16
Scary Monsters and Waterfalls: Tinnitus Narrative Therapy for Children
Stories are an integral part of young children’s lives. We work with the stories children and families tell us about tinnitus: their thoughts and feelings about it. We look at how tinnitus affects their life, and how life affects their tinnitus. Often their story is alive with negative connotations and emotions: tinnitus can be scary and frightening; tinnitus can be a monster. By changing children’s stories about tinnitus, we help them to see it in a new light. Monsters can be friendly too.
The child’s family will also have a story about tinnitus as they try to make sense of the child’s experience and the impact it has on their lives. Although this story may or may not be the same as the child’s, it will be equally alive. When the dominant story lies with the parents, this becomes the focus of intervention.
Stories about tinnitus are connected to the wider system around the child. Troublesome events in a child’s life, either at home or at school, can become attached to his or her story about tinnitus. Tinnitus can be seen as the cause of these difficulties or as a consequence.
Psychological work with children cannot be too prescriptive. Intervention must suit each child’s developmental level and follow a thorough assessment. Our intervention packages are tailored to the individual child and take account of the child’s age, audiological status, and life circumstances. Intervention may include individual therapy with the child, family, or school. We use a wide range of intervention strategies, including relaxation techniques and educational assessment. In this chapter, however, we have focused on therapeutic techniques for working with the preadolescent child. These techniques have developed from narrative therapy.
Children and Tinnitus
For many children, tinnitus may have been present from early on, the child only becoming aware of it in middle or late childhood when he or she is able to describe it and discovers that others do not have the same auditory experience (e.g., Tyler and Smith, 2002). Children tend not to complain of tinnitus, and when they do, they should be taken seriously.
Our earlier survey of children presenting with troublesome tinnitus (Kentish et al, 2000) indicated that the impact of tinnitus on children’s experience is similar to that in adults. Sleeping problems, listening and concentration difficulties, and anxiety are the main areas most affected by troublesome tinnitus. As with adults, children’s tinnitus is often exacerbated during times of stress and emotional difficulty.
Although there are well-developed techniques for working with adults, little attention has been paid to developing techniques for children. Inevitably, this is a more complex area. Interventions must match the age and cognitive ability of the child. Young children do not have all the cognitive sophistication required for cognitive-behavioral therapy. The ability to reflect on their cognitions and emotions does not develop until late childhood. Nevertheless, we assume many of the same principles: tinnitus is affected by thoughts and feelings. We work with these in a child-friendly manner because every child loves a good story.
What Is Narrative Therapy?
Humans are, and always have been, story makers. Stories are our most familiar means of communicating the meaning we find in our experiences. Each of us holds stories about ourselves that help us to make sense of our life experiences, and these in turn have the effect of filtering an individual’s experience, thereby selecting what information gets focused in or focused out (Sween, 1999). The narratives we hold about ourselves help us to make sense of what happens to us. For each of us, our lives will be defined by how we respond to the experiences in our lives, as much as by the experiences themselves.
By looking at the stories and meanings associated with tinnitus, narrative therapy helps us start to disentangle why it is that for some children and families, tinnitus becomes problematic, and for others it is a matter of little or no consequence.
Stories about tinnitus held by children and families will in part be construed from their own personal experiences, but they will also be gained from the wider system within which they live. These influences include
• The society within which the child lives (e.g., political and medical). Within the child’s society are commonly held beliefs about tinnitus that the child and family may have heard from health, media, deafness, or hearing groups. These beliefs can have a powerful influence on how the family approaches tinnitus. Such beliefs may be that tinnitus is only associated with hearing loss, that it does not occur in children, and that it is a permanent or untreatable condition.
• Community, school, and friends. If we look at community, school, and friends, we can see that meanings and beliefs from these will be important in shaping the families ideas about childhood tinnitus. A teacher, for example, who has personal experience of tinnitus will respond to a child’s tinnitus quite differently from one who knows little about it.
• Family and siblings. Family stories about illness, hearing impairment, and hospitals will have a bearing on how treatment is approached. For example, whether a family believes the child and feels that the tinnitus is important will affect the interactions among the family and child.
