61 Robotic Surgery and Transoral Laser Surgery in Head and Neck • History • Indications • Advantages • Disadvantages • Setup • History • Advantages • Disadvantages • European Laryngological Society classification of endoscopic resection (Fig. 61.1) – Resection VF epithelium passing through the superficial layer of lamina propria – Resection of epithelium, Reinke space, and the vocal ligament – Resection of the VF down through vocalis muscle – Resection of the cord that extends from the vocal process to the anterior commisure ± internal perichondrium of the thyroid ala – Va: + contralateral vocal fold and anterior commissure – Vb: + arytenoids – Vc: + subglottis – Vd: + ventricle and false cords
61.1 Robotic Surgery in Head and Neck
 Da Vinci Robot
Da Vinci Robot
 1st ever robotic operation was a heart bypass in Leipzig, Germany, in 1998
1st ever robotic operation was a heart bypass in Leipzig, Germany, in 1998
 1st transoral resection by Weinstein/O’Malley at University of Pennsylvania, USA, 2004
1st transoral resection by Weinstein/O’Malley at University of Pennsylvania, USA, 2004
 Oropharyngeal, laryngeal, hypopharyngeal malignancy
Oropharyngeal, laryngeal, hypopharyngeal malignancy
 Parapharyngeal tumours
Parapharyngeal tumours
 Thyroid and parathyroid surgery
Thyroid and parathyroid surgery
 (Initial cadaveric studies show tongue base hypertrophy contributing to obstructive apnea may be an application for the robot)
(Initial cadaveric studies show tongue base hypertrophy contributing to obstructive apnea may be an application for the robot)
 Increased visualization and precision through limited access
Increased visualization and precision through limited access
 Transoral approach
Transoral approach
 Reduced surgical time
Reduced surgical time
 Shorter hospital stay
Shorter hospital stay
 Avoidance/dose reduction in chemo/RT
Avoidance/dose reduction in chemo/RT
 Expense
Expense
 Learning curve for surgeons and theatre staff
Learning curve for surgeons and theatre staff
 Limited software to run the robot
Limited software to run the robot
 No tactile feedback
No tactile feedback
 Surgeon’s console (in room with patient)
Surgeon’s console (in room with patient)
 Instrument cart with robot with 4 interactive robotic arms adjacent to patient
Instrument cart with robot with 4 interactive robotic arms adjacent to patient
 3 arms are holders for instruments such as scalpel, scissor, and cautery
3 arms are holders for instruments such as scalpel, scissor, and cautery
 1 arm is a camera (0° or 30°) with 2 lenses affording stereoscopic vision
1 arm is a camera (0° or 30°) with 2 lenses affording stereoscopic vision
 Surgeon looks via the wired vision cart at a high-definition 3D image on the console while using 2 foot- and 2 hand-controlled pedals that move the arms
Surgeon looks via the wired vision cart at a high-definition 3D image on the console while using 2 foot- and 2 hand-controlled pedals that move the arms
 Movements by the surgeon are converted into microscopic movements by the robot’s computer system
Movements by the surgeon are converted into microscopic movements by the robot’s computer system
 The range of movement is 540° of rotation
The range of movement is 540° of rotation
 Computerized motion scaling eliminates tremors and fatigue
Computerized motion scaling eliminates tremors and fatigue
 Process relies on human operator for all input
Process relies on human operator for all input
 Future developments include remote operating, i.e., the patient and robot are in a different place to the surgeon; role in metastatic SCC in the neck; and development of haptic feedback systems
Future developments include remote operating, i.e., the patient and robot are in a different place to the surgeon; role in metastatic SCC in the neck; and development of haptic feedback systems
61.2 Transoral Laser Surgery in Head and Neck
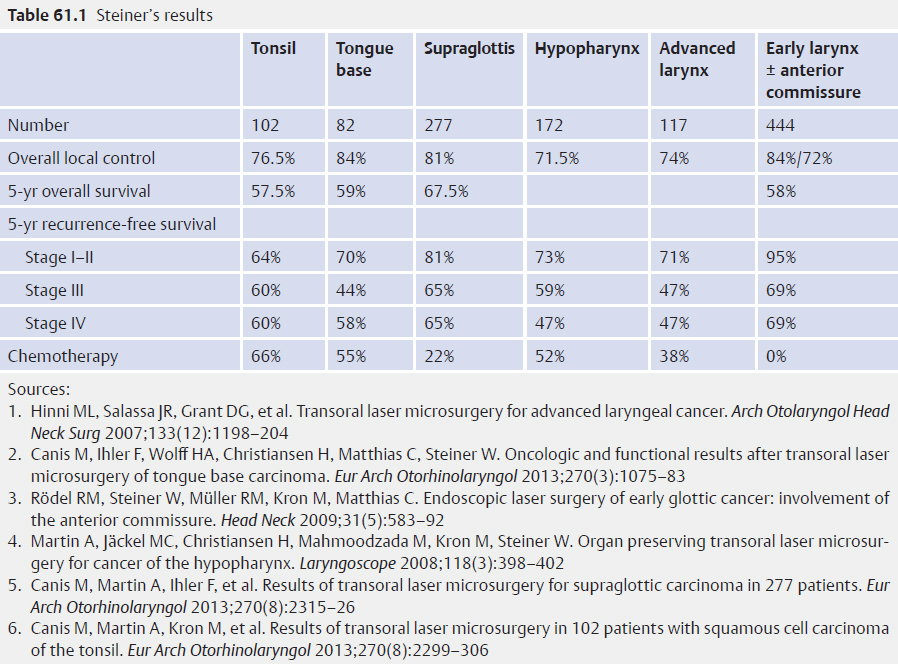
 1985 Steiner, Ambrosch: University of Göttingen, Germany
1985 Steiner, Ambrosch: University of Göttingen, Germany
 See Table 61.1
See Table 61.1
 Less local recurrence
Less local recurrence
 Less salvage laryngectomy
Less salvage laryngectomy
 Organ sparing
Organ sparing
 Morbidity/complication rate lower
Morbidity/complication rate lower
 Laser injury
Laser injury
 Learning curve
Learning curve
 Type I—subepithelial cordectomy
Type I—subepithelial cordectomy
 Type II—subligamental cordectomy
Type II—subligamental cordectomy
 Type III—transmuscular cordectomy
Type III—transmuscular cordectomy
 Type IV—total cordectomy
Type IV—total cordectomy
 Type V—Extended cordectomy
Type V—Extended cordectomy
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


