Saccadic Velocity Measurements in Strabismus
Henry S. Metz
A typical evaluation of patients with strabismus includes a measurement of muscle balance at distance and near fixation, as well as an evaluation of ocular rotations and the deviation in the nine cardinal positions of gaze. An array of sensory tests can provide useful and interesting information. Forced traction testing (under anesthesia in pediatric patients or in an outpatient setting in teenagers and adults) and active force generation testing in cooperative subjects are also of value.
When ocular electromyography became available, it became possible to study the co-firing and reciprocal innervation of the extraocular muscles. Normal muscle firing patterns could be compared with those of paralytic muscles, and recovery could be documented. However, ocular electromyography was available at only a few centers, required sophisticated equipment, and was not applicable to pediatric patients because of discomfort and inability to cooperate sufficiently for the study. An objective test that could provide information about the strength of an extraocular muscle yet be relatively simple, inexpensive, safe, and able to be performed on patients of all ages would be a useful addition to the evaluation of patients with strabismus, providing information to assist in diagnosis and to aid in management decisions.
Direct measurements of muscle force are difficult to perform quantitatively and are usually not possible in the pediatric age group. However, eye movements can be measured relatively easily and accurately with equipment available in many hospitals and medical centers.
The term saccadic movement applies to the rapid changes in eye position typically found between fixational pauses during reading.1 Movements constituting the fast phase of nystagmus were noted to have similar characteristics. Saccades have a latency of 150 to 200 milliseconds and, once started, cannot be stopped.2 Electromyographic recordings during a saccade show a large motor unit input.3
The velocity of a saccadic eye movement is related directly to the force produced by an extraocular muscle and thus is an indicator of the strength of a rectus muscle. A saccade also acts as a stress test because the muscle must function fully to produce a saccadic movement with a normal, rapid velocity.
Although eye movements can be measured by a number of techniques and devices,4 electro-oculography has proven to be a readily available, relatively simple technique that provides sufficient accuracy for clinical purposes. It has been known since the early 1920s that certain electrical changes are associated with eye movement. The eye has a standing electrical potential or charge across it, like a weak battery, with the front of the globe positive and the back negative. The resting or “standing potential” is generated largely by the transepithelial potential across the retinal pigment epithelium. It varies from one to several millivolts.5 With electrodes placed on both sides or above and below the eye, potentials indicating both horizontal and vertical eye movements may be recorded without interference to normal eye movements. The method is useful and convenient for recording rotations in the range of 0.5 to 40 degrees. The technique is linear over a segment of this range, and careful calibration can be used to determine the extent of large movements.
The technique of electro-oculography for saccadic velocity determinations is useful in infants and young children because head fixation is not required. Both average and peak velocities can be measured. Inspection of the eye position channel provides information about the amplitude of the saccade and the shape of the tracing. The peak velocity recording allows for an easy comparison between movements left and right or up and down.
Technique and Normal Values of Electro-Oculography
For horizontal saccades, miniature skin electrodes are placed on the skin just beside the medial and lateral canthi with the indifferent electrode on the brow (Fig. 21.1). Vertical saccades are recorded by placement of the electrodes centrally above the brow and on the lower eyelid, with the indifferent electrode temporal to the lateral canthus. The skin should be cleansed of oils or other debris with alcohol. Electrodes should be applied with a conductive paste. The electrodes are connected to an electro-oculography unit (Fig. 21.2) and display both an eye position and a peak velocity channel (Fig. 21.2). The original wave forms are displayed during the electro-oculography recording. This allows the examiner to observe whether there are artifacts, such as undershoots and overshoots, that would require repetition of the test to obtain more reliable results.
 Figure 21.1 Miniature electrode placement for measurement of horizontal (A) and vertical (B) saccades. Source: Metz HS: Saccadic velocity measurements in strabismus. Trans Am Ophthalmol Soc 81:630, 1983 |
 Figure 21.2 Electro-oculography unit. Source: Metz HS: Saccadic velocity measurements in strabismus. Trans Am Ophthalmol Soc 81:630, 1983 |
Saccades are usually generated by voluntary eye movements of 20 to 40 degrees across the primary position, either horizontally or vertically. In patients in whom paralysis or restriction prevent rotations of this size, the largest eye movements possible are recorded.