Children are influenced by the meanings and beliefs conveyed by the wider system around them, and even very young children will pick up their parents’ responses to illness, hospitals, and tinnitus. A commonly held view is that talking to a child about tinnitus may make it worse. A tinnitus consultation may therefore be the first time that a child has been allowed to voice his or her concerns in a developmentally manageable way.
Unique Outcomes
During the process of assessment, we aim to bring into the open the stories about tinnitus that are held by the child and family. When tinnitus is troublesome, these stories will inevitably be problem filled. We are listening, however, for examples of situations that contradict these dominant, problem-filled stories, and so bring to mind other, problem-free stories. For instance, a child may hold a story that “tinnitus always keeps me awake at night.” Always? If the child and family can think of a time when the child did get to sleep, even when the tinnitus was noisy, then we have begun to explore with them a new and different story that “tinnitus stops you from sleeping.” In narrative therapy these situations are called unique outcomes (White, 1988).
Mapping the Influence of Tinnitus
Tinnitus can have a significant effect on a child’s life, and its presence will inevitably affect the family also. No parent remains unaffected by seeing his or her child seemingly in pain and distressed. Difficulties listening in school and getting to sleep at night are often mentioned effects of tinnitus. Other difficulties in life, however, that may not be a direct outcome of tinnitus can also become connected, or mapped onto the tinnitus. A child who is having difficulties making friendships may believe that it is because of tinnitus.
Case Example: Trouble at home Ten-year-old Susie had tinnitus for as long as she could remember. Over the past year, however, it had gradually worsened. Rarely present at school, it occurred most evenings at home. Susie’s mother was worried about talking to her about the tinnitus for fear of making it worse. Instead, she would try to distract her daughter by playing with her, or reading to her, often long into the night. Susie identified loud noises as triggering her tinnitus, and therefore the rest of the family was instructed to keep as quiet as possible. In particular, Susie identified arguments between Susie’s father and her teenage brother as being the main influence on her tinnitus. They frightened and worried her. Susie’s brother, however, was fed up with the limitations placed upon family life by Susie’s tinnitus. As psychologists we can see that Susie’s story about tinnitus was that it prevented family arguments. For her brother, tinnitus was sometimes the source.
Externalizing
Narrative therapy holds the view that “the person is never the problem; the problem is the problem” (Sween, 1999, p. 191). When people see a problem as an integral part of themselves, it is difficult for them to change, or to believe that things can be different. We can see how tinnitus, by its very nature, can easily be seen as an integral part of oneself, and hard to change.
Externalizing is a process of helping the person to separate from the problem, and to see the problem (tinnitus) as something outside and separate from the person. This process of separation from the problem also helps relieve the person from all the negative thoughts, feelings, and ideas about tinnitus from which he or she has become inextricably linked. White (1988) noted that, among other things, it helps to decrease conflict and reduce feelings of failure and stress.
Thus, when we work with children in this way, we describe the tinnitus or problem in the third person; it is no longer ascribed to a person or relationship. In this way we do not say “your tinnitus” but “the tinnitus.” Care is taken not to use labels or diagnoses because they internalize rather than externalize the problem. With younger children we would use the name that the child uses (e.g., one child named his tinnitus noises “boum boums”). By taking the problem outside the person, it means that we can have an influence on it, and it does not add to an experience of helplessness.
Using externalizing as a technique for children allows us to introduce a more lighthearted and playful approach to therapy. The child can be invited to draw the problem (tinnitus), thus creating a depiction of the problem that can be looked at from outside the child. A soft toy also can be used to represent the tinnitus. The toy can be looked at and talked to, and new and different relationships can be explored with the tinnitus. For adults, such blurring of reality and imagination may seem strange or uncomfortable. However, we are entering into the playful and imaginative world of the child. For the child, externalization is like playing a game of “pretend.” Implicitly, or even explicitly, we are saying to the child, “Let’s pretend the problem is outside you, and we will play with it from there” (Sween, 1999).
