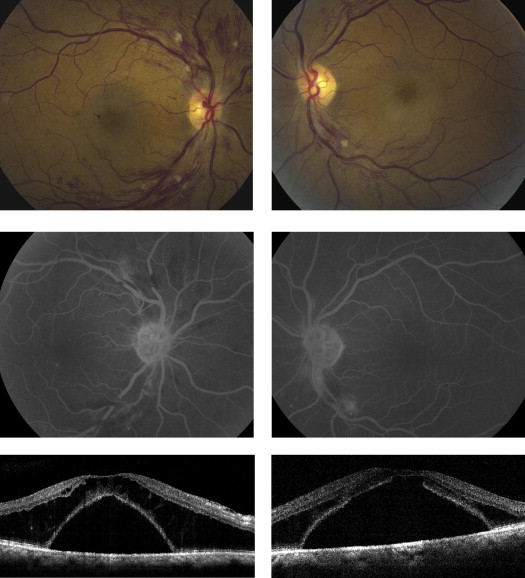
A 63-year-old African American man with a history of non-insulin-dependent diabetes mellitus and hypertension presented with a several-month history of progressive bilateral vision loss. Best-corrected visual acuity was 20/200 in both eyes, without relative afferent pupillary defect. Dilated funduscopic examination revealed mild bilateral optic disc edema, mildly tortuous veins, scattered intraretinal hemorrhages, occasional cotton-wool spots, and a 2 disc area shallow macular detachment with associated CME ( Figure 3 , Top row). Fluorescein angiography of both eyes showed a few scattered macular microaneurysms, but no significant leakage ( Figure 3 , Middle row). OCT demonstrated a bilateral localized neurosensory detachment with overlying intraretinal edema and a focal outer retinal disruption overlying the subretinal fluid ( Figure 3 , Bottom row).
The patient’s blood pressure was 145/90. Hemoglobin level was low at 9.2 g/dL. Fasting blood glucose and carotid Doppler ultrasonography were normal. SPEP revealed an abnormal elevated M (IgM) spike of 8434 mg/dL. The hematologist diagnosed the patient with Waldenström macroglobulinemia and started systemic treatment with plasmapheresis, bortezomib, dexamethasone, and rituximab. The patient experienced visual improvement shortly after starting treatment, and 5 months later his visual acuity had improved to 20/40 in the right eye and 20/70 in the left eye. The optic nerve edema, retinal hemorrhages, cotton-wool spots, and intraretinal edema all improved. However, the subretinal fluid worsened and migrated inferiorly. Yellow intraretinal exudates developed in the area of the macular detachment.
Patient 3
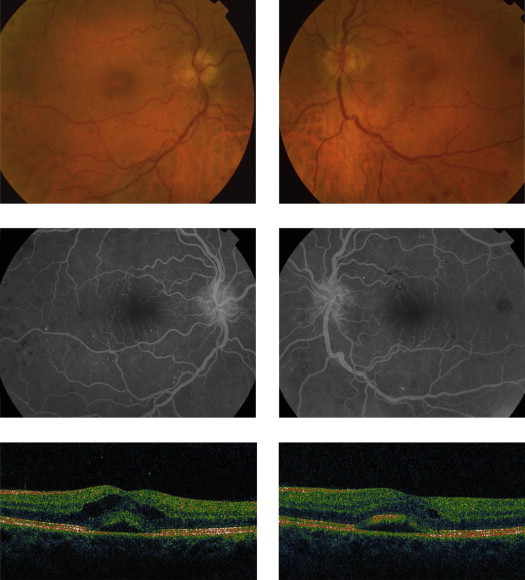
A 56-year-old white man with a medical history of vertigo and prostate cancer complained of mild fatigue as well as mild decreased vision in both eyes for several months prior to presentation. Best-corrected visual acuity was 20/25 in the right eye and 20/20 in the left eye, without relative afferent pupillary defect. Dilated funduscopic examination revealed bilateral dilated tortuous veins and arteries, scattered intraretinal hemorrhages, mild optic nerve edema, and mild CME overlying a small 0.33 disc area foveal neurosensory detachment ( Figure 4 , Top row). FA showed bilateral microaneurysms most prominent in the midperiphery ( Figure 4 , Middle row). OCT demonstrated mild intraretinal edema and a small area of subfoveal fluid in each eye ( Figure 4 , Bottom row).
The patient’s blood pressure was 110/70. Systemic evaluation revealed mild anemia, normal fasting blood glucose, and no carotid stenosis. SPEP was abnormal, with an elevated M (IgM) spike of 6200 mg/dL. Hematology consultation confirmed a diagnosis of Waldenström macroglobulinemia and he started plasmapheresis and a chemotherapy regimen of bortezomib, dexamethasone, and rituximab. After 5 months of treatment, his visual acuity returned to 20/20 in both eyes, the intraretinal edema and neurosensory detachment completely resolved, and the vascular tortuosity and hemorrhages were markedly improved.
Patient 4
A 72-year-old white woman with a history of hypertension presented with decreased vision in both eyes. Best-corrected visual acuity was 20/60 in the right eye and 20/200 in the left eye, without a relative afferent pupillary defect. Dilated funduscopic examination revealed bilateral CME overlying a 0.5 disc area serous macular detachment. FA showed late hyperfluorescence in a petaloid pattern in both eyes. OCT demonstrated bilateral CME with a focal neurosensory macular detachment.
The patient was diagnosed with Waldenström macroglobulinemia 5 years prior to her retinal evaluation and she had responded well to treatment with rituximab. At that time, she had CME for which she received numerous intravitreal triamcinolone acetonide injections. These injections helped her vision, but she required retreatment every 4 to 6 months over a period of 6 years. Her visual acuity fluctuated depending on the status of her CME and subretinal fluid. At her most recent follow-up, her vision was 20/30 in the right eye and 20/50 in the left eye.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