Calibration is performed by having the subject make a 20-degree saccade using the eye being studied for fixation. A bowl perimeter can be useful in quantifying the size of the saccade for calibration.
With infants and young children, saccades can be generated involuntarily by the use of optokinetic or vestibular nystagmus. The rapid recovery phase of nystagmus is a saccadic eye movement. A small, rotating drum or optokinetic nystagmus tape can be used to elicit optokinetic nystagmus, whereas spinning an infant in his mother’s arms can induce vestibular nystagmus. Normally rapid, recovery saccades of optokinetic nystagmus are shown in Fig. 21.3, whereas the slow recovery saccades produced by the lateral rectus muscle in a patient with sixth nerve palsy are shown in Fig. 21.4.
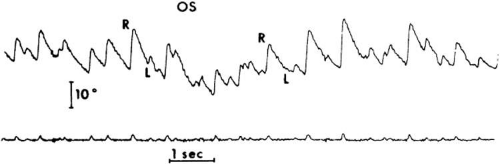 Figure 21.3 Electro-oculography recording of normal optokinetic nystagmus demonstrating rapid recovery phase. Upper tracing: eye position; lower tracing: peak velocity. Source: Metz HS, Scott AB, O’Meara D: Saccadic velocity in infants and children. Am J Ophthalmol 72:1130, 1971. Published with permission from the American Journal of Ophthalmology. Copyright by the Ophthalmic Publishing Company |
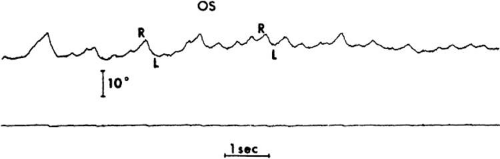 Figure 21.4 Electro-oculography recording of optokinetic nystagmus in a patient with sixth nerve palsy. Recovery saccades (L) are slow. Upper tracing: eye position; lower tracing: peak velocity. Source: Metz HS, Scott AB, O’Meara D: Saccadic velocity in infants and children. Am J Ophthalmol 72:1130, 1971. Published with permission from the American Journal of Ophthalmology. Copyright by the Ophthalmic Publishing Company |
To provide reliable calibration in very young patients, the child’s fixation with one eye can be obtained by showing a colorful, moving, noisy toy at a distance of one-third of a meter. A 10-Δ prism is introduced before the fixing eye, and the resulting horizontal eye movement is recorded by electro-oculography. The recorded eye movement can be used for calibration because the distance the eye moved is known.6
During the studies, it seems to make little difference whether the paretic or nonparetic eye is used for fixation, as long as equal amplitude saccades are used for comparison.7 For calibration purposes, however, the eye in which saccades are to be measured must be used for fixation.
Raab8 found peak saccadic velocity determinations for 20-degree saccades to be distributed normally and range from 281 to 541 degrees/second. He concluded that peak horizontal saccadic velocities of <300 degrees/second are likely to be abnormally slow using his equipment.
Other Methods of Measurement
Other methods of saccadic velocity measurement that are as accurate or more accurate than electro-oculography include infrared oculography, a magnetic search coil technique using a contact lens, and a video-based eye tracker.9 The infrared technique depends on the difference in the reflected infrared light from the cornea and sclera at the limbus but does not work well for measurements of vertical saccades. The search coil is difficult or not possible to use for clinical measurements in infants and young children. The video eye tracker is a high-resolution, noninvasive, user- and participant-friendly instrument with a linear range of 25 to 30 degrees. An excellent review of the advantages and disadvantages of these techniques was presented by Ygge at the Wenner-Gren Symposium in 1999.10
Direct observation of the speed of saccadic movements is easy to do but is less accurate. When saccades are very slow, as in the case of a complete paralysis of a rectus muscle, direct observation of the eye movements is both simple and accurate. Rosenberg11 commented that slight differences in saccadic velocities may be difficult for an untrained observer to identify. By using a + 14- or + 20-diopter lens over one or both eyes, velocity differences became more readily apparent because of the magnification of the high plus lens.