Interviewing the Young Child
With young children, it is important not to apply the “child as a small adult” way of thinking. Developmental change is extensive within childhood. The child’s level of language and cognitive and social development will affect his or her understanding of tinnitus, as well as the ability to describe it and to participate in different kinds of treatment.
Research on children’s pain suggests that by around 7 years of age, children can give reasonably sophisticated descriptions of their pain. However, concepts of pain are qualitatively different. Adult-like (abstract and complex) understanding of illness does not occur until adolescence. The child’s cognitive and developmental status will influence the level of sophistication of illness concepts and pain-related beliefs (Siegel and Smith, 1989). Children may generate their own hypotheses and explanations for the causes of their pain or illness, in the absence of information that is complete, or given at a developmentally appropriate level (Bush, 1987). Children will thus construct their own “stories” to account for their tinnitus.
To understand the child’s story about tinnitus, we need information about the tinnitus, which is gathered in a child-friendly and developmentally appropriate way. This process cannot be hurried. Time spent in playing and drawing at the initial interview will help the child feel comfortable and at ease in a new and strange environment. Play and drawing are also useful ways for young children to depict their ideas and feelings about tinnitus, particularly when language skills are limited. Most children enjoy drawing. A picture of what tinnitus looks like can be highly revealing and a useful starting point to the process of externalization.
Many health care professionals often adopt a closed form of questioning, requiring a yes/no form of answer. Indeed it has been shown that young children will often answer a nonsense question when presented in a closed format (e.g., “Is a jumper angrier than a tree?”). Children will often try to please adults by providing the answer they think the adult wants to hear. However, we know from studies that children generate more information from open-ended questions (Waterman et al, 2001).
A young child may not be able to describe the tinnitus in a temporal way. Frequency and duration are hard for the young child to assess. This information does need to be gathered, and it is best done through a recording chart over a period of time. Younger children are less able to link tinnitus to events or internal cognitions (e.g., how it made them feel) or their mood. As part of ongoing therapy, these connections need to be taught through intervention or through observations.
Clinical Protocol
Assessment
INFORMATION GATHERING
Information is gathered about the child’s tinnitus through multiple methods. Prior to the first appointment, the school is contacted for information about the child’s educational progress, friendships, or any other difficulties noted by the child’s teacher (s). Parents are sent the Tinnitus Parents’ Questionnaire, which the authors devised, which begins to focus on their understanding of the child’s tinnitus and the factors contributing to it (Fig. 16–1).
By the end of the initial assessment we should be able to answer the following questions.
Background Information
• Can we describe the child’s tinnitus (e.g., frequency, times of the day when it is most likely to occur)?
• Are there other associated health and psychological problems (headaches, dizziness, hyperacusis)?
The Influence of Tinnitus upon Life
• How does the tinnitus influence the child’s daily life (e.g., sleep difficulties, anxiety, depression)?
• Does the tinnitus influence the child’s school life (e.g., difficulties listening or concentrating in class)?
• How does the tinnitus influence friendships and family?
The Influence of Life on Tinnitus
• Are there current life events that have influenced tinnitus (e.g., family or school difficulties)?
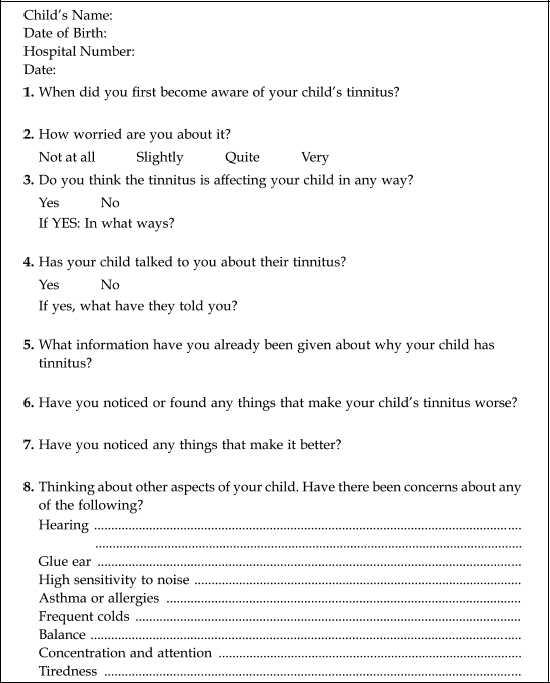
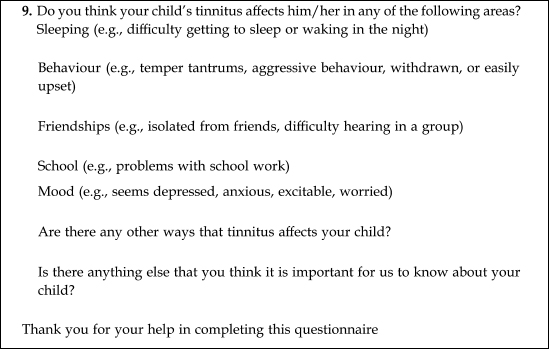
Figure 16–1 Tinnitus Parents Questionnaire.
