Sensory Tests and Treatment of Binocular Vision Adaptations
Paul R. Mitchell
Marshall M. Parks
Before treatment of the sensory status in a strabismic patient, it must be diagnosed. Diagnosis of the binocular vision adaptations in strabismus is accomplished by observing the results of various tests presented to the patient.
SENSORY TESTS
WORTH 4-DOT TEST
One of the simpler methods for investigating fusion, suppression, and anomalous retinal correspondence (ARC) is the Worth 4-dot test. The testing target consists of four illuminated dots that are clustered equidistant from each other; two dots are green, one is red, and one is white. The patient views the target through anaglyphic testing glasses that consist of a red filter in front of one eye and a green filter in front of the other. Viewed through the red filter, the green dots are invisible; viewed through the green filter, the red dot is invisible. The white dot is seen as red when viewed through the red filter and as green when viewed through the green filter. The test subject monocularly sees two red dots through the red filter and three green dots through the green filter. Binocularly, however, the fusing subject perceives the target as four dots because the white dot is seen as either a single red or green dot, according to which eye is dominant. If the dominance pattern vacillates between the eyes, the white dot manifests color rivalry by changing from red to green.
The examiner must consider that the response of the patient may vary according to the size of the projection angle that the cluster of the four dots presents to the retinas. A normal subject possessing both macular and extramacular binocular vision perceives four dots, regardless how minute the projection angle that the target subtends on the retina. A patient devoid of macular binocular vision but who possesses extramacular normal binocular vision does not manifest fusion of the target (subtending an angle of about 3° or less) yet manifests a fusion response for larger targets.
Essentially, two methods of performing the test are available. One is to have a fixed target at a distance from the subject, which may either be contained in an illuminated box or projected on a screen. This is referred to as the distant Worth dot test. The other method is a near Worth dot test, which consists of a flashlight easily advanced or receded from the subject to alter the projection angle of the target image on the retinas. The latter can be accomplished with the fixed location of the distant Worth dot test by having the subject advance toward or recede from the target. At 6 meters, the distant Worth dots project an image of 1.25°; at 0.33 meters, the near Worth dots project a 6° angle (Fig. 1). The projection angle of the image is the imaginary circumference encircling the outer border of the four dots collectively, not simply the projection angle of each of the four dots. The subject should be tested with the optimal optical correction on (spectacles or contact lenses) behind the anaglyphic filters.
 Fig. 1. A. Distant Worth dots. B. Near Worth dots. C. Approaching near Worth dots. |
Monofixation syndrome patients have a 3° macular scotoma in the nonfixating eye (Fig. 2), which precludes a fusion response unless the projection size of the target image exceeds 3°. If the distant Worth dot test is 6 meters from the patient, it is not fused. By advancing toward the target, fusion is achieved at about 2.5 meters. Because the standard near Worth-dot flashlight projects 6° images at 0.33 meters, the test should begin about 2 meters from the patient. On advancing the target toward the patient, fusion is usually manifest at about 0.66 meters. Fusion response is lost by moving the flashlight away from the patient farther than 0.66 meters, and the patient sees either only two red or three green dots, according to which is the fixating eye. When this occurs, the examiner is inclined to state or to record this response as “suppression,” which it is not. The test result merely identifies the presence of the macular scotoma in the nonfixating eye of the monofixation syndrome patient. Whatever the cause of the macular scotoma in the monofixation syndrome patient—dissimilarity of macular images exceeding the threshold tolerated for macular fusion, an inherent inability to develop macular binocular vision (bifixation) despite having developed extramacular binocular vision, or a unilateral macular destructive disorder—it is not a scotoma generated by a cortical process to eliminate symptoms of diplopia and visual confusion, as encountered in strabismus. The latter is suppression. Its scotoma is displaced away from the macula in the nonfixating eye’s extramacular retina locus that receives the image projected onto the fixating eye’s macula. The suppression scotoma in the strabismic patient is larger than the macular scotoma in the monofixation syndrome patient. The suppression scotoma in the strabismic patient is associated with ARC, whereas the macular scotoma in the monofixation syndrome patient is associated with normal retinal correspondence (NRC). The strabismic patient manifesting a suppression scotoma does not have stereopsis. The suppression scotoma exists in the strabismic patient because the extramacular binocular vision reflex has the ability to adapt to any strabismic angle and continue to fuse by changing from its innate NRC to ARC plus, developing suppression. The macular binocular vision reflex is devoid of this attribute. The development of any deviation of the fixation axes of the eyes of more than 20 minutes of arc instantly causes the reflex to cease functioning, manifesting no annoying symptoms of diplopia and visual confusion but having no capacity to adapt to the strabismic deviation of the eyes and continue functioning.