Extraocular Muscle Palsy
Sixth Nerve Palsy
The typical clinical picture of sixth nerve palsy is that of abduction deficiency with significant esotropia in primary gaze. Saccadic velocity, produced by the palsied lateral rectus muscle (toward abduction), can be compared with the speed of the movement toward adduction in the same eye (medial rectus function) and with abduction in the opposite eye (contralateral lateral rectus function) when the palsy is unilateral. The normal average saccadic velocity for a movement of 20 degrees or larger is usually between 200 and 320 degrees/second. Saccades produced by the palsied lateral rectus muscle vary from 40 degrees/second (Fig. 21.5) with complete paralysis to 160 degrees/second (Fig. 21.6) when only mild paresis is present.12 Recovery of the lateral rectus palsy can be documented by increased saccadic velocity with time.
 Figure 21.5 Electro-oculography recording of horizontal saccades with complete right lateral rectus paralysis. Abduction saccades (R) are very slow, whereas adduction saccades (L) are rapid. Source: Metz HS, Scott AB, O’Meara D et al: Ocular saccades in lateral rectus palsy. Arch Ophthalmol 84:453, 1970. Copyright 1984, American Medical Association |
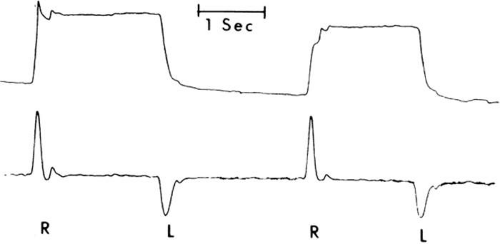 Figure 21.6 Electro-oculography recording of horizontal saccades with mild left lateral rectus palsy. Upper tracing: eye position. Abduction saccades (L) are mildly slowed, whereas adduction saccades (R) are rapid. Lower tracing: peak velocity. Source: Metz HS, Scott AB, O’Meara D et al: Ocular saccades in lateral rectus palsy. Arch Ophthalmol 84:453, 1970. Copyright 1984, American Medical Association |
In patients with marked or complete lateral rectus paralysis, visual observation of lateral saccades can reveal slowing. This slow movement is caused by relaxation of the antagonist medial rectus without active contraction of the lateral rectus muscle. When only mild to moderate lateral rectus palsy is present, eye movement recordings are needed to document the reduction in velocity.
Rosenbaum et al.13 used horizontal saccadic velocity measurements to determine whether transposition surgery with botulinum injection to the medial rectus was indicated in patients with sixth nerve paresis or paralysis. Only those patients with marked slowing of abduction saccadic velocity underwent this procedure.
Subjects are unable to alter saccadic velocity for a fixed-amplitude horizontal movement. Thus, slow saccades cannot be made voluntarily. A decrease in saccadic velocity is caused by an abnormality in the oculomotor apparatus.
Similar slowing of a saccade is noted following injection of Clostridium botulinum toxin into a rectus muscle. Velocity returns to normal in 4 to 6 weeks, when the effect of the toxin has worn off. Recovery from other causes of sixth nerve palsy can be similarly documented.
Sharpe et al.14 observed no recovery of saccadic velocity in chronic sixth nerve palsy of central origin, while in peripheral palsies, velocity improvement was noted. They suspect that speed is increased in this latter group secondary to remyelination and central monocular adaptation of innervation.
Third Nerve Palsy
Exotropia in primary gaze associated with limited adduction, elevation, and depression are the major clinical findings in third nerve palsy. Ptosis and a nonreactive pupil are also noted frequently. Adduction saccades in the affected eye vary from an average velocity of 30 to 175 degrees/second. Vertical saccades vary from 10 to 150 degrees/second, depending on the extent of the palsy. These slower velocities are probably due to the fact that some of the vertical saccades may be smaller than 20 degrees in amplitude because of significant weakness of both the superior and inferior rectus muscles.
After complete third nerve paralysis, the eye typically assumes a slightly hypotropic and markedly exotropic position. If this deviation persists, the lateral rectus and adjacent tissues usually become shortened and contractured, and nasal rotation of the globe also becomes mechanically limited. If medial rectus function recovers, nasal rotation will remain deficient because of lateral mechanical restrictions. Saccadic velocity studies can reveal the extent of recovery of the medial, superior, and inferior rectus muscles, even if rotations remain limited.