The Tinnitus Story
• What do the child, family, and teacher know about tinnitus? How correct is this information?
• What are the beliefs within the family about the child’s tinnitus (e.g., the child is going deaf; the child has a brain tumor)?
• Who in the family is most worried about the child’s tinnitus (e.g., parent or child)?
• What stories does the family have about illness, hospitals, and hearing loss?
Unique Outcomes
• Can we identify situations or thoughts that contradict the dominant tinnitus story?
• Coping strategies: What has the child tried to do already to alleviate the tinnitus? Has this been successful?
• What have the parents tried to do to help the child? What effect has this had?
The Initial Interview
At the initial interview, all the family are invited to the appointment, but usually the parent(s) and child are seen together. The child and the therapist complete a questionnaire that the authors devised called Tinnitus and Me (Fig. 16–2). This relates to the questions outlined earlier in the section Information Gathering. The child is encouraged to personalize the booklet with coloring and drawings. The booklet is used as a guide only, and questions are adapted to suit the level of the child. This booklet serves the function of gathering information about the child’s understanding of tinnitus and hearing, as well as factors that influence them.
Past and present strategies for managing the child’s tinnitus are explored in the booklet. This is an important part of the assessment. Identifying strategies that have alleviated the tinnitus begins the process of changing the dominant story about tinnitus; the child and parent can begin to see that tinnitus is not something to be just passively endured.
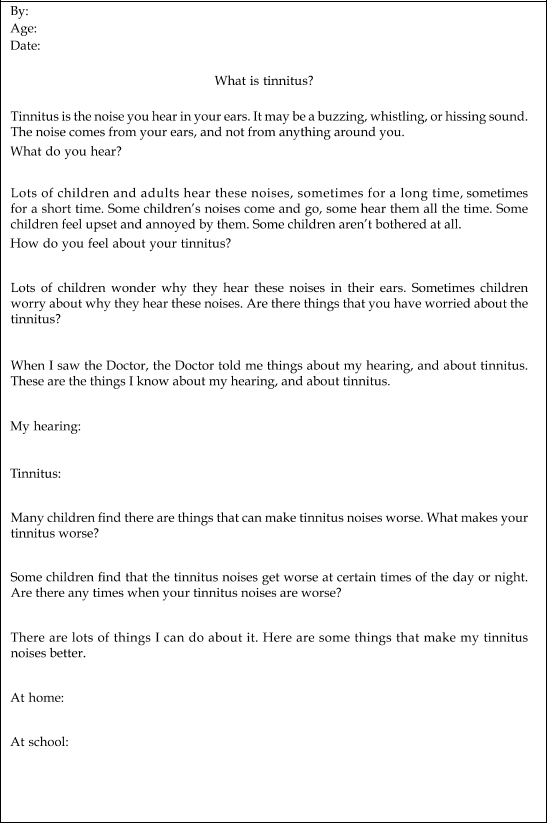
Figure 16–2 Tinnitus and Me Child Questionnaire.
Formal measures of anxiety and depression also can be used. If necessary, the therapist will go through this with the child, depending on his or her age.
