Robotic Resection of Recurrent Nasopharyngeal Cancer
William Ignace Wei
INTRODUCTION
The primary treatment modality for early-stage nasopharyngeal carcinoma (NPC) is radiotherapy and for advanced-stage disease, concomitant chemotherapy and radiation. With the use of intensity-modulated radiotherapy in recent years, the local cancer control rate has improved, while the long-term morbidity has decreased. Despite the better treatment results, there are still a few patients who have residual or recurrent NPC after the initial therapy. Further external radiotherapy in the management of these patients is associated with significant complications especially in the long term and little hope that a modality that failed the first time would succeed the second time. Stereotactic radiation and brachytherapy have been applied with favorable outcomes for some. These types of radiation are only effective when the exact extent of the cancer has been determined accurately with imaging studies so that the cancer could be completely included in the radiation field. This precise determination of the edge of the cancer might be difficult for some patients. The other alternative for management of these residual or recurrent cancer with a curative intention is surgical resection.
Anatomically, the nasopharynx is located in the center of the head; it is over 10 cm from the skin surface from all sides. It is difficult to get adequate exposure for removal of cancer at this site. Various approaches have been described in the literature, and they all require external incisions, and there are associated morbidities. An endoscopic approach for transnasal resection of small tumors in the nasopharynx has been reported. The instruments currently available for endoscopic transnasal surgery when employed for oncologic resection of these tumors have certain limitations. It is difficult to achieve an en bloc resection of the tumor under direct vision especially when the tumor extends to involve the lateral wall of the nasopharynx.
In recent years, the efficacy of transoral robotic surgery in Otolaryngology—Head and Neck Surgery has been established. The da Vinci robot has been used effectively for resection of malignant tumors arising in the oropharynx, supraglottic larynx, and superior hypopharynx. The feasibility of the surgical robot employed for resection of pathologies at the skull base and the nasopharynx has been described. The first successful application for resection of a small recurrent cancer in the nasopharynx has also been reported in recent years.
HISTORY
It is essential to know the stage of the NPC on initial presentation and also the form of therapy such as radiation alone or concomitant chemoradiation. The duration and dosage of radiation should be noted and if chemotherapy was given, the chemotherapeutic agent and the dosages recorded. The time when recurrence was detected should be noted, and any therapy for the management of the recurrence should be documented. This might include further external beam radiotherapy, stereotactic radiation, or brachytherapy. Any medical comorbidities should be recorded.
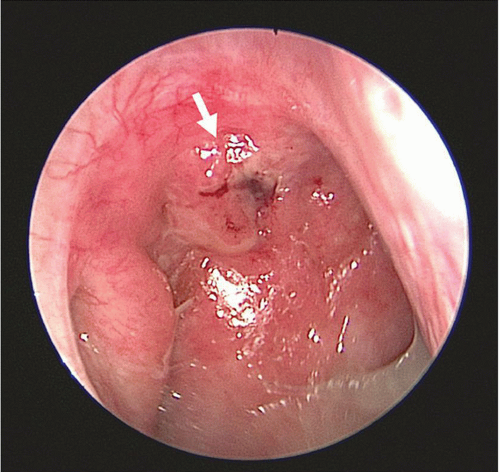 FIGURE 34.1 A small recurrent cancer seen through a 0-degree endoscope located at the superior aspect of right lateral wall of the nasopharynx (arrow). |
PHYSICAL EXAMINATION
A complete physical examination is essential to exclude metastases to the cervical lymph nodes and to other organs. Palpation of the neck and abdomen should be carried out, and if there is any doubt, an ultrasound examination of these regions should be performed. All suspicious lesions should be investigated further with a fine needle aspiration biopsy or even with positron emission tomography-computed tomography (PET-CT).
Endoscopic Examination
The nasopharynx should be thoroughly examined with both 0-degree- and 30-degree-angled Hopkins rigid endoscopes to ascertain the extent of the tumor (Fig. 34.1). Biopsies around the cancer should be carried out to determine the edges of the tumor and to guide the extent of the resection.
Salvage resection of the primary tumor should only be done when there are no distant metastases. For regional metastasis, a separate surgical salvage procedure such as a neck dissection can be planned either at the same session with the resection of the primary cancer or at a later date.
PREOPERATIVE PLANNING
Imaging Studies
Magnetic resonance imaging (MRI) of the nasopharynx is indicated to see the deep extent of the tumor, its extension in the submucosa of the nasopharynx and paranasopharyngeal space (Fig. 34.2). Its proximity to the
internal carotid artery can also be evaluated with the contrast MRI. CT is also indicated if there is any suspicion that the cancer has infiltrated bone, such as the pterygoid plates, the anterior wall of the sphenoid sinus, and the clivus. Either of these imaging studies will demonstrate whether the tumor has involved the paranasal sinuses.
internal carotid artery can also be evaluated with the contrast MRI. CT is also indicated if there is any suspicion that the cancer has infiltrated bone, such as the pterygoid plates, the anterior wall of the sphenoid sinus, and the clivus. Either of these imaging studies will demonstrate whether the tumor has involved the paranasal sinuses.
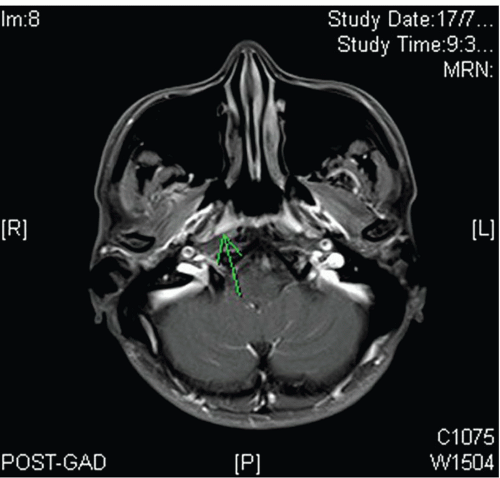 FIGURE 34.2 Magnetic resonance imaging (MRI) of the same cancer (arrow) demonstrates that it is only in the fossa of Rosenmüller and has not extended to the paranasopharyngeal space. |
INDICATIONS
The bulk of the recurrent NPC should be at the inferior aspect of either the lateral wall or the posterior wall of the nasopharynx. In general, tumor bulk should be <2 cm in diameter and involve only one Eustachian tube orifice. The tumor should only involve the mucosa or the muscular wall of the nasopharynx. It should not be extending into the paranasopharyngeal space or beyond the pharyngobasilar fascia and not lying close to the internal carotid artery.
CONTRAINDICATIONS
The limitations of employing the robot to carry out resection of the recurrent NPC are those related to the tumor and the clinical condition of the patient. For extensive cancers involving both Eustachian tube orifices and for infiltrative tumors involving the paranasopharyngeal space or close to the internal carotid artery, an anterolateral approach should be carried out to ensure tumor clearance. For those cancers that have extended into the sphenoid sinus or infiltrated the clivus or the pterygoid plates, resection with the robot is unlikely to remove all of the cancer with a clear margin. Robotic resection of the recurrent NPC is done transorally after splitting the palate; thus, the patient should have no trismus and no previous palate surgery. The tongue and intraoral tissue should be pliable and able to stand some stretching. Needless to say, the patient should be well enough medically to tolerate general anesthesia for 3 to 4 hours.