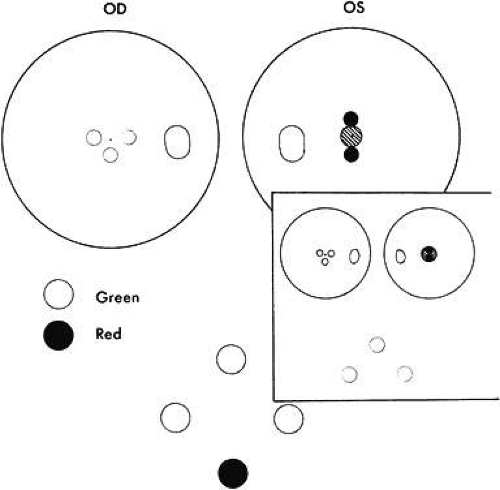 Fig. 2. Extramacular binocular vision with absence of macular binocular vision showing the left macular scotoma in a monofixating patient. Worth lights must project outside the scotoma to be fused. |
Strabismic patients who acquire deviation of 10Δ or more after having developed normal binocular vision reflexes have diplopic and visual confusion symptoms until extramacular binocular vision reflex converts from NRC to ARC. While still in NRC mode, the response to the Worth dot test is five lights (two red and three green). The dots seen by the fixating eye are clear, whereas those seen by the deviating eye are blurred. The blurred dots are projected in space opposite the direction of the deviated eye, causing homonymous diplopia in esotropia, heteronymous diplopia in exotropia. The dots seen by the hypertropic eye appear lower; those seen by the hypotropic eye appear higher. The image in the intorted eye appears extorted; that in the extorted eye appears intorted. Horizontal or vertical diplopia can be eliminated by the appropriate prism or prisms placed before the strabismic eyes but there is no prism correction that eliminates the torsional diplopia. As the ARC fusion mode gradually replaces the NRC fusion mode, the Worth-dot response becomes four lights—despite strabismic deviation. The projection angle on the cluster of dots, however, must exceed the size of the suppression scotoma that always accompanies ARC. The suppression scotoma is 5° or more in esotropia (Fig. 3) but larger in exotropia.
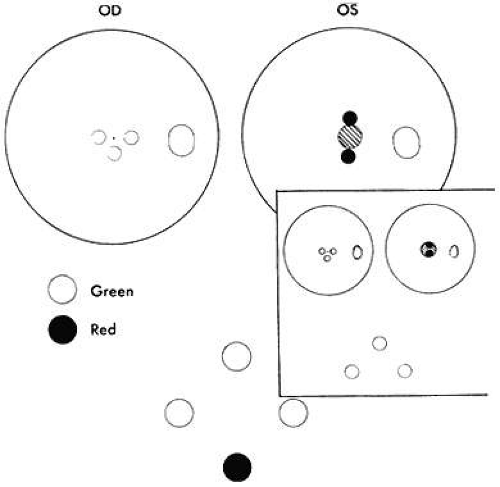 Fig. 3. As near Worth dots approach the esotropic patient, they become fusible when they first project outside the suppression scotoma. |
The esotrope’s suppression scotoma is usually overcome by advancing the near Worth-dot flashlight to about 40 cm from the eyes, with the patient at that time giving a fusion response. As the flashlight recedes beyond 40 cm, the cluster of dots project within the boundary of the suppression scotoma, and only those dots projecting into the fixating eye are seen. In exotropia, the suppression scotoma is larger and extends up to the hemiretinal line. Consequently, it is unusual to succeed in projecting the near Worth-dot flashlight cluster outside the large temporal retina scotoma. Hence, the test generally does not validate ARC in the exotropic patient because the fusion response is seldom obtainable. For this reason, the sensorial adaptations in the exotropic patient are better investigated by methods other than the Worth 4-dot test alone. For example, ARC in the exotropic patient during either near or distant Worth-dot testing may be revealed as the base-in prism power neutralizing the objective angle that is placed before the eyes. As soon as the cluster of dots is moved across the hemiretinal line and out of the temporal scotoma, homonymous diplopia is elicited despite the targets being projected on corresponding retinal areas. The patient sees the diplopic images as being separated by a considerable distance.