The remainder of the interview is used to map the influence of tinnitus on the child, and vice versa. We explore with the child and parent other events in the child’s life. We are interested to know why the child’s tinnitus has become troublesome at this point in time, and whether there are particular events either at home or at school that may be affecting the child. Common events include school examinations, difficulty getting along with the teacher, and difficulties with academic work; and at home, marital or other family difficulties, health problems in another family member, or bereavement.
Intervention
Next, we begin to unpack the tinnitus story. For each child and family, the dominant story may lie in one or all of the areas already described. Through assessment, we will have determined where intervention needs to be focused.
1. Fears and worries about tinnitus: information about tinnitus
2. Life stressors linked to tinnitus
3. Individual work with the child: externalization and visual imagery
FEARS AND WORRIES ABOUT TINNITUS
Providing the child and parents with factual information about tinnitus is often the first major turning point. This begins to answer worries such as: is my child going deaf? Negative beliefs and feelings of hopelessness are a common part of the story (e.g., “I will always have tinnitus and there is nothing I can do about it”). This may have been engendered by parts of the child’s system including medical professionals, as in the example of David.
Case Example: A story of fear Nine-year-old David had a mild to moderate hearing loss. Due to an ear infection, he was prescribed a course of antibiotics from his medical practitioner. Although the ear infection cleared up, David developed a buzzing in both of his ears. Shortly after, his ear, nose and throat surgeon diagnosed tinnitus. He and his mother were told that there was nothing that could be done about it, and he must “go away and learn to live with it.” This devastated David and his mother. Over the forthcoming weeks he became increasingly distressed, then stopped sleeping and attending school.
Sadly, David’s story is not uncommon. Information about tinnitus began to focus on changing the story for David and his mother. First, they were reassured that there was much that could be done to help with the tinnitus. Changing this aspect of the story had a powerful effect for David and gave a story of hope.
LIFE STRESSORS LINKED TO TINNITUS
If there is an obvious association between an external life event and onset of troublesome tinnitus, then this will clearly need to be addressed, as will any educational or family difficulties.
INDIVIDUAL THERAPY WITH THE CHILD
Through discussion and play, we aim to find out, first, what the child’s tinnitus sounds like to the child, how it makes the child feel, and any images it conjures up for him or her. Second, we ask the child to generate characters or images that will help him or her to see tinnitus in a different way and give the child a sense of being in control. During the interview with the child we are observing closely the child’s response to various activities to see which works best.
1. The word tinnitus may be new to the child, so we first find out whether the child already has a name for it. If not, we ask the child what he or she would like to call it, and stick to that.
2. We ask the child to draw a picture of tinnitus. For those keen on drawing, this will be both pleasurable and engaging, and often works well with the older child.
3. We invite the child to play with a collection of toys. Depending on the age of the child, toys will include soft toys, miniature people, Lego pieces, and the latest cartoon and Disney characters. We also have a collection of less friendly-looking toys (our “monster” collection).
4. Side-by-side seating is less threatening. Young children rarely respond well to adult-style interviews.
5. We ask the child about activities that he or she enjoys doing at home, whether he or she has a favorite cartoon or superhero. We are looking for strong, powerful images for the child to use for support.
6. From Tinnitus and Me Questionnaire (Fig 16–2), we will already have some information about how often the child is affected by tinnitus, times of day and places it occurs most often, and feelings associated with it. We are now also interested in any visual images associated with it, both negative and positive. If images are strong, then the use of visual imagery techniques is indicated in intervention.
Through this process, we will have discovered whether the child works best through play, drawing, visual imagery, or a combination. The following case examples are used to show how we have used these to change children’s stories about tinnitus.
Case Example: Scary monsters Seven-year-old Hannah had a past history of intermittent conductive hearing loss and eustachian tube dysfunction. She was troubled by intermittent tinnitus, which occurred both at school and at home. Hannah described difficulties listening in the classroom and keeping up with schoolwork. She was also distressed by her lack of friends and was verbally teased at school. Both Hannah and her mother shared the belief that these difficulties had arisen as a result of the tinnitus. Hannah’s teacher was surprised by her concerns, reporting that her schoolwork was average, but acknowledged Hannah’s lack of friends.