Superior Oblique Palsy
Although Rosenbaum et al.15 reported slowing of peak velocity of downward saccades in superior oblique palsy, this finding has not been confirmed.16 Even when measured with the involved eye in the adducted position, upward and downward saccades appear normally and equally rapid (Fig. 21.7). It would seem as if the diagnosis of fourth nerve palsy should be made on clinical grounds (e.g., small hypertropia, V pattern, antagonist inferior oblique overaction, positive Bielschowsky head tilt test, excyclotorsion) rather than on saccadic velocity measurements. Calculations of the superior oblique muscle’s contribution to downward gaze in adduction (only 18%) support the concept that saccadic velocity will be affected minimally by paresis of this muscle.17
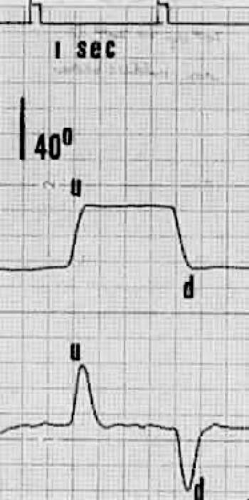 Figure 21.7 Electro-oculography of patient with superior oblique palsy. Both upward (U) and downward (D) saccades in adduction are normally rapid. Upper tracing: eye position; lower tracing: peak velocity. Source: Metz HS: Saccadic velocity studies in superior oblique palsy. Arch Ophthalmol 102:721, 1984. Copyright 1984, American Medical Association |
Duane Syndrome
In type I Duane syndrome (Huber’s classification), there is usually a small-angle esotropia or no deviation in primary gaze. Abduction shows marked limitation, whereas adduction is only mildly limited and is associated with retraction of the globe and oblique overaction. The average abduction saccadic velocity is usually quite slow, whereas the average adduction velocity is only moderately reduced18 (Fig. 21.8). This is due to the lack of lateral rectus firing on attempted abduction along with paradoxical innervation of the lateral rectus on attempted adduction. These findings clearly differentiate type I Duane syndrome from lateral rectus palsy. Because the approach to therapy differs significantly in these two conditions, these diagnoses must not be confused.
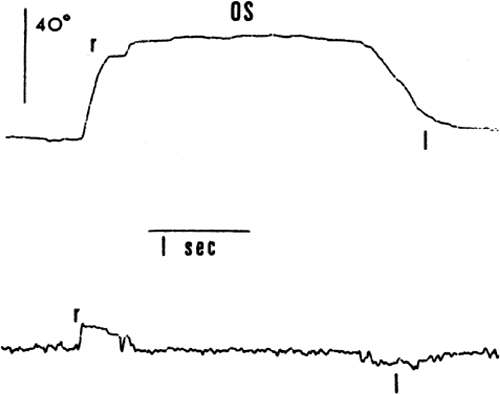 Figure 21.8 Electro-oculography recording of horizontal saccades in left eye of a patient with Duane syndrome, type I. Abduction saccades (L) are very slow (70 degrees/second), whereas adduction saccades (R) are moderately reduced in velocity in the upper tracing. Lower tracing: peak velocity. Source: Metz HS, Scott AB, Scott WE: Horizontal velocities in Duane’s syndrome. Am J Ophthalmol 80:901, 1975. Published with permission from the American Journal of Ophthalmology. Copyright by the Ophthalmic Publishing Company |
In type II Duane syndrome, average abduction saccades are generally normal in speed, but adduction saccadic velocity is markedly subnormal. The typical type III Duane syndrome has slowed saccades both medially and laterally, presenting a distinctive picture.
Restrictions
Restrictions limit the range of eye movement, but do not reduce saccadic velocity. The innervational input is not reduced; thus, where the eye is mechanically free to move, saccades are normally rapid.
Thyroid Ophthalmopathy
Limited elevation of one or both eyes, often accompanied by exophthalmos and eyelid retraction, is a common motility defect seen in patients with thyroid eye disease. Limitation of abduction, adduction, and depression may also be seen, in decreasing order of frequency. The forced traction test is invariably positive, most notably to upward gaze.
Upward and downward saccades, measured by electro-oculography, are normal in speed and are rapid (Fig. 21.9). This indicates that limitation of upward gaze is restrictive and not paretic, and this finding also applies to abnormalities of horizontal rotation. Using a more accurate search coil technique, Schworm et al.19 were unable to identify clinically relevant saccadic changes in the early stages of Graves’ ophthalmopathy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