Absence of binocular vision is manifest in the esotropic patient when regardless how near the target to the eyes or how large the projection angle of the cluster of dots, the patient continues to see either three green or two red dots (Fig. 4). One precaution must be exercised by the examiner to guard against rapid alternation of the fixating eyes, which can produce a response of five dots because of summation of the three green dots seen by one eye and the two red dots seen by the other eye. The important question is whether the five lights are seen simultaneously or whether the patient is adding the separate responses?
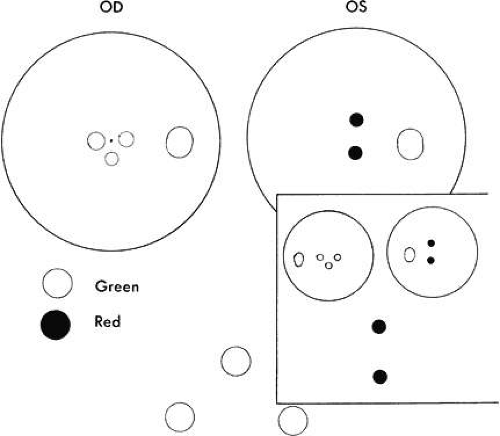 Fig. 4. If the near Worth dots are advanced to within 10 cm of the eyes of an esotropic patient having no single binocular vision, that patient reports seeing either three green or two red dots, never four. |
The Worth 4-dot test is simple enough to be performed on children who can count to five. If the visual acuity can be determined, so can the Worth 4-dot response. The test is performed with ordinary room illumination to provide the usual peripheral vision clues.
BAGOLINI STRIATED GLASSES TEST
Most tests for fusion, suppression, and ARC create artificial viewing circumstances. Normally, the visual environment is not that of a red filter in front of one eye or a combination of red-green filters; separately viewed slides in illuminated tubes are nothing more than a laboratory analysis of retinal correspondence. The striated glasses popularized by Bagolini, however, allow the patient to view the normal visual environment with a faint reference line placed on the background viewed by each eye (Fig. 5). The reference line for each eye is placed at right angles by arranging the glasses in the trial frame so that the striations before the right eye and the left eye are perpendicular to each other. For example, the striations are placed at 135° in the trial frame in front of the right eye and at 45° in front of the left eye. The patient views a fixation light at any distance the examiner chooses; ordinary room illumination is maintained. The patient reports on the fixation light and observed streaks extending out into the peripheral field of vision.
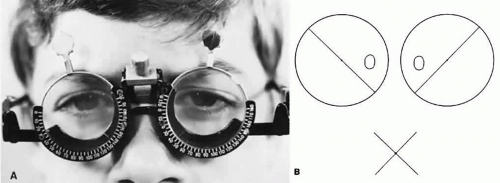 Fig. 5. A. Bagolini striated glasses. B. Simultaneous perception of opposite diagonal streaks projected onto opposite retinas by Bagolini striated glasses in a patient without strabismus. |
Patients with either straight eyes or with a deviation up to 8Δ by simultaneous prism and cover test and NRC binocular vision describe seeing one fixation light and two streaks forming an X intersecting at the light. The bifixating patient with macular fusion sees it as just described. If macular fusion is lacking although extramacular fusion is present, a gap of 3° is reported in one streak on either side of the light (Fig. 6). The gap represents the macular scotoma in the nonfixating eye of the monofixating patient. Monofixating patients are unaware of this gap in the one streak around the fixating light until the examiner questions them about it; they invariably seem to be oblivious to the presence of the scotoma until it is brought to their attention. When the fixating eye is covered, the gap in the streak disappears, and the entire streak then passes through the center of the fixation light. If the patient can switch fixation, the macular scotoma is observed to transfer from eye to eye.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