Hannah was invited to play with our collection of soft toys. Talking as she played, it became clear that Hannah believed that the noises were caused by having a monster in her head. This was very scary for her and was getting in the way of her concentration, listening, schoolwork, and friendships. Hannah selected a soft toy that she felt resembled her “monster,” and we seated this on the table in front of us. We used externalization techniques to think about the monster, what it was like, and to think of any times when the monster was not scary. We explained to Hannah what tinnitus was, and that there was not a real monster in her head; however, the noise at times might be so unpleasant that it seemed there was a monster there. Hannah was invited to talk to the monster and to ask the monster to be her friend. Hannah gave the monster a name, and we were able to use the monster to fight the tinnitus noises. We thought about special powers that the monster might have, and how she might be able to get the monster to fight off the scary noises. This new story about the monster gave Hannah control over the scary noises.
For Hannah, the tinnitus noises were clearly scary. Furthermore, both Hannah and her mother believed that tinnitus was the cause of her other difficulties. By changing tinnitus into something more friendly and supportive, we were able to give Hannah a sense of power and influence over the tinnitus. Further sessions focused on helping Hannah address the separate difficulties she had with friendships and schoolwork.
Case Example: Waterfalls Sophie, age 11, was referred with troublesome tinnitus that caused sleep problems and interrupted her education. She was profoundly deaf following meningitis and communicated orally via lip reading.
Night was worse for Sophie, after she took her hearing aids out. She described the tinnitus as sounding like “a telephone ringing nonstop,” also like traffic, beeps, and wind. Sometimes she had more than one sound at a time. She could not predict when it would get louder or “worse.” Sophie had learned to distract herself from the constant tinnitus noises by doing exercises, or “keeping busy.” At night she would read and “think good things,” and take her cats to bed to help her to sleep. The tinnitus would be there the moment she woke up, and she told me that she just wanted to be “normal,” and to know if it would go away when she got older.
At times she felt tense and anxious, so we practiced some relaxation techniques that could be used at any time of the day. We talked about the sounds of the tinnitus, discussing more fully the “wind” sound. We elaborated a story about trees and a river that she could think about when the tinnitus became troublesome. Sophie clearly enjoyed nature, and this conversation led to her telling me that she was going away camping soon after this meeting.
On her return a month later, Sophie told me that the tinnitus now reminded her of water and a beautiful place where she had camped near a waterfall. She said that by recalling this, although still present, her tinnitus was now no longer distressing.
Here, Sophie’s dominant story is of tinnitus as being an unpleasant and intrusive experience that must be endured. The tinnitus made her feel different from other people, and she feared that it would never change. However, an exception to this story was her pleasant image of tinnitus as wind, which she did not find intrusive. This allowed us to develop another story in which control and calm were present. For Sophie this came from her camping experience. Tinnitus could become a waterfall and a pleasant place to be, rather than feared. The conversations previously had allowed her to find a way of understanding the tinnitus noises, and she had been able to adapt her thoughts about the “wind” noise into something that recalled a pleasant experience. By relating the story about the waterfall, she was able to depict herself as strong and able to succeed over the tinnitus. She was able to take responsibility in changing the perception of tinnitus.
Case Example: Superman to the rescue Nine-year-old Robert had tinnitus for as long as his mother could remember, but over the past few months it had become worse. He developed difficulties in getting to sleep and complained that he could not hear in class when his tinnitus was loud. His mother was concerned about his literacy difficulties and felt that he was finding school quite stressful. She described Robert as an anxious child and a worrier. Robert and his mother both feared that his worsening tinnitus might indicate that he was losing his hearing.
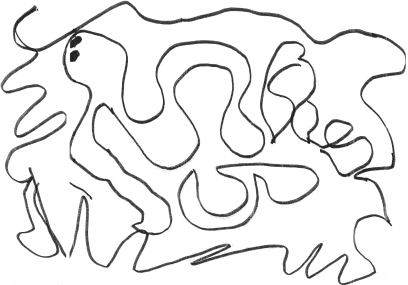
Figure 16–3 Robert’s depiction of tinnitus, the “Tin-monster.”
Robert enjoyed drawing, and with great enthusiasm he drew a picture of the tinnitus, which he depicted as a squiggly, snake-like creature. He called it Tin-monster (Fig. 16–3). He said that he felt afraid of the tinnitus, which would sneak up on him during lesson time at school and worm its way into his head through his ears. When not in his head, it would hide in the classroom, waiting for its moment to jump out at Robert.
Robert wanted to create his own character to support him in his fight against the Tin-monster. With great enthusiasm, he set about drawing a picture of Tin-man. An equally scary-looking creature, Tin-man was laden with all sorts of weapons that he could use to fight Tin-monster. Robert talked as he drew, and it was clear that his character was coming very much alive for him.
At the next session, Robert said that there had been several battles between Tin-monster and Tin-man. After each battle, Tin-monster had become a little weaker. He added some more weapons to his picture of Tin-man (Fig. 16–4). Robert’s general demeanor seemed brighter and stronger. He was also beginning to sleep better. Clearly, he was beginning to feel in charge.

Figure 16–4 Robert’s drawing of the “Tin-man.”
Over the course of further sessions we talked about worries held by both Robert and his mother about Robert’s hearing and tinnitus. It also became apparent that Robert’s class was particularly noisy, in part accounting for his difficulties in listening. Robert’s mother discussed this with his class teacher, and with various changes, this improved also.
In this situation, drawing proved the most useful technique for helping to externalize the tinnitus. Through the support of his powerful new ally, Tin-man, Robert began to develop a new story about himself, a story in which he saw himself as being more powerful.
Conclusion
Intervention for children with tinnitus is highly effective, and we often see a dramatic difference within a few sessions. We focus on stories: the meanings, beliefs, and emotions children and families have about tinnitus. These stories are in part acquired through the wider context around them: from the media, teachers, medical professionals, audiologists, and friends. Families will bring their own stories about illness and hospitals that influence how they cope with tinnitus in the child. Families will also have stories about how they respond to the difficulties that life has sent their way—whether they see themselves as helpless victims or as a family who can rise to a challenge. These stories are highly complex.
We aim to bring to light the dominant stories that influence the child’s and families’ response to tinnitus. Young children will attempt to make sense of their tinnitus, and if adults fail to talk with them openly about tinnitus at their developmental level, they will construct their own explanation. Tinnitus really can be a monster.
We use externalization techniques to help children separate from their problem. Through drawing, play, and discussion, we learn their view of tinnitus. Once tinnitus is out in the open, we can then begin to construct a new and different story about it. This will include factually correct information about tinnitus and powerful new images of coping and of influence over tinnitus. As psychologists, we help separate the real impact of tinnitus on children’s lives from those that become associated with it. Not all problems in life are due to tinnitus.
References
Aus G. Tinnitus in childhood. Int Tinnitus J 2002;8:20–26
Bush JP. Pain in children: a review of the literature from a developmental perspective. Psychol Health 1987;1:215–236
Kentish R, Crocker S, McKenna L. Children’s experience of tinnitus: a preliminary survey of children presenting to a psychology department. Br J Audiol 2000;34:335–340
Siegel LJ, Smith K. Children’s strategies for coping with pain. Paediatrician 1989;16:110–118
Sween E. The one-minute question: what is narrative therapy? Some working answers. In: Denborough D, White C, eds. Extending Narrative Therapy: A Collection of Practice-Based Papers. Adelaide, South Australia: Dulwich Centre Publications; 1999:191–194
Tyler RS, Smith RJ. Management of tinnitus in children. In: Newton VE, ed. Paediatric Audiological Medicine. Philadelphia: Whurr Publishers; 2002:397–404
Waterman A, Blades M, Spencer C. Is a jumper angrier than a tree? The Psychologist 2001;14:274–277
White M. The externalising of the problem and the re-authoring of lives and relationships. Adelaide, South Australia: Dulwich Centre Publications; newsletter 1988:5–28
< div class='tao-gold-member'>



